
Abstract
Aim
Evidence suggests low-grade inflammation (LGI) to be associated with multimorbidity. Furthermore, there are links between inflammation markers, physical activity (PA), and labour market participation. The aims of this study were to examine the association between PA and LGI in people with multimorbidity and if this association was moderated by self-reported labour market attachment.
Methods
Cross-sectional data were collected in the Lolland-Falster Health Study (LOFUS) from 2016–2020. We included 1,106 participants with multimorbidity and valid accelerometer data. PA was measured as the average counts per minute (CPM) per day during wake time and split in time spent in moderate to vigorous intensity (MVPA) and light intensity (LPA). Degree of inflammation was determined by high sensitive C-reactive protein (hsCRP) level. Associations were investigated using multiple logistic regression analyses, stratified by labour market attachment.
Results
The odds of having LGI was higher with lower amount of daily LPA. The highest odds of LGI was observed for CPM < 200 per day (odds ratio (OR) 2.55; 95% confidence interval (CI) 1.46–4.43), MVPA < 15 minutes per day (OR 2.97; 95 % CI 1.56–5.62), and LPA < 90 (OR 2.89; 95 % CI 1.43–5.81) with the reference groups being CPM ≥ 400 per day, MVPA ≥ 30, and LPA ≥ 180 min per day, respectively. We could not preclude an interaction between LPA and labour market attachment (p = 0.109).
Conclusion
PA recommendations should be developed with attention to people with chronic diseases, who may experience barriers to reach PA at high intensities. People with no labour market attachment may benefit from primary and secondary prevention of multimorbidity.
Keywords
Introduction
More than half of individuals diagnosed with a chronic disease are affected by two or more chronic diseases – commonly referred to as multimorbidity. 1 The prevalence of multimorbidity is estimated to be 33% in the general population, 2 and with an expected increase in the prevalence, 3 multimorbidity is considered to be one of the next global health challenges. 4 Multimorbidity is associated with age and a range of adverse lifestyle factors, such as smoking, high alcohol intake, and physical inactivity. 5 Moreover, a socioeconomic gradient in the prevalence of multimorbidity has been observed, i.e. the prevalence of multimorbidity is higher among people with lower educational levels, lower incomes, and people in unemployment.6,7 Additionally, low-grade inflammation (LGI), defined by a high level of high sensitive C-reactive protein (hsCRP) of 3-10 mg/L, 8 has been found to be associated with chronic diseases and multimorbidity. 9 But, socioeconomic factors also seem to play a role in CRP levels in the general population, e.g. employed individuals are shown to have lower CRP levels than unemployed. 10 However, the association between employment status and CPR is not consistent. 11
Physical activity (PA) appears safe and beneficial for the physical and psychosocial health of people with multimorbidity. 12 PA is also shown to reduce inflammatory markers, such as CRP, 13 and protect against chronic diseases associated with LGI, such as diabetes and cardiovascular diseases.14,15 Furthermore, international guidelines recommend at least 150-300 minutes moderate-intensity aerobic PA or at least 75-150 minutes vigorous-intensity aerobic PA per week for adults with and without chronic diseases. 16 Despite the beneficial effects of PA on inflammation and chronic diseases, people with multimorbidity often fail to adhere to PA guidelines, however, knowledge on PA levels among people with multimorbidity is limited. 17 Technically measured PA is considered more accurate than self-reported PA.18,19,20,21 Therefore, studies investigating PA levels among people with multimorbidity may benefit from including such measurements.
Further understanding of the complex mechanisms of multimorbidity and potential confounders from external socioeconomic factors, like labour market attachment, is needed to enhance our identification of ways to treat and prevent the growing number of people with multimorbidity. Therefore, the aims of this study were to examine the association between technically measured PA and LGI in people with multimorbidity adjusted for potential confounders, and if this association was moderated by labour market attachment. We hypothesized that a lower level of technically measured PA, would increase the odds of LGI among people with multimorbidity. Furthermore, we assumed that the odds of LGI by a lower PA level would be higher among individuals who were not attached to the labour market compared to those who are attached.
Methods
Context, study design, data collection, and study population
Cross-sectional data were collected in the Lolland-Falster Health Study (LOFUS) from February 8, 2016 to February 13, 2020. Lolland-Falster is located in the south-eastern part of Denmark where income is lower and life expectancy is shorter than in the average Danish population.22,23 It is a mixed rural-provincial area with approximately 100,000 inhabitants. 22
LOFUS is a household-based prospective cohort study including people of all ages. Using the unique civil registration numbers in the Danish Civil Registration System, 24 people aged 18 or above were randomly selected. The entire household of these randomly selected inhabitants was allocated either to an invited group or to an uninvited, non-contacted control group. 22 The data collection encompassed questionnaires, physical examination, and biological samples. 22 In total, 18,949 individuals aged 0-96 years participated in LOFUS. Between 1 February 2017 and 30 November 2018, a subsample of LOFUS participants were invited to have their PA measured by using a dual accelerometer system. 25 In this subsample, the inclusion criteria for participation in the accelerometer assessment was that at least one adult and one child aged 17 or below from a participating household should agree to wear accelerometers. This criterion was set because the first LOFUS research project needing accelerometer data aimed at examining family patterns of physical activity. Later, from 1 December 2018 to 13 February 2020, all LOFUS participants were eligible for inclusion in the accelerometer assessments. Subjects who could not walk, e.g. young toddlers or wheelchair users, were excluded from the collection of accelerometer data. 26 This study included all adult LOFUS participants with available accelerometer data. The inclusion criteria for the present study were 18-79 years of age, participation in the accelerometer subsample, and having an accelerometer wear time of ≥8 hours per day for a minimum of four days, 26 as well as having multimorbidity, i.e. a minimum of two self-reported chronic diseases. The definition of multimorbidity was based on previous work on multimorbidity1,5 and chronic diseases were selected among those available in the LOFUS dataset and based on previous literature. 27
We expected movement patterns and PA intensity measurement among the oldest citizens to differ markedly from younger adults. Furthermore, the PA intensities we used in this study were tested among a younger population. 28 Therefore, individuals aged 80 years or above were excluded to ensure that the cutoffs, used to estimate PA levels, were reliable for the study population. 28
Exposure variables
The PA outcomes used in the present study were estimated as the average Actigraph counts per minute (CPM) per day during wake time, time spent in moderate to vigorous intensity (MVPA), and time spent in light intensity (LPA). MVPA was estimated as the average time spent in 3522 CPM or above per day, whereas LPA was estimated as the average time spent in the intensity range from 100-3521 CPM per day. 26 The specific intensity thresholds for MVPA and LPA were established using an internally conducted validation experiment described in detail elsewhere. 28 This study suggested that an age independent moderate intensity cut-point can be defined as the average count for walking at self-selected speed irrespective of age, whereas the vigorous cut-point is defined as the count threshold at which most subjects are considered running. 28
In all analyses, CPM was categorized as <200, 200-399.99, and ≥400 minutes per day, MVPA as <15, 15-29.99, and ≥30 minutes per day, and LPA as <90 minutes, 90-179.99, and ≥180 minutes per day.
Outcome variable
Covariates
Selection of covariates (potential confounders) was based on findings in the literature and included sociodemographic factors (age, sex, labour market attachment, civil status, and education),31,32 number of diseases,9,33,34 health and lifestyle factors (diet, smoking, Body Mass Index (BMI), waist circumference, self-rated health, sleep, stress, and alcohol consumption).31,35–40 Use of anti-inflammatory/potentially anti-inflammatory medication was included as a confounder, as anti-inflammatory medication can improve individuals with chronic diseases’ ability to participate in physical activities (e.g. anti-inflammatory drugs are commonly used by athletes with asthma), 41 and because anti-inflammatory drugs are directly linked to CRP-levels. 42 Data on the covariates was obtained from self-administered questionnaires. 23
Labour market attachment was dichotomized into 1) ‘attached’ (including: ‘in labour’, ‘studying or training’, and ‘caregivers or work in home’) and 2) ‘not attached’ (including: ‘unemployed’ and ‘out of the labour market’). 43
Alcohol consumption was measured by asking participants: “How often do you drink five units or more at one occasion?” with four response options ranging from ‘never’ to ‘daily’. We trichotomized the response options into 1) ‘rarely’ (including: ‘never’ and ‘rarely’), 2) ‘weekly’, and 3) ‘daily’. 49
Smoking was measured by asking participants: “Do you smoke?” with five response options ranging from ‘never smoked’ to ‘yes, every day’. Response options were dichotomized as 1) ‘smoker’ (including: ‘yes, every day’, ‘yes, at least one time per week’, and ‘yes, less than every week’) and 2) ‘non-smoker’ (including: ‘ex-smoker’ and ‘never-smoker’). 49
Self-perceived diet quality was measured by asking participants to rate their dietary habits on a 5-point scale, ranging from ‘very healthy’ to ‘very unhealthy’. We dichotomized the response options into 1) ‘healthy’ (including: ‘very healthy’, ‘healthy’, and ‘somewhat healthy’) and 2) ‘unhealthy’ (including: ‘unhealthy’ and ‘very unhealthy’). 50
Ethics
Region Zealand's Ethical Committee on Health Research (SJ-421) approved LOFUS. LOFUS is registered in the Danish Data Protection Agency (REG-024-2015). The present study is also registered in the Danish Data Protection Agency (REG-130-2020). LOFUS is registered in Clinicaltrials.gov (NCT02482896). All participants provided written informed consent. 23
Statistical analyses
Characteristics of the study sample (n = 1,106) distributed on inflammation level calculated by high sensitive C-reactive protein (hsCRP). Mean values with standard deviation (±SD) or number of participants with prevalence are presented.

CPM: counts per minute; MVPA: moderate to vigorous physical activity; LPA: light physical activity; hsCRP: high sensitive C-reactive protein; LGI (Low-grade inflammation; BMI: Body Mass Index.
aLow risk (waist circumference for women <80 cm and for men <94 cm).
bIncreased risk (waist circumference for women ≥80 cm and for men ≥94 cm.
Odds of having low-grade inflammation (LGI) (hsCRP 3–10 mg/L) among participants with different levels of physical activity (CPM, MVPA and LPA). Results are presented as OR with corresponding 95% CI.
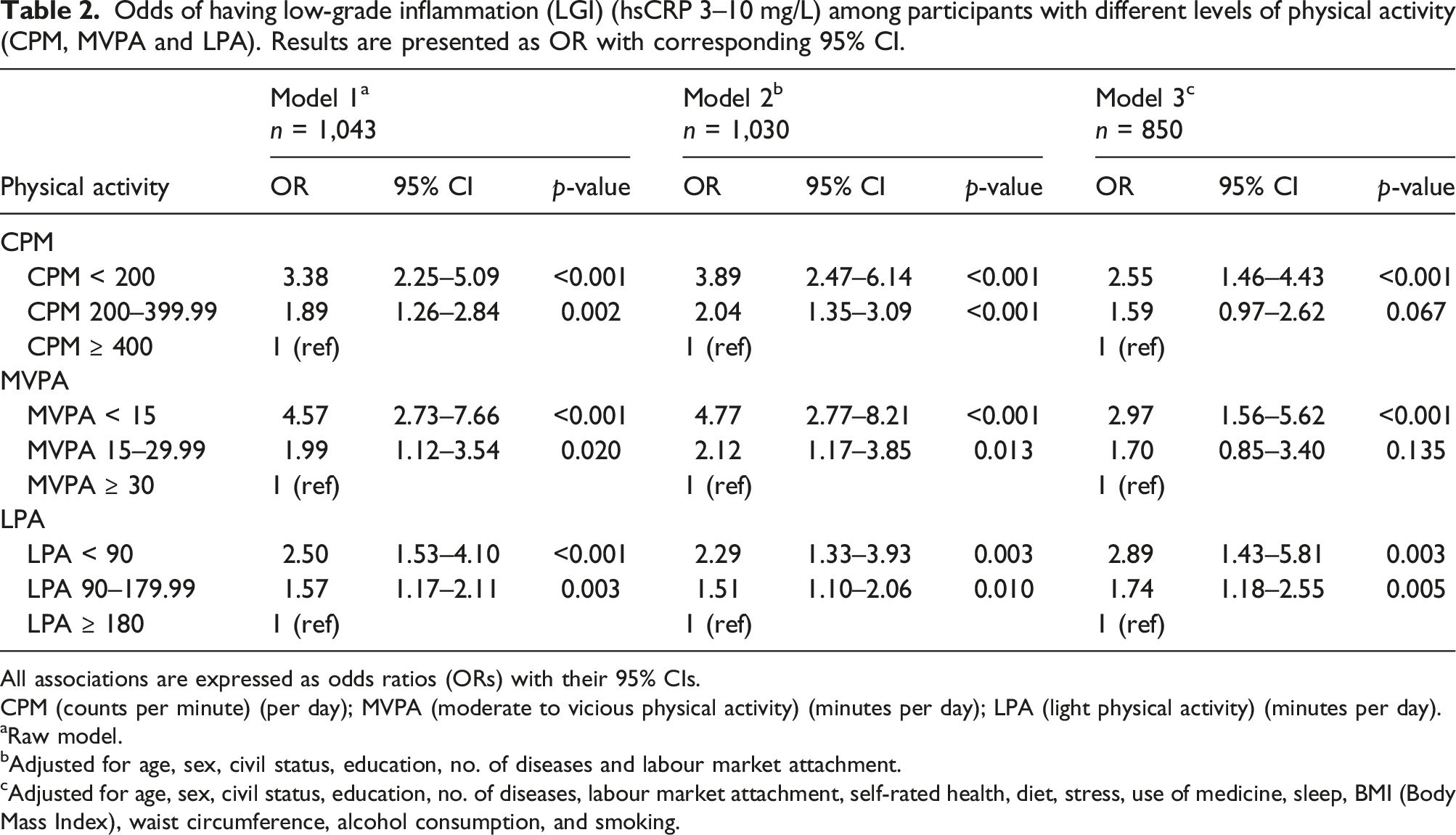
All associations are expressed as odds ratios (ORs) with their 95% CIs.
CPM (counts per minute) (per day); MVPA (moderate to vicious physical activity) (minutes per day); LPA (light physical activity) (minutes per day).
aRaw model.
bAdjusted for age, sex, civil status, education, no. of diseases and labour market attachment.
cAdjusted for age, sex, civil status, education, no. of diseases, labour market attachment, self-rated health, diet, stress, use of medicine, sleep, BMI (Body Mass Index), waist circumference, alcohol consumption, and smoking.
Odds of having low-grade inflammation (LGI) (hsCRP 3–10 mg/L) among participants with different levels of physical activity (CPM, MVPA and LPA), stratified on labour market attachment. Results are presented as OR with corresponding 95% CI. Interaction terms are presented as p-values.
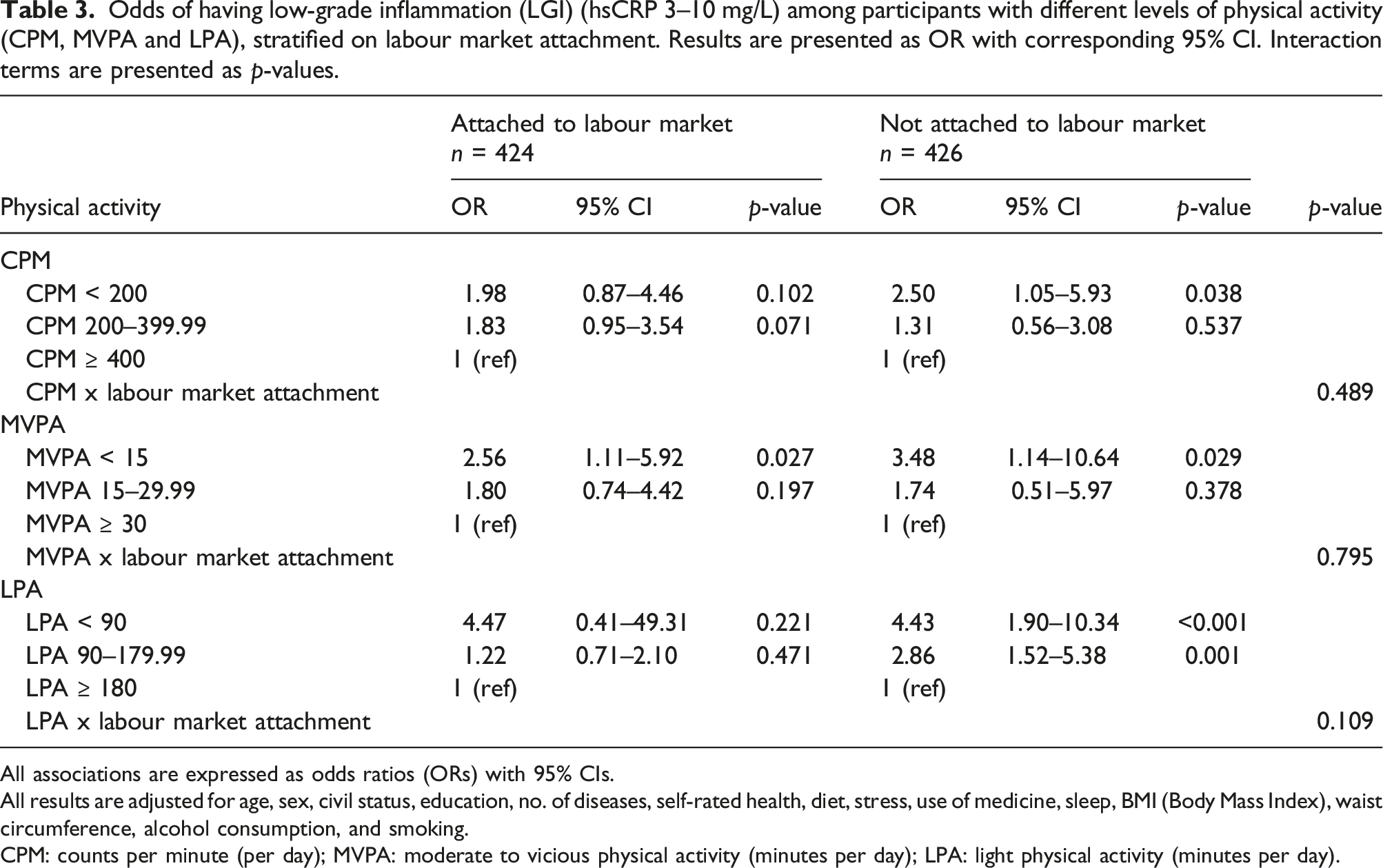
All associations are expressed as odds ratios (ORs) with 95% CIs.
All results are adjusted for age, sex, civil status, education, no. of diseases, self-rated health, diet, stress, use of medicine, sleep, BMI (Body Mass Index), waist circumference, alcohol consumption, and smoking.
CPM: counts per minute (per day); MVPA: moderate to vicious physical activity (minutes per day); LPA: light physical activity (minutes per day).
Results
In total, 18,949 (35.6%) of the 53,313 invited individuals from Lolland-Falster agreed to participate in LOFUS. Based on the inclusion criteria for this study, a total of 17,843 participants were excluded, ending up with a study population of 1,106 participants (Figure 1). Flow chart for the study on the association between PA, LGI, and labour market attachment in people with multimorbidity, Lolland-Falster Health Study (LOFUS).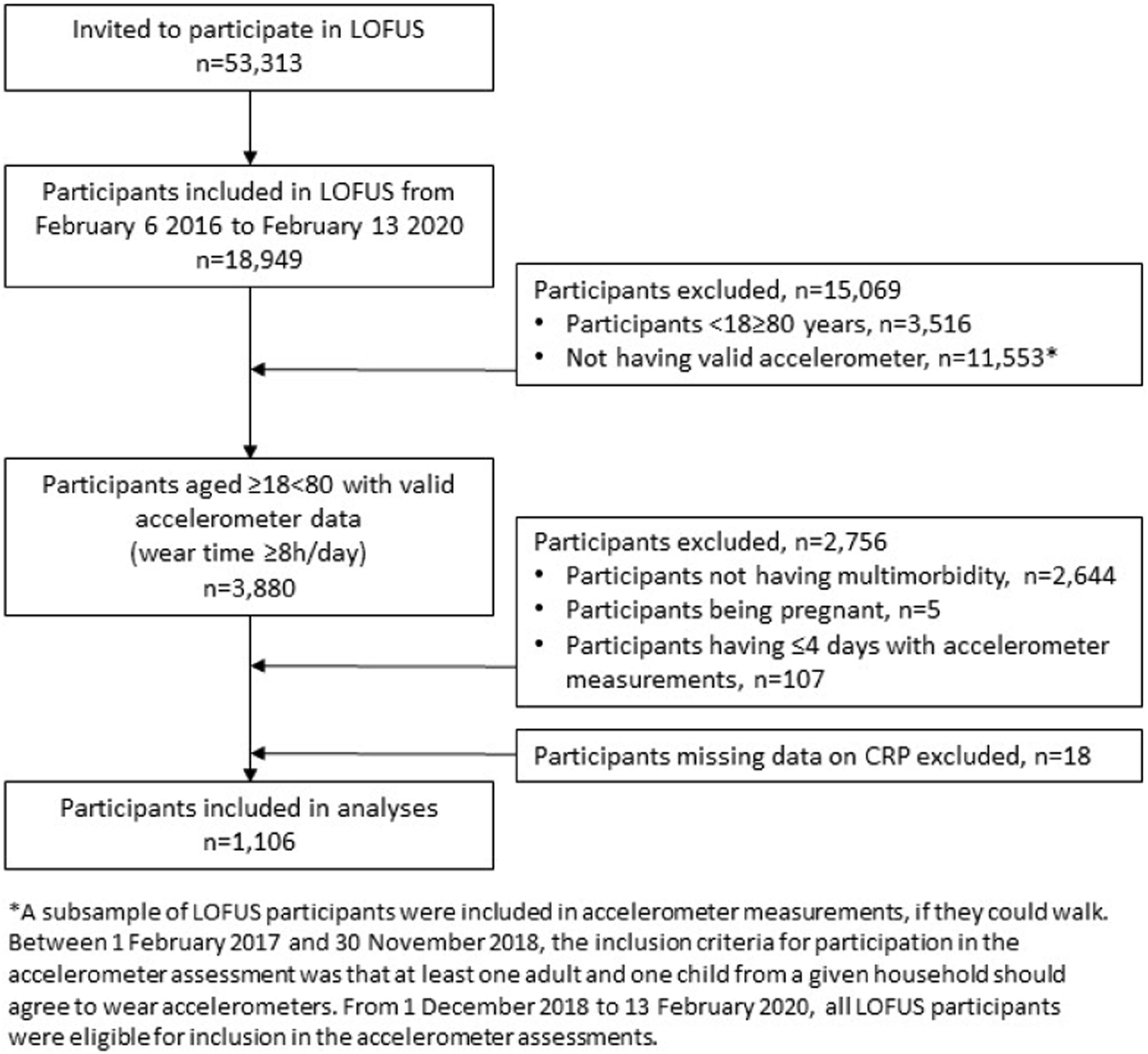
Table 1 shows the explanatory variables according to levels of inflammation. We found no evidence of a difference in participants across the three groups of hsCRP levels in terms of age (p = 0.627), accelerometer wear hours per day (p = 0.602), number of wear days (p = 0.292), education (p = 0.063), self-reported health (p = 0.072), sleep (p = 0.952), stress (p = 0.230), and alcohol consumption (p = 0.255) (Table 1). A statistically significant difference between participants in the three groups of hsCRP levels was observed for the exposure variables, i.e. CPM (p < 0.001), MVPA (p < 0.001), LPA (p < 0.001), and the remaining variables, i.e. civil status (p < 0.003), sex (p = 0.010), no. of chronic diseases (p = 0.021), labour market attachment (p = 0.007), use of medicine (p < 0.001), BMI (p < 0.001), waist circumference (p < 0.001), smoking (p < 0.001), and diet (p = 0.006) (Table 1).
For all PA outcomes, the odds of having LGI increased with lower levels of PA, however, for CPM and MVPA only the lowest levels of PA were statistically significant (Table 2). The odds of LGI increased for every 90 minutes decrease in LPA per day (Table 2). The highest odds of LGI were observed for CPM < 200 per day (OR 2.55; 95% CI 1.46-4.43), MVPA < 15 minutes per day (OR 2.97; 95 % CI 1.56-5.62), and LPA < 90 minutes per day (OR 2.89; 95 % CI 1.43-5.81) with the reference groups being CPM ≥ 400 per day, MVPA ≥ 30, and LPA ≥ 180 minutes per day, respectively.
We found no evidence of statistical interactions between CPM (p = 0.489) and MVPA (p = 0.795) and labour market attachment, but we cannot rule out the possibility of interaction between LPA and labour market attachment (p = 0.109) (Table 3). 52
When stratified on labour market attachment, we found statistically significant higher odds of LGI for MVPA<15, independent of labour market attachment, and higher odds of LGI for CPM<200 among those who were not attached to the labour market (Table 3). Furthermore, the odds of LGI were higher the less time spent in LPA, however, the results were only statistically significant for those who were not attached to the labour market although the pattern of association were similar to those attached to the labour market.
Discussion
This study examined the association between technically measured PA and LGI among people with multimorbidity, and if this association was moderated by labour market attachment. We found that a low level of PA was associated with higher odds of LGI among participants with multimorbidity, especially among those who are not attached to the labour market.
Comparison with previous findings
PA is safe and beneficial for the physical health in people with multimorbidity. 12 Previous studies show higher levels of PA to be associated with lower levels of CRP in the general adult population13,14,53 and among people with chronic diseases.54,55 This is in line with our results showing lower odds of LGI by higher levels of PA in people with multimorbidity.
Our study showed that a low level of MVPA<15 minutes per day was associated with higher odds of LGI with MVPA ≥30 minutes per day being the reference. The Danish health authorities recommend ≥30 minutes of MVPA per day, 56 and 71% of the general adult population reports to follow this recommendation. 49 In our study sample, however, only 15% of the participants performed MVPA for ≥30 minutes per day. Similarly, a recent study found that only 32% of older adults with multimorbidity lived up to PA recommendations. 57 Such findings indicate that people with multimorbidity might experience barriers to reach these duration and intensity levels of PA.
Adherence to recommended PA levels is associated with a significant reduction in the risk of chronic diseases, and is thereby a means of primary and secondary prevention of multimorbidity. 57 Furthermore, adherence to PA recommendations is associated with sex, socioeconomic status, smoking habits, diet, and BMI, and among people with multimorbidity, those belonging to the more deprived socioeconomic groups are more likely to not adhere to PA guidelines. 57 In this study, the participants did all have multimorbidity and were recruited from Lolland-Falster – a socioeconomically deprived area. 22 Thus, it is not surprising that the adherence to PA recommendations in our study population was relatively low.
As previously stated, WHO recommends at least 150-300 minutes moderate-intensity aerobic PA or at least 75-150 minutes vigorous-intensity aerobic PA per week for adults with and without chronic diseases to gain health benefits. 58 Our study shows lower odds of LGI with longer durations of LPA. This is in line with the WHO recommendations stating that sedentary time should be replaced with PA of any intensity (including light intensity) to gain health benefits, 58 which are supported by a study showing as little as 10 minutes of brisk walking per day to associate with longer life expectancy. 59
Finally, our results indicate that labour market attachment may moderate the association between LPA and LGI, although the two strata show similar patterns of associations between PA and LGI, being the less PA performed the higher odds for LGI. Yet, the results were only statistically significant for those not attached to the labour market. These findings are in line with previous findings showing higher levels of CRP among people who are unemployed. 10 Thus, our results highlight that not only are the amount and intensity of PA associated with the odds of LGI among people with multimorbidity, external factors like labour market attachment also seem to play an important role in this association. One explanation may be, that people in lower socioeconomic positions, e.g. those who are not attached to the labour market, are more vulnerable to exposures from risk factors, such as inactivity, for various diseases. 60 However, a recent study suggested that a binary categorization of unemployment versus employment does not capture the complexities of (un)employment. 11 Thus, more knowledge is needed about labour market attachment subgroups and CRP levels.
Strengths and limitations
This study is strengthened by the use of accelerometer data to assess PA in people with multimorbidity. By using technically PA outcomes instead of the alternative of self-reported data, we have minimized the risk of information bias and thereby the risk of differential misclassification of dependent and independent variables. The drawback is though, that the voluntary participation in accelerometer measurement may have increased the risk of selection bias. E.g. it is possible that healthier individuals were more likely to agree to wear accelerometers, leading to weaker estimates of the association between PA and LGI. However, previous studies using large health surveys suggest that biased participation may not affect the associations between variables. 61
Another strength of this study is the population-based sampling. The large study sample provided statistical power to investigate the association between PA and LGI among a subgroup of participants in LOFUS with multimorbidity. Furthermore, the inclusion of participants in LOFUS, who all came from rural-provincial areas with lower socioeconomic and health status than the average population, add to findings from previous Danish cohort studies in rural-provincial areas. However, in the analyses, stratified by labour market attachment, the sample size of the strata was relatively low, thus, the results should be interpreted with caution.
We adjusted for several demographic, socioeconomic, and health factors previously shown to be associated with PA and inflammation, which we expected to some extent to reduce the risk of unmeasured confounding. But, because of our cross-sectional design, we cannot preclude a bidirectional relationship between the included variables in terms of reverse causation; that is, it is possible that LGI affected the level of PA among participants. However, a review examining the effect of PA on chronic inflammation reported consistency in large population-based studies showing an inverse association between inflammation and PA, and found that small-scale intervention studies supported that PA diminishes inflammation. 14 Moreover, a review and meta-analysis of RCTs supported that PA may have a positive effect on reduction of CRP. 13
Another limitation is that the subgroup of participants who were not attached to the labour market included both those who were ‘unemployed’ and ‘out of the labour market’ with the latter also including people who were retired. Thus, this subgroup includes participants who are not attached to the labour market due to different reasons. This categorization may have led to residual confounding. However, regardless the cause, participants who are not attached to the labour market are comparable in terms of not being exposed to occupational PA, which has previously been stated as one of four central domains of PA assessment. 62
This study did not include all chronic diseases. Our results can therefore not be generalized to all people with multimorbidity. It is possible that inclusion of more diseases would have led to different results. However, this is a general limitation on studies in multimorbidity since definitions of multimorbidity used in the literature have varied widely 63 and guidelines specifying diseases to include in multimorbidity research were not published until 2022, which was after the LOFUS data were collected. 27
Practical implications
As the prevalence of multimorbidity is increasing and considered to be a major health priority, it is crucial to consider effective ways to prevent and treat chronic diseases and develop ways to avoid serious health consequences among people with chronic disease. 4 Adherence to PA guidelines is previously identified as a means of primary and secondary prevention of multimorbidity, but, individuals with multimorbidity are more likely to not adhere to PA guidelines. 17 Our results showed that both the amount and intensity of PA were associated with the odds of LGI among people with multimorbidity. Therefore, adjusting existing guidelines according to amounts and intensities that are reachable for people with chronic diseases or various abilities to do PA at different levels may be one method for secondary prevention of multimorbidity. Furthermore, WHO recommendations state that sedentary time should be replaced with PA of any intensity (including light intensity) to gain health benefits. Such recommendation may be relevant to incorporate in future preventive interventions.
Our results also showed that labour market attachment seem to play an important role in the association between LPA and LGI. This knowledge can be used to identify target groups for preventive interventions. Furthermore, our findings highlight the importance of obtaining information regarding patients’ socioeconomic conditions and job situation in the clinical setting to target treatment – especially treatments where changes in lifestyle markers, such as PA, are involved.
Conclusion
This study shows that low amounts of CPM and MVPA, were associated with higher odds of LGI among people with multimorbidity. Our study also shows that higher levels of LPA is associated with lower odds of LGI, especially among those who are not attached to the labour market. This knowledge is important for development of PA recommendations for people who might experience barriers to reach PA at high intensities.
Supplemental Material
Supplemental Material - The association between physical activity, low-grade inflammation, and labour market attachment among people with multimorbidity: A cross-sectional study from the Lolland-Falster Health Study, Denmark
Supplemental Material for The association between physical activity, low-grade inflammation, and labour market attachment among people with multimorbidity: A cross-sectional study from the Lolland-Falster Health Study, Denmark by Vivian Rueskov Poulsen, Linda Kjær Fischer, Mette Aadahl, Ole Steen Mortensen, Søren T Skou, Lars Bo Jørgensen, Randi Jepsen, Anne Møller, Therese Lockenwitz Petersen, Jan Christian Brønd, Lars Tang and Mette Korshøj in Comparative Political Studies
Footnotes
Author contributions
VRP drafted the manuscript and conducted the final analyses. LKF initiated and designed the study and planned and conducted the initial analyses. MK designed the analysis including labour market attachment, contributed to interpret the results and to review and revise the manuscript. RJ was responsible for the data collection. STS, MA, LBJ, OSM, AM, TLP, JCB, and LT provided input on study design and methods, and critically reviewed and provided feedback on the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: STS is associate editor of JOSPT, and has received personal fees from Munksgaard and TrustMe-Ed, outside the submitted work. Furthermore, he is co-founder of GLA:D®, a not-for profit initiative hosted at University of Southern Denmark aimed at implementing clinical guidelines for osteoarthritis in clinical practice.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: STS is currently funded by a program grant from Region Zealand (Exercise First) and two grants from the European Union’s Horizon 2020 research and innovation program, one from the European Research Council (MOBILIZE, grant agreement No 801790) and the other under grant agreement No 945377 (ESCAPE). LBJ and LHT are funded by grants from Region Zealand (Project: Exercise First) and The Danish Health Confederation through the Development and Research Fund for financial support (project no. 2703). LHT is further funded by a grant from Naestved-Slagelse-Ringsted Hospitals research fund, Denmark (project no. A1277).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.