
Abstract
Introduction
Persistent pain (PP) and long-term conditions are all associated with psychological well-being. Less is known about their associations with reduced psychological well-being when co-occurring. We investigated how PP and long-term physical and mental conditions relate to psychological well-being when occurring together.
Method
Data collected in the Danish population-based Lolland-Falster Health study were used in this cross-sectional study. Participants aged ≥18 years completing questions concerning PP, long-term conditions and psychological well-being were included. PP and long-term conditions were defined as conditions lasting 6 months or longer. Psychological well-being was assessed by the World Health Organization Well-Being Index (WHO-5). Multiple linear regression investigated combinations of PP and physical and mental long-term conditions and their associations with WHO-5.
Results
Of 11,711 participants, 10,744 had available data. One third had PP (n = 3250), while 6144 (57%), 213 (2%) and 946 (9%) reported having only physical conditions, only mental conditions or both, respectively. All combinations of PP and long-term conditions were negatively associated with WHO-5. PP in combination with mental (−23.1 (95% CI −28.3 to −17.8)) or both physical and mental conditions (−25.1 (−26.7 to −23.52) yielded the strongest negative associations. Two or more pain sites together with long-term physical and mental conditions was associated with a lower WHO-5 score (−6.2 (−8.9 to −3.5) compared to none or one pain site.
Conclusion
The presence of PP and long-term conditions, in particular mental conditions, were strongly associated with worse psychological well-being. This highlights the importance of assessing psychological well-being in individuals with PP and long-term conditions.
Keywords
Introduction
Pain is a major cause of years lived with disability, 1 social disturbance 2 and impaired quality of life (QOL),2–4 and is typically the most frequent cause of care-seeking.1,5 Pain is defined as an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage. 6 Persistent pain (PP) is defined by The International Association for the Study of Pain (IASP) as pain lasting for more than 3 months. 1
Today, it is recognized that PP entails a pathologic reorganization of the neural system caused by many factors.7,8 PP and having pain in multiple sites of the body are associated with mortality and health-related risk factors9,10 and can lead to biological and social life disturbances as well as a negative impact on mental health. 11 For example, affected mood and increased level of anxiety are reported to reduce psychological well-being in individuals with PP. 12 PP is common in people living with a wide range of long-term conditions. 13 Similar to PP, living with physical and mental long-term conditions can have an impact on mental health.14–16 However, it is unclear how PP and physical and mental conditions influence psychological well-being when occurring together. Until recently, the International Classification of Diseases (ICD) did not include PP, and the recognition of PP as a disease has therefore been continuously debated. 1 As a result, PP has often not been included in analyses exploring the impact of living with several long-term conditions. 17 Nonetheless, PP represents a long-term condition that requires special treatment and care 1 and knowledge about the potential relationship between PP, long-term physical and mental conditions, and psychological well-being is essential as reduced psychological well-being is linked with a higher level of morbidity, several health problems, and increased mortality rate in both healthy and diseased individuals.12,18,19
Previous studies that investigated a relationship between PP and long-term conditions used only a few, specific combinations of long-term conditions. For example, combinations between PP and either diabetes, hypertension, or bone disease have been reported to impact negatively on health-related quality of life. 20 In a previous population-based study including the same population as in our current study, combinations of physical and mental long-term conditions were associated with poorer psychological well-being. 15 Mental conditions seemed to be particularly important for this association, whereas only small variations were found across the physical conditions. 15 Yet with PP potentially leading to biological and social life disturbances and poorer mental health, co-occurrence of PP and physical long-term conditions may potentially have a clinically relevant impact on mental health. 11 Today, there are no consensus on how to cluster long-term conditions. 21 As very little variance in psychological well-being was found within various physical conditions in the previous population-based study, it seemed valid simply to group long-term conditions in physical and mental conditions. 15 In contrast to the use of specific combinations of long-term conditions, such grouping allows for a simpler interpretation of the relationship between PP and long-term physical and mental conditions and its association with psychological well-being. This may help clinicians assess and support individuals burdened from chronic conditions, PP and reduced psychological well-being.
The aim of this study was to investigate how PP and long-term physical and mental conditions relate to psychological well-being when occurring together. Our hypothesis was that PP and physical and mental conditions together have a stronger association with poor psychological well-being than PP or long-term condition alone. Further, we investigated if multiple pain sites were associated with psychological well-being in individuals living with and without long-term physical and mental conditions.
Methods
This cross-sectional study complies with STROBE reporting guidelines. 22
We included participants in the household-based population study Lolland-Falster Health Study (LOFUS) 23 recruited from a mixed rural-provincial part of Denmark with lower life expectancy, lower socioeconomic status, and higher burden of mental and physical health problems than the Danish average. 23 Lolland-Falster health study is approved by Region Zealand’s Ethical Committee on Health Research (SJ-421) and is registered by the Danish Data Protection Agency (REG-24-2015) and Clinicaltrials.gov (NCT02482896). Detailed descriptions of the LOFUS study design and methodology are published elsewhere.23,24
Sample
Eligible participants for the present study were aged ≥18 years and participated in the LOFUS study between 8 February 2016 and 7 March 2019. Most participants answered questionnaires electronically, but paper-based versions were available.23,24 Only participants completing questions about persistent pain, long-term conditions and psychological well-being were included.
Primary outcome
The World Health Organization Well-Being Index (WHO-5) is a generic, self-reported questionnaire assessing psychological well-being. 25 WHO-5 consists of five positively phrased statements concerning the previous 14 days. It is scored using a 6-point Likert scale (0 = at no time; 5 = all of the time). 25 The items are (1) ‘I have felt cheerful and in good spirits’, (2) ‘I have felt calm and relaxed’, (3) ‘I have felt active and vigorous’, (4) ‘I woke up feeling fresh and rested’ and (5) ‘My daily life has been filled with things that interest me’. The sum of the item-scores (0–25) are multiplied by 4, giving a sum score 0 to 100, with 0 representing the worst possible psychological well-being and 100 the best. 25
WHO-5 is validated and has successfully been used to assess psychological well-being across a wide range of patient groups. 25 A difference of 10 points is considered clinically relevant.25,26
Data variables
Persistent pain
We used a single yes/no question ‘Do you have long-lasting/chronic pain that has lasted for 6 months or more?’ to define PP. The question has been used nationally in The Danish Health and Morbidity Surveys in 2013 and 2017. 27 The question was followed by ‘If “yes”, where do you feel pain?’ with 11 possible options to be selected (more than one could be selected): (1) head, neck, face and mouth, (2) shoulders, arms and hands, (3) chest, (4) stomach, (5) back, (6) buttocks, (7) legs and feet, (8) pelvis, (9) rectum, (10) genitals and urinary tract and (11) other. For the purpose of this paper, we grouped the 11 sites into a total of six overall pain sites based on their location; (1) head, neck, face and mouth, (2) upper extremity, (3) truncus (including the three sites: chest, stomach and back), (4) pelvis, reproductive organs and rectum (including the four sites: pelvis, buttocks, rectum, and genitals and urinary tract), (5) lower extremity and (6) other.
Classification of long-term physical and mental conditions
The classification of long-term conditions in the current data set has previously been described in detail. 15 In summary, long-term conditions were self-reported from a list of 18 conditions previously used in the Danish General Suburban Population Study 28 and a national health cohort in Denmark conducted since 1987. 29 The 18 conditions included were: (1) acute myocardial infarction, (2) atherosclerosis in the heart, (3) angina pectoris, (4) blood clot (thrombosis) in the leg, (5) diabetes, (6) asthma, (7) allergy (not asthma), (8) kidney disease, (9) cancer, (10) anxiety, (11) depression, (12) osteoarthritis, (13) rheumatoid arthritis, (14) hypertension, (15) long-term bronchitis, emphysema, long-term obstructive pulmonary disease (COPD), (16) migraine or frequent headaches, (17) spinal hernia or other spinal diseases, (18) Others. The condition ‘hypertension’ was excluded as it was seen as a risk factor for many of the included conditions. 30 Further, a systematic coding of the ‘others’ category was conducted (for details, see Tang et al. 15 ). In total, 74 medical conditions were classified for this study. These were divided into two overall condition groups, physical and mental. This was done to simplify interpretation of our findings and enhance statistical power. This approach is supported by existing research in the same population, showing little differences in associations with WHO-5 across physical conditions, whereas mental conditions have a threefold greater association with WHO-5 compared to any physical conditions. 15
Covariates
We coded the sociodemographic covariates collected in LOFUS 24 as follows: age (years), gender (female, male), marital status (married, separated/divorced, widowed, single), working status (unemployed, out of the labour market, in labour, studying or training, caretaker or work in home, other) and education level (less than high school, high school, Bachelor degree, advanced degree, other). An ‘other’ category was available for working status and education level without further specification. In total, 285 (2.7%) responded ‘other’ for working status and 563 (5.3%) for education level.
Statistical analyses
All statistical analyses were performed using the software SAS Enterprise Guide 5.1 (SAS Institute Inc., Cary, NC, USA). Baseline characteristics were calculated using descriptive statistics for normally distributed data (mean, ±SD) and categorical data (frequencies and percentages), unless other is mentioned.
Multiple linear regressions were used to investigate the associations between the WHO-5 and (1) PP, (2) long-term physical and mental conditions, and (3) the combination of PP and long-term physical and mental conditions. PP was inserted as a binary variable (yes/no). Based on previous research, long-term conditions were coded as none, physical, mental or a combination when assessing its association with WHO-5. 15 Finally, all combinations of PP and physical and mental conditions (8 combinations in total) were used to assess associations between PP and long-term physical and mental conditions and WHO-5. Two regression models were built. The first model adjusted for age (continuous) and gender. The second and fully adjusted model further included marital status, working status and education level. Co-variables were inserted as described above. Models were run on the full sample.
Location and number of pain sites were modelled separately in a sub-analysis to explore their association with the WHO-5 score in participants reporting PP. Location of PP was one of the six pain sites. Number of pain sites were coded as a continuous variable when exploring its association with the WHO-5 score, and as, none, 1 or 2 and above when physical and mental conditions were taken into account. This was due to the relatively low number of individuals with especially mental conditions that reported pain. For all models, the coefficient of determination (R2) was extracted and beta coefficients (95% CI) were reported. Assumptions for all models were investigated through diagnostic plots. Model assumptions were not violated in any of the analyses. To investigate risk of bias, we assessed differences in baseline characteristics between responders and non-responders. Level of statistical significance was set at p < 0.05.
Results
Out of a total of 11,711 participants, 10,744 (92%) provided information on PP, long-term physical and mental condition, and psychological well-being (Figure 1). As the majority of the 1027 non-responders did not provide any questionnaire data, a comparison between responders and non-responders was only possible on age, gender, height and weight. There was no evidence of a difference in gender (p = 0.19), height (p = 0.29) or weight (p = 0.46), but non-responders were slightly older than responders (2.2 years; p < 0.001) (data not shown). Study flow and distribution of long-term conditions in participants with and without persistent pain.
Baseline characteristics of the 10,744 included participants.
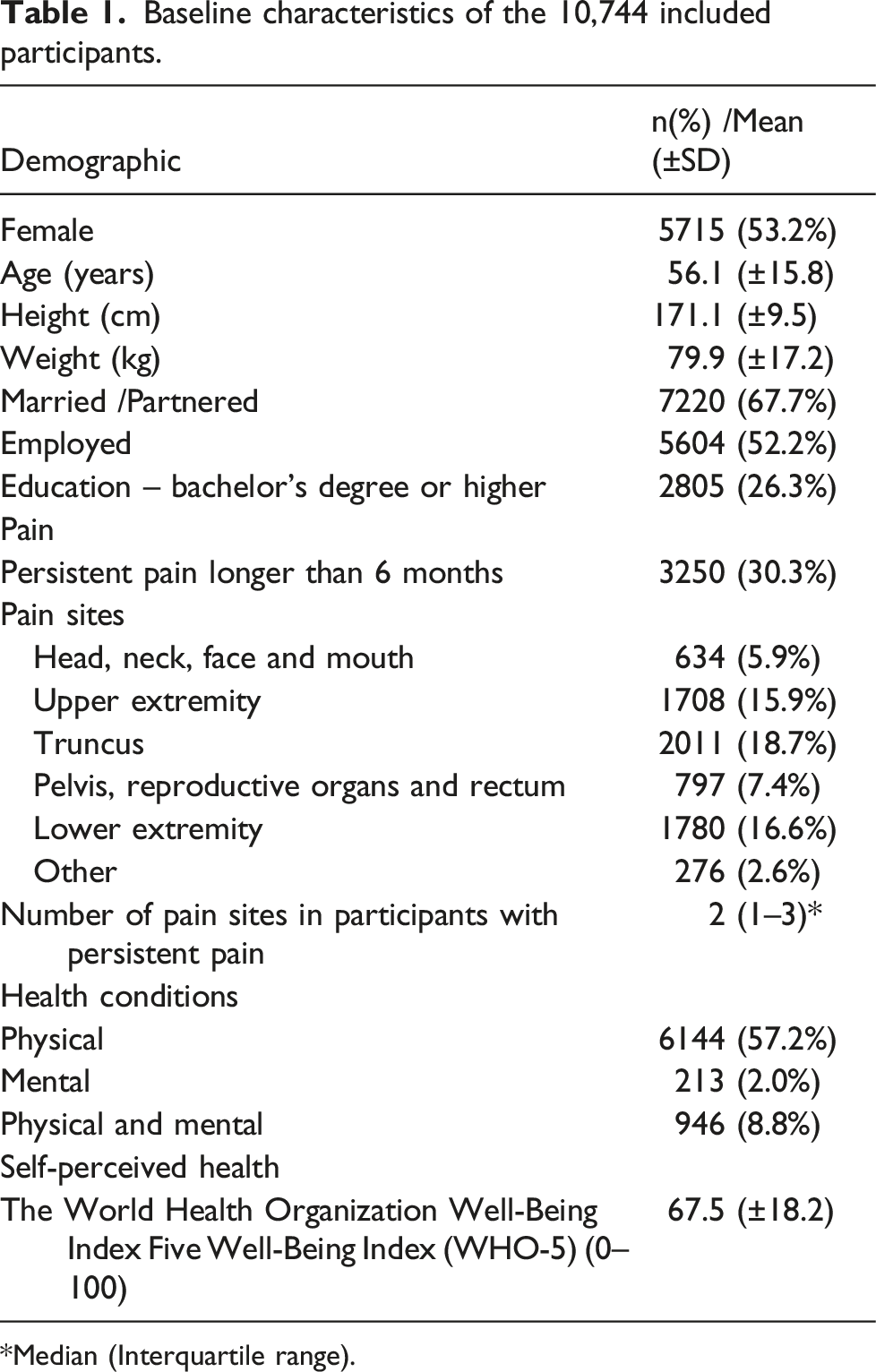
*Median (Interquartile range).
Multiple linear regressions showing the associations between The World Health Organization Well-Being Index (WHO-5) and combinations of long-term conditions and persistent pain.

Age/gender adjusted model: Adjusted for age (continuous) and gender.
Fully adjusted model: Adjusted for age (continuous), gender, education level, marital status and working status.
R2: Coefficient of determination, Physical: Physical long-term condition, Mental: Mental long-term condition, Pain: Persistent Pain.
Exploring associations across pain sites, only the truncus area was found to be slightly negatively associated with WHO-5 score compared to the rest of the study sample not reporting pain in the site of interest (fully adjusted model: −2.0 (95% CI −3.3 to −0.6)) (See Table A1). However, a higher number of pain sites were associated with worse WHO-5 score (p < 0.001) (Figure 2 and Table A2). Compared to no pain sites, having two or more pain sites together with a long-term physical or mental condition or both yielded a stronger association with a poorer WHO-5 score than having only one pain site. The association was, however, not significant in participants only having PP and a mental condition (−10.6 (95% CI −21.3 to 0.1; p = 0.11)) (Table 3). Associations between The World Health Organisation Well-Being Index (WHO-5) and self-reported numbers of persistent pain sites for all participants irrespective of types of long-term conditions. Data is adjusted for age, gender, marital status, working status and education level and presented as mean and 95% confidence interval. Multiple linear regressions showing the association between The World Health Organization Well-Being Index (WHO-5) and combinations of long-term conditions and number of persistent pain sites. Age/gender adjusted model: Adjusted for age (continuous) and gender. Fully adjusted model: Adjusted for age (continuous), gender, education level, marital status and working status. Physical: Physical long-term condition, Mental: Mental long-term condition, Pain: Persistent Pain.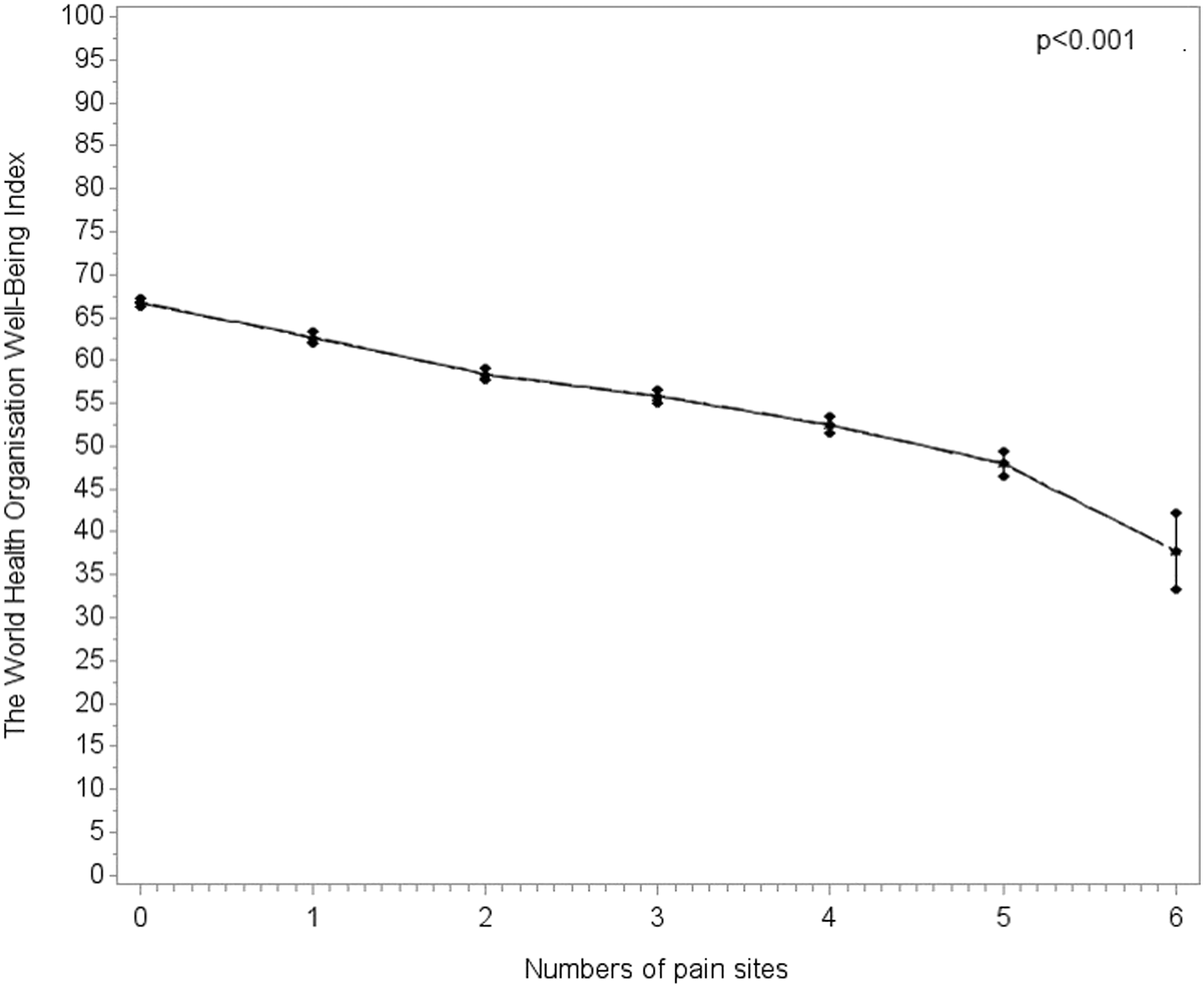

Discussion
Based on data from a large Danish population-based cohort, we showed that having either self-reported PP for more than 6 months or long-term physical or mental conditions was associated with worse psychological well-being. However, when PP and long-term physical or mental conditions occurred all together or in binary combinations, psychological well-being was worse to a degree which is most likely clinically relevant, particularly if multiple pain sites or a mental condition is included.
Pain is typically a part of a disease trajectory,31,32 and therefore individual associations between pain and health outcomes, for example, psychological well-being, are often concealed behind the condition.31,32 Literature refers to this phenomenon as the hidden burden of PP.31,32 We demonstrated that having either PP or a long-term physical or mental condition was associated with worse psychological well-being. Yet the associations exceeded the threshold for a clinically relevant difference when they occurred together and were especially large when a mental condition was included. It was expected that the WHO-5, a measure of psychological well-being, would be worse in individuals with mental conditions than individuals with physical conditions due to the substantial impact mental conditions have on psychological well-being.15,33–36 Furthermore, it is well-known that PP can have a substantial impact on depression and anxiety symptoms 37 – and vice versa. 11 Physical conditions alone did not yield an association above the threshold for a clinically relevant difference in psychological well-being. However, evidence shows that PP is associated with poorer mental health. 11 So, although it is expected that psychological well-being is worse in individuals with mental conditions, combinations of PP and physical long-term conditions could potentially be associated with poorer well-being. Although not reaching the 10-point threshold for clinical relevance in the age and gender adjusted analysis, our study did demonstrate that a combination of PP and physical conditions was associated with poorer well-being than either alone (−9.7 (95% CI −10.6 to −8.9)). Little variance in the association with psychological well-being scores has been identified across specific physical conditions (WHO-5 range: 2.5–7.2)15. Hence, we cannot exclude that the association for some physical conditions would exceed the clinically relevant difference of 10 points. 38 In addition, a dose-response association between number of physical conditions and mental health has previously been documented but was not included in our study. 39
For the first time, we demonstrated that the co-occurrence of multiple pain sites was associated with a worse WHO-5 score. Interestingly, there seems to be a linear association between more pain sites and worse WHO-5 score. Statistical significance was found in the age and gender adjusted analysis when comparing associations between number of pain sites and psychological well-being for the group of participants having a mental condition. In the fully adjusted analysis, the estimate did exceed the threshold for a clinically relevant difference without being statistically significant (−10.6 (95% CI −21.3 to 0.1)). We interpret this to be a consequence of a low number of participants having PP combined with a mental condition (n = 36). Existing literature shows that number of pain sites is associated with increased risk of all-cause mortality 10 and physical and psychosocial risk factors. 9 This highlights the importance of assessing number of pain sites when studying the influence of PP in physical and mental long-term conditions. The fact that we saw only very small differences in psychological well-being across the individual pain sites, and far below the clinical relevance, further supports the classification of pain at multiple anatomical sites simply by the number of paint sites rather than its anatomical distribution when studying PP. 9
Our cross-sectional design does not allow for conclusions on causality but supports the significant influence of PP on psychological well-being. The biopsychosocial model of pain illustrates that PP can influence quality of life through various biological, psychological and social pathways. 11 A higher disease burden can have a greater impact on all pathways and may be the simple explanation to why having PP in addition to physical and mental conditions is associated with the worst psychological well-being.
Self-perceived well-being can be assessed in four domains: physical, psychological, social and spiritual. 40 However, in the past decades, psychological well-being has been investigated in many studies and found to be strongly associated with physical health and psychological function14,15,18,38 and to have favourable influence on survival in both healthy and diseased populations. 19 Our study adds to this by highlighting that if PP and physical and mental conditions occur together or in binary combinations, they could be important contributors to worse psychological well-being. Major societal awareness in public health and research concerning the huge burden of disease and disability that is driven by pain-associated conditions has been called for.32,41 Despite the lack of causality in the cross-sectional design, our results highlight the importance of including an assessment of psychological well-being in individuals living with PP and long-term conditions, especially if occurring together, and in individuals with a mental condition.
Limitation
The findings in this study are based on data from a socioeconomically disadvantaged area of Denmark having a higher burden of mental and physical health problems compared to the Danish average. 23 In our study, 30% reported PP compared to the 16% previously being reported across Denmark. 42 Despite the fact that we adjusted for important sociodemographic factors (e.g. education level, marital status, working status) that can accompany PP, 1 our results need to be verified in a more representative population to strengthen their generalizability to the entire Danish population.
Using self-reported PP defined as a duration of 6 months is likely to increase the risk of recall bias. PP is often defined as a period longer than 3 months. 1 From our data, we were not able to verify the exact PP duration for each individual, and we could not assess whether findings were the same had we used another definition of PP.
Long-term conditions can lead to different pain types (e.g. neuropathic and musculoskeletal pain) with different pain severity across various pain sites. 1 Our data did not show any large difference in psychological well-being across pain sites (Table A1). Data on pain types, severity and diagnostic pain patterns were unfortunately not available for our analyses. One might expect that increased pain severity or certain pain patterns could have an even worse association with psychological well-being. Furthermore, future research must determine if conditions where pain is a more central symptom, for example, osteoarthritis, is similarly associated with psychological well-being as conditions where pain is less common.
Possible usage of pharmacotherapy for PP was not adjusted for in our analyses. A previous study reported that the associations between PP and mortality were mediated by opioid use. 10 Despite a short-term pain relief, long-term usage of analgesics can lead to negative mental consequences like depression. 43 So, the lack of information on analgesics could both over and underestimate the associations that we found between PP and psychological well-being.
Despite the limitations, study findings are strengthened by the large study sample collected in a socioeconomically disadvantages area with relatively high morbidity and mortality rates 44 which often is underrepresented in research. 45 Further, the study uses a valid assessment tool on psychological well-being with a clear, meaningful cut-off for clinical relevance 38 and has a limited number of participants with missing data (9%).
Conclusion
The presence of PP and long-term physical and mental conditions were associated with worse psychological well-being. Combinations, including mental conditions or two or more pain sites, had the largest negative associations with psychological well-being thereby potentially affecting the individual’s health status. Our findings highlight a need for assessing psychological well-being in individuals living with PP and long-term conditions and for clinical strategies to help and support individuals burdened from chronic conditions, PP and reduced psychological well-being.
Footnotes
Acknowledgement
The Lolland-Falster Health Study (LOFUS) is a collaboration between Region Zealand, Nykøbing Falster Hospital and Lolland and Guldborgsund Municipalities. The authors are grateful to LOFUS for making the LOFUS research data available. However, LOFUS bears no responsibility for the analysis or the interpretation conducted within this study.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: STS is associate editor of the Journal of Orthopaedic and Sports Physical Therapy, has received grants from The Lundbeck Foundation, and personal fees from Munksgaard and TrustMe-Ed, all of which are outside the submitted work. He is co-founder of Good Life with Osteoarthritis in Denmark (GLA:D®), a not-for profit initiative hosted at University of Southern Denmark aimed at implementing clinical guidelines for osteoarthritis in clinical practice.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: LHT is currently funded by a grant from the Danish Regions and The Danish Health Confederation through the Development and Research Fund for financial support (project nr. 2703) and a grant from Region Zealand (Exercise First). KHA is currently funded by a grant from Region Zealand (Exercise First). STS is currently funded by a program grant from Region Zealand (Exercise First) and two grants from the European Union’s Horizon 2020 research and innovation program, one from the European Research Council (MOBILIZE, grant agreement No 801,790) and the other under grant agreement No 945,377 (ESCAPE).
ORCID iDs

| Age and gender adjusted | Fully adjusted | |||||||
|---|---|---|---|---|---|---|---|---|
| Mean | 95% CI | p-value | R 2 | Mean | 95% CI | p-value | R 2 | |
| Pain sites | ||||||||
| Head, neck, face and mouth | −2.1 | (−3.7 to −0.4) | 0.014 | 0.131 | −1.3 | (−2.9 to 0.2) | 0.122 | 0.168 |
| Upper extremity | 1.4 | (−0.1 to 2.8) | 0.052 | 0.131 | 0.7 | (−0.5 to 2.2) | 0.219 | 0.168 |
| Truncus | −2.2 | (−3.6 to −0.8) | 0.002 | 0.132 | −2.0 | (−3.3 to −0.6) | 0.004 | 0.168 |
| Pelvis, reproductive organs, and rectum | 1.1 | (−0.5 to 2.7) | 0.162 | 0.131 | 0.6 | (−1.0 to 2.2) | 0.467 | 0.168 |
| Lower extremity | 1.2 | (−0.1 to 1.5) | 0.074 | 0.131 | 1.2 | (0.1 to 2.4) | 0.068 | 0.168 |
| Other | 0.3 | (−1.8 to 2.4) | 0.788 | 0.131 | 0.6 | (−1.5 to 2.6) | 0.578 | 0.168 |
Age/gender adjusted model: Adjusted for age (continuous), gender and number of pain sites.
Fully adjusted model: Adjusted for age (continuous), gender, education level, marital status, working status and number of pain sites.
R2 = coefficient of determination.
Associations between The World Health Organization Well-Being Index (WHO-5) and number of persistent pain sites in participants reporting persistent pain.

| Age and gender adjusted | Fully adjusted | |||||||
|---|---|---|---|---|---|---|---|---|
| Mean | 95% CI | p-value | R 2 | Mean | 95% CI | p-value | R 2 | |
| Pain sites | ||||||||
| 0 | Reference | <0.001 | 0.131 | Reference | <0.001 | 0.168 | ||
| 1 | −4.4 | (−5.4 to −3.3) | −4.0 | (−5.1 to −3.0) | ||||
| 2 | −9.8 | (−11.0 to −8.7) | −8.3 | (−5.5 to −7.2) | ||||
| 3 | −12.9 | (−14.2 to −11.5) | −10.8 | (−12.2 to −9.5) | ||||
| 4 | −17.6 | (−19.4 to −15.7) | −14.3 | (−16.1 to 12.4) | ||||
| 5 | −23.9 | (−26.6 to −21.2) | −18.7 | (−21.5 to −16.0) | ||||
| 6 | −35.8 | (−44.7 to −26.9) | −28.9 | (−37.6 to −20.2) | ||||
Age/gender adjusted model: Adjusted for age (continuous) and gender.
Fully adjusted model: Adjusted for age (continuous), gender, education level, marital status and working status.
R2 = coefficient of determination.