
Abstract
Cancer and coronary artery disease, both leading global causes of mortality, share common risk factors and are exacerbated by various cancer treatments. Coronary artery disease may delay cancer treatment initiation. Revascularization improves the safety of subsequent cancer treatment and long-term survival. Radiation commonly induces ostial coronary artery disease due to its proximity to the mediastinum, while ostial coronary artery disease related to chemotherapy is rarely reported. In this case, we explore an instance of Serous cystadenocarcinoma of the ovary, treated with Neo Adjuvant chemotherapy based on Paclitaxel, subsequently presented with ostial coronary artery disease, leading to cardiogenic shock and heart failure. The condition was successfully managed through bailed out angioplasty, followed by debulking oophorectomy surgery. The patient was under regular follow up for the past 3 years.
Introduction
Cancer and coronary artery disease (CAD) are leading global causes of death. Improved cancer therapies have increased the five-year survival rate to nearly 70% in upper middle income countries. 1 However, these treatments may lead to cardiovascular issues, resulting in acute coronary syndrome, cerebral ischemia, limb ischemia, heart failure, and arrhythmias. Individuals with mild CAD prior to a cancer diagnosis may witness disease progression attributed to the proinflammatory and hypercoagulable states induced by cancer. CAD, in turn, might lead to a postponement in the onset of cancer treatment due to either a deterioration in the patient’s cardiac health or an elevated risk associated with surgical interventions. Interventional cardiovascular procedures pose specific challenges, including an increased risk of bleeding associated with certain tumors and challenges associated with coagulation defects.
Case Report
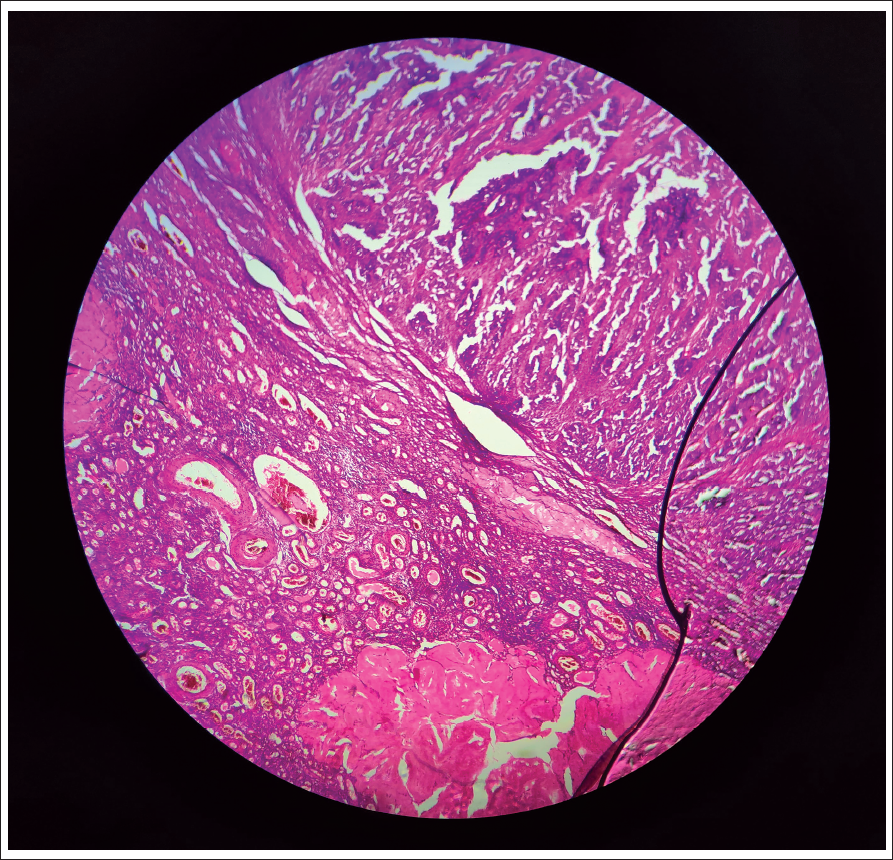
A 45-year-old female with a history of high-grade papillary serous cystadenocarcinoma of ovarian malignancy (Figure 1), who underwent six cycles of neoadjuvant chemotherapy with paclitaxel and carboplatin chemotherapy, was due for debulking ovarian surgery. She presented to us with symptoms of NYHA class III–IV of heart failure. Upon evaluation, her blood pressure was 90/60 mm Hg. Additionally, ascites and pleural effusion were noted. Platelet count was 1 lakh/mm3. An echocardiogram suggested global hypokinesia with preserved endocardium, and the ejection fraction was less than 30%. The patient was stabilized with inotropes and diuretics. Coronary angiography was performed, revealing a critical ostial left main lesion (80%–90%) and mid-left anterior descending (LAD) total occlusion with retrograde filling (Figure 2(a)). Considering the presence of cardiogenic shock and a preserved endocardial thickness of 8 mm, it was determined that the myocardium remained viable. Revascularization was deemed necessary to improve systolic function, which would facilitate subsequent surgical management of ovarian carcinoma. However, since the patient declined high-risk bypass surgery, a bailout angioplasty was planned.
Low-power Microscopic View Showing Ovarian Tissue Comprising Corpora Albicantia Along with a Tumor Component Arranged in Branching Papillary. The Tumor Cells Are Columnar with Marked Pleomorphism Scant Eosinophilic Cytoplasm and Prominent Nucleoli.
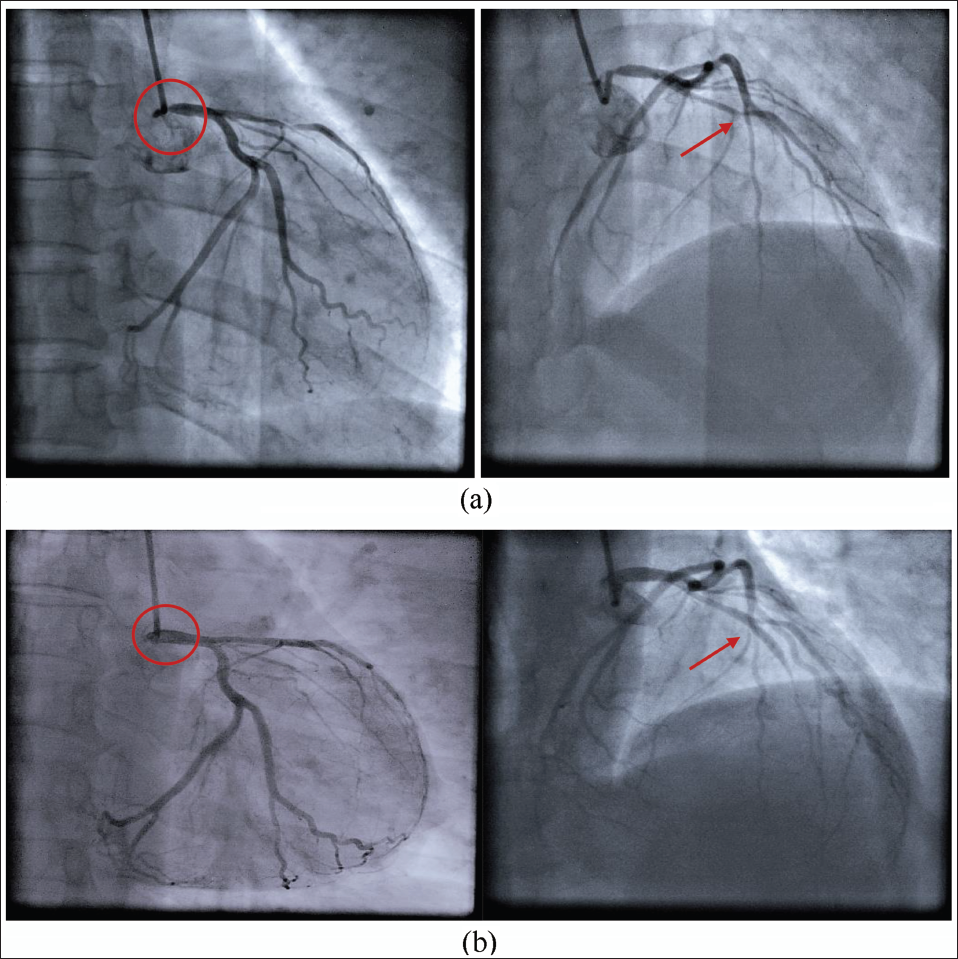
The radial route was chosen as the femoral site had a severe candida infection. The left main coronary artery (LMCA) was engaged with a 6Fr EBU, and the BMW wire was quickly advanced into the left circumflex (LCX) without contrast to avoid further damage to the LMCA. The left main ostium was predilated with a 2 × 8 mm balloon at 12 atmospheres. There was an appearance of reflux of contrast and no pressure damping. This helped us to cross the mid-LAD lesion with balloon support and another hydrophilic wire (pilot 50), keeping the initial BMW wire in the LCX. The mid-LAD was dilated with a 2 × 8 mm balloon, establishing flow in the LAD. However, this revealed another challenge: an ostial tight lesion in a significantly large diagonal. Subsequently, the LCX wire was rerouted into the diagonal, and the ostial diagonal lesion was dilated with a 2 × 8 mm balloon at 10 atmospheres, resulting in TIMI III flow. The LAD was then stented with a 2.5 × 15 mm drug-eluting stent, followed by the ostial LMCA being stented with a 4 × 12 mm drug-eluting stent. TIMI III flow was observed in all vessels with distal LAD diffuse disease (Figure 2(b)). The patient recovered from shock, and on evaluation after a month, the ejection fraction improved to 40%. As ovarian surgery could not be deferred for long, she underwent oophorectomy with single antiplatelet coverage after six weeks of stenting. Post-surgery, the patient remained stable, and under regular follow-up, she is doing well for the past three years.
Discussion
Cancer survivors face an elevated risk of developing CAD. A study focusing on childhood cancer survivors and another study involving 12,785 patients undergoing percutaneous coronary intervention (PCI) confirmed this risk. 2 Patients with cancer and acute coronary syndrome have a one-year survival rate of only 25%, with the highest cardiovascular mortality risk within the first year. 3 This risk persists for many years after cancer treatment, especially with endometrial, laryngeal, bladder, and prostate cancers. Additionally, CAD itself increases the incidence of cancer, particularly lung and colorectal cancers, due to shared risk factors.
Cancer and CAD share common risk factors, including obesity, diabetes, hypertension, hyperlipidemia, smoking, inactivity, and an unhealthy diet, with insulin resistance, atherogenic dyslipidemia, inflammation, and intestinal flora disorder contributing to these conditions. Inflammation and oxidative stress and vascular injury are established contributors to atherosclerosis, linking them to the development of cancer and CAD. A cohort study with 7,178 CAD patients over 12 years revealed a correlation between chronic low-grade inflammation and cancer incidence. 4
Chemotherapy stands as a pivotal treatment option in cancer management. However, it is crucial to note that several chemotherapeutic agents are recognized for their potential to induce cardiotoxicity. Anthracyclines such as doxorubicin and epirubicin can cause cardiotoxicity by oxidative stress, mitochondrial dysfunction, and DNA damage. 5-Fluorouracil is associated with myocardial ischemia (68%) by activation of protein kinase C, leading to coronary artery vasospasm, vascular endothelial injury, direct cardiotoxic effects, and sensitizing radiation-induced thrombogenicity. 5 Patients undergoing platinum-based chemotherapy face a 1.5–7.0 times higher long-term risk of CAD compared to controls, which is linked to endothelial toxicity, platelet activation and aggregation, and acute coronary thrombosis. Moore et al 6 noted that 18.1% of patients treated with cisplatin experienced venous and arterial thromboembolic events. Immune checkpoint inhibitors have the potential to influence the development and rupture of unstable atherosclerotic plaques by triggering the release of various inflammatory cytokines, and there is a 1% increase in the incidence of myocardial infarction. 7 People with cardiovascular risk factors are more likely to suffer from chemotherapy-related cardiotoxicity. This patient underwent six cycles of platinum therapy, which was the cause for CAD. Targeted drugs kill cancer cells. Monoclonal antibodies and tyrosine kinase inhibitors, notably VEGF inhibitors, have been shown to disrupt the cell signaling pathway closely linked to CAD, leading to complications such as hypertension, left ventricular dysfunction, and QT prolongation. 8
Coronary artery disease accelerated by radiation exposure, known as radiation-induced coronary artery disease, often occurs following extensive mantle radiation for mediastinal tumors. With approximately half of oncology patients undergoing radiotherapy at some stage of their treatment, this condition has become the second most prevalent cause of morbidity and mortality. 9 The disease process begins with oxidative stress, which subsequently leads to vascular permeability and damage to the vasa vasorum.
Our patient did not possess any risk factors associated with CAD such as diabetes, hypertension, smoking, or obesity, nor was there a significant family history of CAD. Prior to commencing chemotherapy, she underwent evaluation and was found to have normal electrocardiogram and echocardiogram with no cardiac symptoms reported. She completed six cycles of platinum-based chemotherapy without exposure to radiation. The sole risk factor leading to CAD in this patient appears to be chemotherapy, a well-documented cause of chemo-induced cardiotoxicity. However, the occurrence of severe ostial involvement, characteristic of radiation-induced CAD, is an unusual phenomenon in the context of chemotherapy.
Diagnosing CAD in cancer patients is challenging due to atypical clinical presentations, with only one-third experiencing chest pain and less than half presenting with dyspnea among those with CAD, complicating detection. 10 Cancer patients may have mostly silent ischemia or type 2 myocardial infarction, characterized by a mismatch between myocardial oxygen supply and demand. 4 Several studies have indicated that coronary revascularization enhances the safety of subsequent oncologic treatment. Balanescu et al, 11 in a study involving over 200 patients with cancer and acute coronary syndrome, proposed a survival advantage at one year when coronary angiography was conducted within 72 hours of presentation.
Precise vascular access is crucial, and a radial-first approach is favored to minimize bleeding complications, particularly in patients with significant peripheral artery disease or scarring in the inguinal region. In this case, the radial approach was employed in view of severe inguinal fungal infection and also to reduce bleeding complications. Consensus guidelines from the Society for Cardiovascular Angiography and Interventions (SCAI) 12 recommend aspirin use for all patients with platelet counts exceeding 10,000/mm3 and dual antiplatelet therapy (DAPT) with aspirin and clopidogrel if the platelet count is >30,000/mm3 and advise against using ticagrelor or prasugrel if the platelet count is below 50,000/mm3. Percutaneous coronary intervention can be performed with platelet counts exceeding 30,000/mm3, while coronary artery bypass grafting is recommended at counts >50,000/mm3. A loading dose of 300 mg clopidogrel was administered before PCI due to a platelet count >100,000/mm3. A drug-eluting stent was chosen for placement considering the ostial lesion and supported by a study by Ahmed et al, 13 which found no significant difference in all-cause mortality and bleeding risk between bare metal and drug-eluting stents.
Although Mehran et al demonstrated non-inferiority of 1–3 months of DAPT compared to longer durations, Valgimigli et al 14 showed similar outcomes with one month of DAPT compared to a three-month regimen in patients treated with drug-eluting stents. In this case, six weeks of DAPT (ecosprin 150 and clopidogrel 75) were continued, with a switch to single antiplatelet therapy (ecosprin 75 mg) before ovarian surgery due to the urgency of the procedure, followed by a three-month regimen of dual antiplatelet therapy and subsequent single antiplatelet therapy to mitigate bleeding risks. Although intravascular ultrasound or optical coherence tomography would provide valuable guidance, the emergent nature of the procedure and challenges in accessing imaging modalities during the COVID-19 pandemic led us to proceed with the intervention without imaging, which could be considered a limitation in this case report.
Prevention
Before starting cardiotoxic anticancer therapy, assess the patient’s CVD history and screen for CAD risk factors. High-risk individuals, especially those with cardiotoxic chemotherapy (anthracycline dosage of 300 mg/m2), total mediastinal radiotherapy exceeding 20 Gy, and combined therapy, should undergo annual follow-ups and physical exams per Children’s Oncology Group recommendations. SCAI recommends CCTA every five years, especially in high-risk populations. Enalapril (IMPROVE HF trial) and carvedilol (CECCY trial) showed reduction in chemotherapy-induced cardiotoxicity. 15 A Danish study found significantly lower cancer-related mortality (HR ¼ 0.85) in long-term statin users. Calcium channel blockers and nitrates prevent and treat coronary artery spasm caused by 5-fluorouracil, while hydrochlorothiazide increases squamous cell carcinoma risk. Before initiating chemotherapy, this patient underwent comprehensive evaluation and was subsequently prescribed long-term use of high-intensity statins, beta-blockers, nitrates, and angiotensin receptor neprilysin inhibitor therapy for CAD.
This case underscores several novel and instructive points:
The discovery of a severe ostial left main coronary lesion following chemotherapy, though typically associated with radiotherapy, highlights an uncommon occurrence with limited literature available. Cardiogenic shock in the setting of metastatic malignancy should not rule out PCI, as timely intervention can enhance the patient’s quality of life by enabling appropriate therapy for the carcinoma.
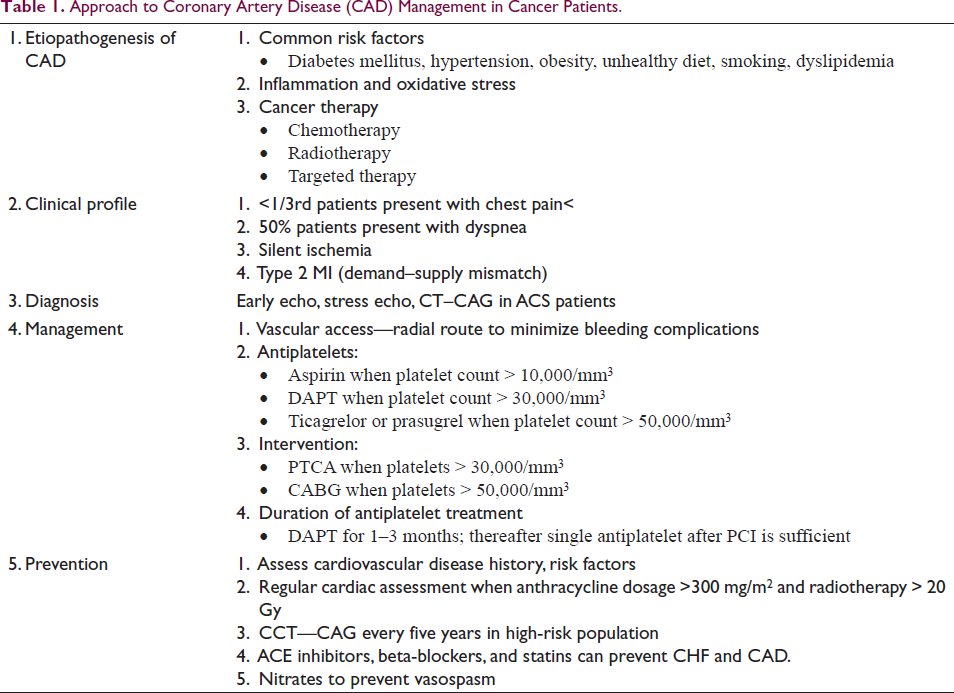
The key aspects of cardiovascular disease associated with cancer are emphasized in Table 1.
Approach to Coronary Artery Disease (CAD) Management in Cancer Patients.
Conclusion
Tailoring coronary care for cancer patients through a multidisciplinary approach is essential for enhancing outcomes. As there are no clear protocols for CAD management in cancer patients, a multidisciplinary collaboration is needed to formulate reasonable strategies for the diagnosis and treatment in these patients. Further, detailed cancer surveillance and possible interventions in the CAD population should be implemented to reduce cancer-related morbidity and mortality.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval was not applicable, as it is a case report and was reported retrospectively.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Patient consent was taken.