
Abstract
Background
Multimorbidity is a group of conditions, it has significant impact on the population as a whole, resulting in lower quality of life, higher mortality, frequent use of medical services, and consequently higher healthcare costs. The objective of this study is to document the prevalence of common multimorbidity and its associated risk factors among population of Mechinagar Municipality.
Methods
Community-based cross-sectional study was conducted where selected multimorbidity were assessed in selected areas of Mechinagar municipality of Jhapa District . Systematic random sampling technique was used to select 590 adult participants from three pre-defined pocket areas. Pre-designed semi-structured multimorbidity assessment questionnaire for primary care (MAQ-PC)was used to assess prevalence of multimorbidity. Multiple logistic regression was conducted to identify the strongest determinants of multimorbidity.
Results
The prevalence of multimorbidity was 22.4%.Hypertension, Diabetes mellitus and COPD was seen in 39.2%, 7.8.% and 4.4% of the participants respectively . Participants with advancing age i. e. 40-49yrs were 12.62 times (AOR) more likely to have multimorbidity compared to their counterparts who were 20-29yrs old( p=<0.01,CI3.01-15.28) after adjusting for occupation, physical activity and family history of kidney disease. Working individuals, Physical inactivity and positive family history of kidney disease were the strongest determinates of multimorbidity.
Conclusions
The study revealed that participants with increasing age, working individuals, physical inactivity and family history of kidney disease were more vulnerable of having multimorbidity. The findings of our study indicate need of intervention strategies and community-based health promotion programs in reducing burden of chronic disease among adult population.
Introduction
Multimorbidity is defined as the simultaneous occurrence of two or more chronic health conditions in the same person, without defining a primary disease.1–3 Multimorbidity is a group of conditions, rather than just the presence of multiple diseases. This health condition has a profound impact on the population's well-being, resulting in a reduced quality of life, increased mortality rate, frequent use of medical services, and ultimately higher healthcare costs. 4 Multimorbidity increases the complexity of managing and preventing these conditions, in part because those who have several diseases are more likely to experience negative health effects.
The existing understanding of multimorbidity is mainly focused on high income countries research finding a high prevalence ranging from 30% among all adults to 60% in 65±74 years old. However, there has been an increase in the prevalence of multimorbidity among people below the age of 65 year. 5 In fact, originally considered a geriatric trend, some recent studies have shown that younger adults demonstrate a substantial prevalence of multimorbidity. 6 In low and middle income countries, the age of onset of non-communicable disease (NCD) is younger than in high income countries and because of their early age of onset, premature deaths are more. 7
Globally, cardiovascular diseases (CVDs), chronic respiratory diseases, diabetes and cancer are the four major NCDs, and this is no different in the South East Asia. 3 In the region, 62% of all deaths are due to NCDs accounting for 9 million persons. 8 Given the circumstances and patterns of emerging non-communicable diseases, we believe that NCDs have developed into a significant public health issue for Nepal that should be handled with prudence in terms of preventative healthcare as well as early diagnosis, screening, and treatment. Various studies results suggested that several factors including age, gender, education, income, employment, obesity, and depression are associated with both single and multimorbidity. 9 The objective of this study is to document the prevalence of common multimorbidity and its associated risk factors among population of Mechinagar Municipality. The magnitude of the problem seems to be larger for multimorbidity compared to single chronic disease. Since those with multimorbidity have higher demand of healthcare services and increased health care costs, 10 a better understanding of the burden of multimorbidity and its related factors among general population of Mechinagar Municipality is the utmost need.
Methods
Study design and settings
Community based descriptive cross-sectional study was done where selected chronic conditions were assessed within the frame work of routine Kidney Hypertension Diabetes and Cardiovascular disease (KHDC) screening activities in selected areas in Eastern Nepal. KHDC is a community-based program for early detection and management of Kidney disease, Hypertension, Diabetes and Cardiovascular diseases working in eastern Nepal since 2003. 11 The study was conducted at the randomly selected three clusters in Mechinagar Municipality where KHDC screening activities was conducted. Mechinagar Municipality is the largest municipality in Jhapa District, Koshi Pradesh being one of the most ethnically diverse districts of the country .It has highest population among municipalities in the whole country.
Study population
The adult population ≥20yrs old attending KHDC screening program were the study population. Those individuals who did not consent to participate in study , aged <20yrs and individuals living for less than 6 months in the district were excluded from the study.
Variables studied
1. Socio-demographic and lifestyle factors related data were collected based on self-report that included respondents age, gender, place of birth, residence , educational level, marital status, occupation , smoking habit, alcohol intake, annual household income, intake of fruits and vegetables, physical activity, type of vehicle in the house. Other social determinants of health (SDOH) were collected as self-rated health, health insurance, perceived discrimination and head of the household. Family history of illness of chronic diseases kidney disease, hypertension, diabetes and cardiovascular disease were collected. Chronic disease like ischemic heart disease, chronic obstructive pulmonary disease/emphysema, stroke, diabetes, chronic kidney disease, hypertension, arthritis was documented.
Operational definitions
1. Multimorbidity was defined as the simultaneous occurrence of two or more chronic health conditions in the same person , without defining a primary disease.1,3,2
2. Social Determinant of Health included social practices and conditions (such as lifestyles, living and work situations, neighborhood characteristics, poverty, environmental pollution, etc.); Socio-economic Status (income, education , and occupation); stressful circumstances; and racial discrimination, along with economic (e.g., unemployment , business recessions), political (e.g., government policies, programs, and public insurance benefits), and religious (e.g., piety, proscriptions against smoking and drinking) factors that affect the health of individuals, groups, and communities—either positively or negatively. 12
3. Marital status • Single: unmarried ,divorced , separated , widow, widower • Married
4. Type of house: kachha, pucca , semi-pucca , cemented , tin , wooden 13
5. Literate: Those who have received formal education and has got the ability to read and write. Illiterate refers to those who cannot read or write and haven’t received any sort of formal education. 14
6. Skilled and semi-skilled agriculture: Those who have received formal education and involved in forestry and fishery are referred as skilled agriculture. Those who does not have any formal education and possesses no particular trained skills on agriculture are referred as semi-skilled agriculture. 14
7. Legislature: Those involved in lawmaking branch of government. 14
8. Poverty index: Poverty line was calculated according to World Bank standard i.e less than USD 1.90 per day head as below poverty line and more than USD 1.90 per day per head as above poverty line. 15
9. Behavioral risk factors: Behavioral risk factor is any attribute, characteristic or exposure of an individual that increases the likelihood of developing a disease or injury. Some examples of the more important risk factors are physical inactivity, tobacco and alcohol consumption.
10. Smoking status: i) Current smokers are those who said they had smoked daily or in the past 30 days.
16
ii) Former smokers: Those who have smoked in the past 12 months but have quit smoking at the time of study
16
iii) Never: life time abstainer • Cigarette, cigar, hookah, bidi, e-cigarette was considered for the study.
17
iv) Smokeless tobacco: • It is the form of tobacco that is not burned. The chewing tobacco (also called as oral tobacco, spit tobacco, etc.), available as khaini, surti, gutkha, etc., are considered as smokeless tobacco in our study.
11. Type of Alcohol: Divided into 3 types ;Home-brewed (home-made) alcohol, commercially available alcoholic beverages such as beer, whiskey, wine(branded) or consumption of both types.
12. Hypertension: Hypertension is defined as having systolic blood pressure ≥140 mm Hg and/or diastolic blood pressure ≥90 mm Hg during the study based on the average of two or more properly measured blood pressure readings from two or more clinical visits , or being previously diagnosed as having hypertension determined for high blood pressure (Joint national committee on prevention ,detection, evaluation and treatment of high blood pressure, JNC 8 criteria) 18
13. Disease such as arthritis , chronic obstructive pulmonary disease , heart attack/stroke and chronic kidney disease. were determined by reviewing documentation such as a treatment record book or by the history of the participant taking medicine for the same.
14. Diabetes Mellitus: Fasting plasma glucose ≥126mg/dl or Previously Physician diagnosed diabetes receiving treatment .Fasting is defined as no calorie intake for at least of 8 hour. 19
15. Body mass Index (BMI) is the ratio of weight in kilograms to the square of height in meters (kg/m2). It is expressed categorically as It is expressed categorically as underweight (<18.5kg/m2), , normal (18.5- 22.9 kg/m2), overweight (23- 24.9kg/m2), obese (>25 kg/m2) according to BMI cut-offs for Asian population. 20
16. Common morbidity is taken as cardiovascular disease (ischemic heart disease, stroke and hypertension), chronic obstructive pulmonary disease, diabetes, arthritis, chronic kidney disease and others which are the top most non-communicable disease of Nepal according to population survey done by Nepal Health Research Council (NHRC), 2019. 17
Technical information
Pre-designed semi-structured multimorbidity assessment questionnaire for primary care (MAQ-PC) 21 was used to assess the prevalence of multimorbidity among the population. Both English and Nepali version of the questionnaire was used for the study as preferred by the participants during pre-testing. Pretesting was performed among 10% of the sample population, (i.e., 60)in Dharan sub-municipality.
Anthropometric measurement includes height measured in participants without shoes by using stadiometer placed against the wall weight using standard procedure and weight measured with a regularly calibrated digital scale. Blood pressure was measured with a calibrated aneroid sphygmomanometer with appropriately sized cuffs under standard techniques. Three readings of systolic and diastolic blood pressure were measured and mean of second and third reading was calculated. Plasma glucose concentration was determined by the glucose oxidase peroxidase method (Vitalab Selectra-2, Merck, Germany. 4
Sampling and sample size
Sample sizes was estimated based on the prevalence of multimorbidity recorded in low middle income countries, Nepal (15.2%).
10
The sample size was calculated using the following formulae for population survey:

N = Sample size, Z = Z-Score point at significant level of 5%= 1.96
p= Prevalence of multimorbidity in general population i.e. 15.2%
q = 100-P
d = relative precision error = 0.2 (20%) so,
N= (1.96)2 x 15.2 x 84.8 /9.2416
N = 536
Adding 10.0% non-response based on other study experiences, the final required sample size was 590. Altogether, 590 eligible participants were enrolled in all screening pre-defined pocket areas. This study was conducted in 3 different screening pre-defined pocket areas of KHDC which had population of 5,103 in Mechinagar-14 (Duwagadi), 6,748 in Bhadrapur-9 (chandragadi) and 5,050 in Mechinagar-4 (Bahundangi) According to sample size estimation at least 600 individuals were interviewed and examined. Hence, a total of 197 subjects from each pre-defined pocket areas/screening were enrolled considering systematic random sampling methods. Kth interval for each pocket areas were calculated by dividing total estimated population size by our sample size which was calculated as 26th,34th and 25th participants in 3 camps i.e. Mechinagar-14 (Duwagadi), Bhadrapur-9 (chandragadi) and Mechinagar-4 (Bahundangi) respectively.
Screening camp comes under regular activity of KHDC done for the prevention of Non—communicable disease where participants are screened for hypertension,diabetes,hyperlipedemia,chronic obstructive pulmonary disease.
Statistical analysis
The collected data was coded accordingly and entered at Microsoft Excel 2019 and uploaded into SPSS version 11.5 for statistical analysis. 1. Descriptive statistics: The socio-demographic data was presented in frequency, percentage and age in mean, standard deviation. 2. Inferential statistics : - Bivariate logistic regression was applied to calculate the crude odd ratios for the independent factors, which was followed by multivariate binary logistic regression for adjusted odds ratio. Statistical significance has been tested with 95% confidence interval and p value less than 0.05 has been considered as significant.
Ethical concerns
Ethical clearance was obtained from the Institutional Review Committee (IRC) of B.P Koirala Institute of Health Sciences (Ref No 248/077/078, Code No IRC/1884/020).Written informed consent was obtained before commencing the data collection and all information was kept confidential.
Results
Socio-demographic Characteristics of the Participants.

Distribution of participants according to behavioral risk factors.

Hypertension was also seen in 39.2% of the participants.
Distribution of participants according the common chronic disease morbidities.

Distribution of participants according the family history of common chronic morbidities.

The prevalence of other morbidities was found to be highest with acid peptic disease (44.1%), arthritis (35.4%), followed by chronic back ache (31.2%), thyroid disease(2.7%), depression(1.5%), deafness (1.9%) and less than 1 % in epilepsy, cancer, filariasis, stroke.
Regarding the presence of multimorbidity among the participants, 22.4% of them had multimorbidity.
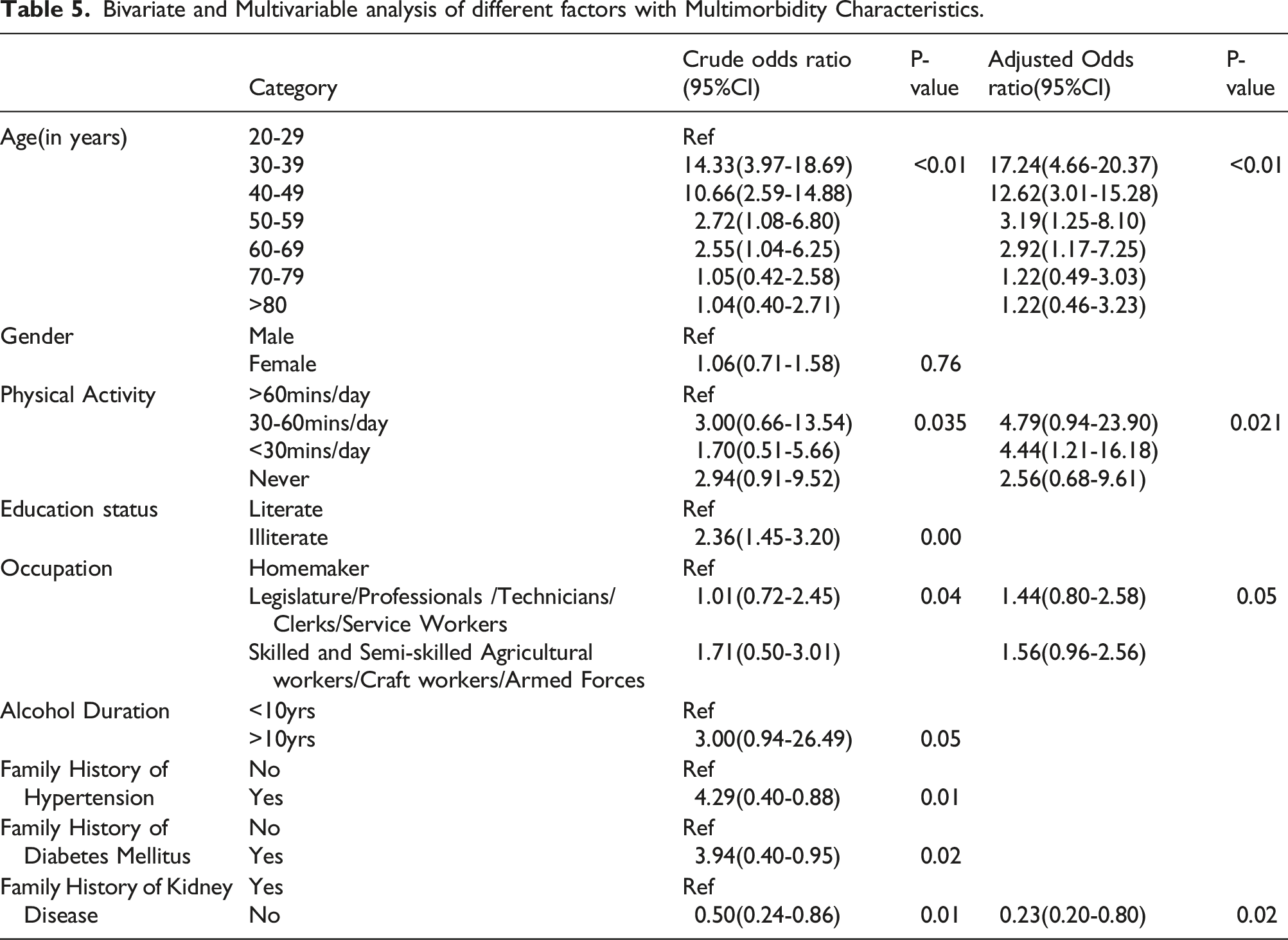
Bivariate analysis of the independent factors was done to calculate the crude odds ratio for the same. Bivariate analysis of multimorbidity with different variables like age, gender, education status, occupation, alcohol duration, physical activity, family history of chronic diseases was taken into consideration.
Bivariate and Multivariable analysis of different factors with Multimorbidity Characteristics.
Discussions
Multimorbidity of noncommunicable diseases is becoming more prevalent globally, and this has rising implications for the treatment of individual patients, estimation of disease burden in communities, and efficacy and efficiency of the health system 5 . However, very little research has been undertaken in low middle income countries regarding multimorbidity, where 80.0% of the burden of non-communicable diseases (NCD) falls 22 (16). This is a cross-sectional study which was conducted to document the prevalence of common multimorbidity and its associated factors among population of Mechinagar Municipality.
Socio-demographic characteristics and Behavioral risk factors
In this study majority of the participants were from age group 50-59yrs. The mean age of participants in our study was 51.55 ± 15.89 years . The mean age of 69.9yrs was found in a study done by Uday et al in rural area of Sunsari and Morang district 22 which is higher than our the study. The age of participants is higher than our study as they have taken only older adults while our study has incorporated all adult population>20yrs.The majority (61%) of female participants in our study is also comparable to the sex ratio of the country according to latest census 2011 which is 94.2 male per hundred female. 23
This study showed that only 10.3 % were current smoker and 4.6% were former smoker . These data were almost similar to the figures from a study done in eastern Nepal by Sharma et all where 11.9% were current smoker and 8.8% were former smoker. 24 Our study also showed that , only 2.0% of the participants were involved in >60mins/day physical activity, 4.3 % involved in 30-60mins physical activity per day. These findings are inconsistent with the findings of the study done by Sharma et all where 37.1% of the study participants were performing >60 min/day physical activity and 25.3% were performing 30–60 min/day physical activity. 24 However , these findings are almost similar to the findings of study done in eastern Nepal where 77.1% of the participants were found to be physically inactive. 22 The findings of our study could be because almost half of the participants were illiterate i.e. 45.1% who are unaware about the benefits of physical activity and there seems to be gap between knowledge into practice in those who have knowledge regarding the benefits of physical activity due to various reason like lack of motivation, busy working hours in office and so on. Health burden of sedentary lifestyle is huge. Thus, the need of adequate intervention and health promotion is paramount. Regarding the fruit intake behavior, 30.4% of the participants consumed only once a week whereas, 23.7% of participants consumed fruits every day and majority of them consumed 3-5times/day which is consistent with the findings done in Eastern Nepal. 24
Around 38.7% of the participants were in obesity category and 19.0% them were pre-obese. These data were higher than WHO STEPwise approach to non-communicable disease risk factor surveillance (STEPS) survey, where 17.7% of the participants were pre-obese and only 4.0% of them were obese. 16 This can be reasoned with the fact that prevalence of sedentary lifestyle in our study population is high and also the second largest group of participants in the study are homemaker which could have attributed to increased weight.
Prevalence of chronic morbidities
Hypertension
In our study, 39.2% of the participants were hypertensive. This findings were similar to a study done in Bangladesh where the prevalence of hypertension was found to be 38.7%. 2 Almost similar prevalence of hypertension was found in a nationally representative study done in Nepal which had a prevalence of 26% 25 and also another study done in eastern Nepal which had prevalence of 33.9%. 24 The higher percentage of hypertensive in our study could be because of the fact that it was done under a screening camp of KHDC and mostly those who are already known to have certain health condition are likely to visit as a part of their regular medical check. Contrary to our finding, study done by Chataut et al in Ramechaap showed 20.5% as hypertensive. 26
Diabetes
Our study showed the prevalence of diabetes to be 7.8% which is similar to findings of nationwide STEPS survey which showed the prevalence of diabetes to be 5.8%. 16 Our findings were similar to the findings of the study in eastern Nepal by Sharma et al which had prevalence of 6.3%. 24 likewise, systematic review and meta-analysis by Shrestha et al also had consistent findings to our study with prevalence of 8.5%. 27
Chronic Obstructive Pulmonary Disease (COPD)
There were differences in the prevalence of chronic obstructive pulmonary disease in our study and other studies because our study findings were based on only self-reported condition with documentation and there might be still more participants in our study yet to be diagnosed with chronic obstructive pulmonary disease.28,29
Arthritis
Our study showed 35.4 % of the participants reported of having arthritis .This finding is almost similar with the result of the study done in Eastern Nepal which showed the prevalence of 41.7%. 22 However, the study done in Canada showed lower prevalence of arthritisi.e.17.6%. 30 This could be because of the variation in study setting as the participant of the developing countries have hardship life due to geographical difficulties and also large group of participants in our study are obese which is one of the aggravating factor for arthritis.
Chronic kidney disease
Among the participants, 2.4% of them reported of having chronic kidney disease which is less than the nationwide study done in Nepal which had prevalence of 6.0%. 29 In another study done in six different regions of the world, prevalence of Chronic kidney disease (CKD) was found 14.3%. 31 The difference in the study findings could be because of the different study settings, population and methodology used in these different studies.
Heart attack and stroke
Our study reported of very few i.e.,2.5% participants who had prior heart attack and stroke. The findings were similar to the findings of the study done in eastern Nepal which had prevalence of 2.4% 22 and a, a nationwide study done in Nepal with prevalence of 2.9% 29
Multimorbidity
Our study showed multimorbidity present in 22.4% of the participants. Contrary to our findings, the prevalence of multimorbidity in South-Africa was found 4.0%. 9 Our study findings is higher than the study findings done in Eastern Nepal which had prevalence of 14.0%. 22 This could be reasoned with the fact that our study incorporated 7 different common Non-communicable Disease while the study in eastern Nepal took only 4 diseases into consideration. However, almost similar prevalence of multimorbidity to our study was found in an study conducted in Odisha, 28.3%. 32 The study conducted in Bangladesh had higher prevalence of multimorbidity than our study, 53.8%. 2 This could be because the study in Bangladesh had elderly population as their study population and the prevalence of multiple chronic conditions is expected to increase with increasing age unlike our study which had mixed study population ranging from 20-92yrs of age. 2
Association of Multimorbidity with socio-demographic characteristics
In many low- and middle-income nations, little is known about the correlates of multimorbidity because research, medicine, and health care have usually focused on single diseases .The strong association between age and multimorbidity is well recognized. Our study showed those between age group of 40-49yrs were 12.62 times more likely to have multimorbidity than those who were between age group of 20-29 years (p=<0.01,CI 3.01-15.28).Likewise, those who were ≥80yrs of age were 2 times likely to have multimorbidity than those who were between age group of 20-29years (p=<0.01, CI 0.46-3.23).Similar Findings were seen in a study done in Canada which showed those >65yrs were 35.4(26.2–46.8) times likely to have multimorbidity than those between age 20-34yrs of age. 30 Likewise in the same study, those between age group 50-64yrs were 13.6 (10.1–18.4) times likely to have multimorbidity than those who were between age group 20-34 years. 30 The study done in India also showed similar findings where multimorbidity of participants increased with the increasing age. The participants aged 70 and above were 39.15 (20.72, 73.98) times likely to have multimorbidity than those aged between 18-29 years. 33
Worldwide study have estimated that physical inactivity is responsible for 6.0% of the burden of disease from chronic diseases with 3.2% in South-east Asia. 34 Our study showed that those participants who were involved in physical activity for 30-60mins/day were 4.79 times more likely to have multimorbidity than those who performed ≥60mins/day physical activity. Likewise , those participants who performed <30mins /day physical activity were 4.44 times more likely to have multimorbidity than those participants who performed >60mins/day physical activity. The odds of having multimorbidity in participants who never performed any physical activity was 2.56 times to those who performed physical activity for >60mins/day. Similar findings were observed in a study done in eastern Nepal where physically inactive individuals had five times higher odds of having multimorbidity than those of regular physical activity(AOR: 5.02; 95% CI: 1.47-17.17). 22 This finding of our study demands the need of both early primary prevention at the community level to prevent multimorbidity as well as secondary/tertiary prevention at the health care facility to avert the further health consequences in those who already have multimorbidity.
Working status of the individuals also affects the health status of the people. This study showed higher odds of multimorbidity in individuals who were working than those who were not. However, a study done in Vietnam among older adults showed higher prevalence among those who were not working than those working. However, the association was not found significant among occupation status and multimorbidity.
Our study showed that multimorbidity was more common in those individuals who had family history of kidney disease. Those individuals who did not have family history of chronic kidney disease were 87% less likely to have multimorbidity than those who had family history of chronic kidney disease. Similar findings were observed in a study done in China where those who have family history of chronic diseases were 2.037 times more likely to have multimorbidity than those who did not have family history of chronic Disease. 35 Similarly, a study done in various parts of India also had similar findings where those individuals with family history had 1.79 [1.58, 2.03] times higher odds of multimorbidity than those who did not have any positive family history. 36
Limitations
As a cross sectional study, which was questionnaire based and with some objective measurements, following limitations were observed. We could not include mental conditions such as depression. The individuals' self-reported behavioral traits were used to compile the data. There could be a social desirability bias in smoking and alcohol consumption records. 37 Furthermore, the recall bias regarding intake of fruit, vegetable intake and accuracy of information gathered for physical activity based on the participant's self-report cannot be ignored. The causal relationships between independent variables and the prevalence of multimorbidity cannot be determined, rather evidence on prevalence and factors associated with the likelihood of multimorbidity were determined.
Conclusion
The study revealed high prevalence of multimorbidity among population of Mechinagar municipality, (22.4%) In multivariate analysis individuals with increasing age, occupation, physical activity and positive family history of kidney disease was found to be significantly associated with multimorbidity. The study revealed that participants with increasing age were more vulnerable of having multimorbidity. Significant association was also found between physical activity and multimorbidity.
Our study highlighted the strong association between multimorbidity and physical inactivity, which suggests both the opportunity for early prevention and the need for tailoring the physical activity to the level of disability (especially for osteoarthritis). Physical activity should be incorporated within school and community health programs and at all levels of care. The findings of our study indicate the need of intervention strategies and community-based health promotion programs in reducing the burden of multimorbidity among the adult population. Furthermore , individuals with advancing age also underscore the need for the attention of policymakers and the implementors to invest more in the development of multidisciplinary management packages for chronic multimorbid conditions. Moreover, we also suggest the need for qualitative research to understand the problems at the individual and population levels, community/family level, and organizational level, which might be help to develop a comprehensive intervention package for people with chronic multimorbid conditions. New healthcare models should be developed and evaluated to better meet the healthcare needs of elderly people with multimorbidity .There is need to put in place measures that will encourage healthy lifestyle and living in the general population by creating awareness about the benefit of physical activity and healthy diet. Since multimorbidity may cause significant cognitive and functional consequences, one of the relevant implications relating to our findings is that researchers and policy-makers should work together to develop effective intervention strategies and programs to reduce the burden of multimorbidity.
Supplemental Material
sj-pdf-1-cob-10.1177_26335565241237892 – Supplemental Material for Prevalence of multimorbidity and its associated risk factors among population of Mechinagar municipality of Nepal
Supplemental Material, sj-pdf-1-cob-10.1177_26335565241237892 for Prevalence of multimorbidity and its associated risk factors among population of Mechinagar municipality of Nepal by Suman lohani, Sanjib Kumar Sharma, Suman Bahadur Singh, Surendra Uranw, and Anup Ghimire in Journal of Multimorbidity and Comorbidity
Footnotes
Acknowledgments
We would like to acknowledge all the residents of Jhapa district for their kind cooperation during data collection and all members of Kidney Hypertension Diabetes Cardiovascular disease (KHDC Nepal) for being so supportive.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the screening program (during data collection).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.