
Abstract
A stepwise analytic approach is needed to decipher tachyarrhythmia electrocardiograms. It is also important to be able to promptly recognize certain characteristic patterns described in some classical arrhythmias. Knowledge of these unique electrocardiogram morphologies and the underlying reasons for them help in quick diagnosis and appropriate management.
Introduction
A systematic approach is needed while assessing tachyarrhythmia electrocardiograms (ECGs) and for this purpose a stepwise analysis is often recommended which includes classifying into broad or narrow QRS tachycardia, identifying p waves, looking at QRS morphology and durations of deflections within the QRS. However, it is also important to be able to recognize characteristic patterns of certain classical arrhythmias as immediate recognition would help select the most appropriate therapy for that arrhythmia. Here we describe one such case.
Case Report
A 27-year-old male patient presented with a history of episodic palpitations, shortness of breath and dizziness. He had no chest pain or syncope. There was no other significant past medical, family, or surgical history. He was a non-smoker and denied any use of alcohol or illicit drugs.
General and cardiovascular examinations were essentially normal. An echocardiogram showed no evidence of any structural heart disease. He had also undergone a coronary angiogram elsewhere which was normal.
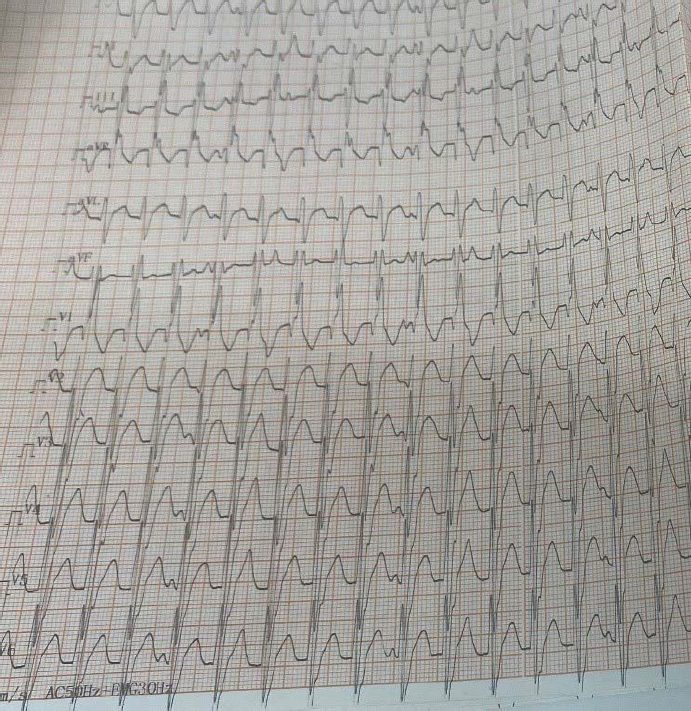
An ECG taken during an episode of palpitations is shown in Figure 1. What is the diagnosis, what is the mechanism of this arrhythmia and how should this patient be treated?
Discussion
The ECG shows a broad QRS tachycardia with right bundle branch block (RBBB) morphology and left axis deviation. The differential diagnosis for any broad QRS tachycardia includes ventricular tachycardia (VT) and supraventricular tachycardia (SVT) with aberrancy (including pre-excited tachycardia). Careful inspection of the 12-lead ECG shows AV dissociation (Figure 2A, p waves indicated by arrows) with more QRS than p waves, indicating VT. Also, the characteristic morphology of RBBB with left axis deviation in a young patient with a structurally normal heart should make one consider idiopathic left fascicular VT.
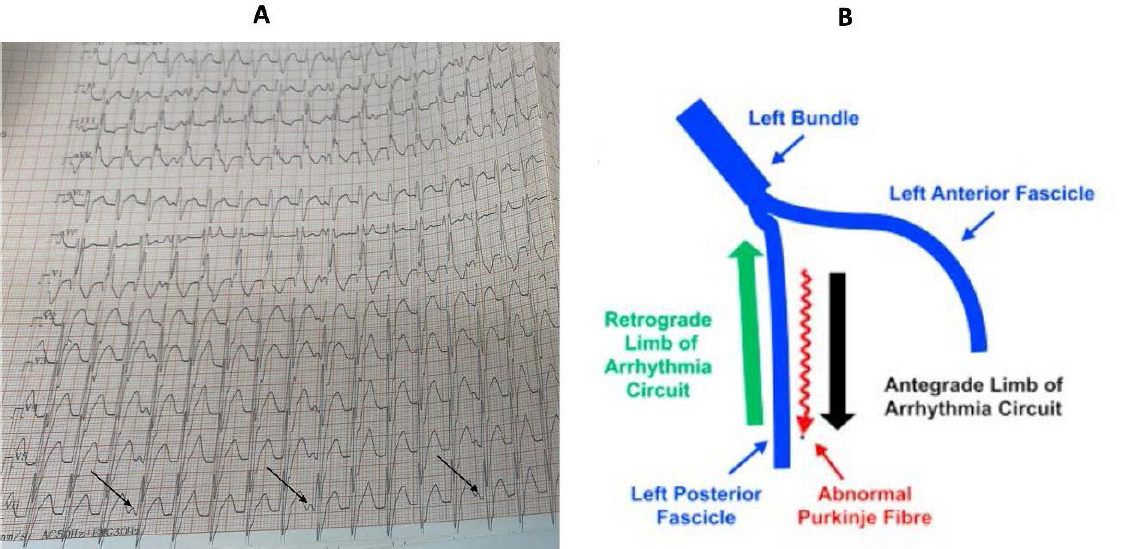
Fascicular VT is due to a unique re-entrant circuit which involves the normal conduction system of the heart. Three forms of fascicular VT have been described, namely left posterior fascicular, left anterior fascicular and upper septal VT. Left posterior fascicular VT is the most common variant where the left posterior fascicle is involved as the retrograde limb of the re-entrant circuit, with the antegrade limb being formed by slowly conducting Purkinje tissue adjacent to the fascicle. 1 The classically described re-entrant circuit of left posterior fascicular VT is shown in Figure 2B. This gives rise to the characteristic ECG morphology of this VT with RBBB and left axis. Furthermore, this VT is uniquely sensitive to verapamil, making it the drug of choice for the pharmacological treatment of this VT. Thus, making an accurate, rapid diagnosis by recognising the ECG appearance will help initiate the correct drug immediately, potentially avoiding more toxic alternatives such as amiodarone. Idiopathic fascicular VT is also eminently treatable by catheter ablation, thus offering the possibility of a cure and avoidance of chronic medication in these often-young patients.
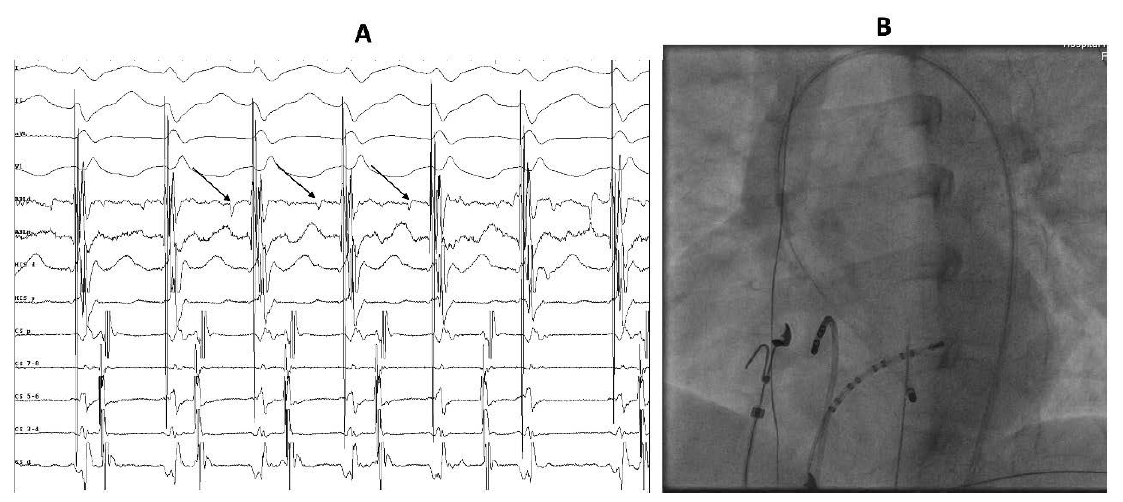
In the present case, the patient had been treated elsewhere with beta-blockers and diltiazem; however, he preferred to undergo a definitive procedure rather than take drugs on a long-term basis. After obtaining informed consent, an electrophysiology study was performed which confirmed the diagnosis of left posterior fascicular VT. Ablation is typically performed at the mid-distal third of the left ventricular (LV) septum posteriorly where characteristic diastolic pre-Purkinje and pre-systolic Purkinje potentials are obtained from the slow conducting critical part of the re-entrant circuit (electrograms from the ablation site and fluoroscopic location of the ablation catheter are shown in Figure 3). The VT was successfully ablated at that site; post-procedure ECG showed sinus rhythm (Figure 4).
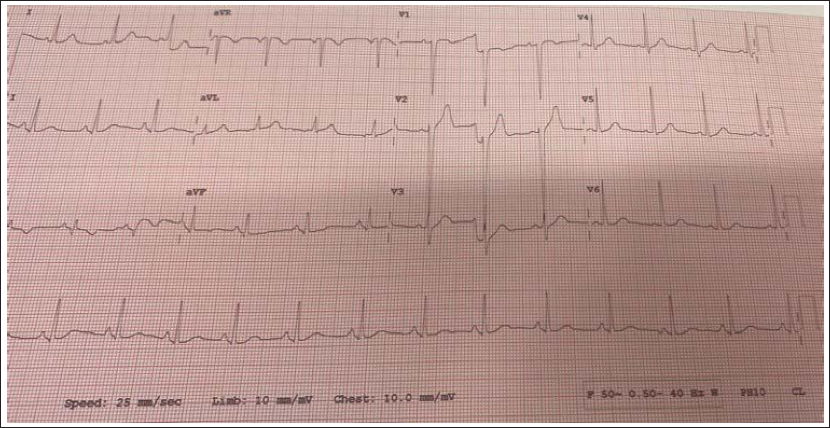
The patient has remained symptom-free since the procedure and is off all drugs.
Conclusion
Idiopathic left fascicular VT is a characteristic VT involving part of the conduction system in its re-entrant circuit and can be successfully treated with catheter ablation. This case highlights the importance of recognising and understanding typical ECG patterns in broad QRS tachycardia which will enable a quick diagnosis and appropriate management.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.