
Abstract

A 24-year-old female patient, without family or personal pathological history, came to the outpatient service because of frequent episodes of palpitations accompanied by generalized weakness and dizziness without loss of consciousness, a duration of several hours, and their self-limited nature. A 12-lead electrocardiogram was performed, which showed sinus rhythm, 88 beats per minute, a short PR interval, a widened QRS complex with initial slurring, and repolarization changes, findings that are consistent with that of Wolff–Parkinson–White (WPW) pattern, possibly right inferior paraseptal atrioventricular accessory pathway (Figure 1A).
Serial Periprocedural Electrocardiographic Changes. (A) 12-Lead Electrocardiogram in Initial Outpatient Assessment Shows a WPW Pattern with Repolarization Changes, QRS Axis of 30º. Possibly Right Inferior Paraseptal Atrioventricular Accessory Pathway. (B) 12-Lead Electrocardiogram After Radiofrequency Ablation Shows Normal PR Interval and QRS Complex but T-Wave Inversion in DII, DIII, and aVF Leads, QRS Axis of 60º.
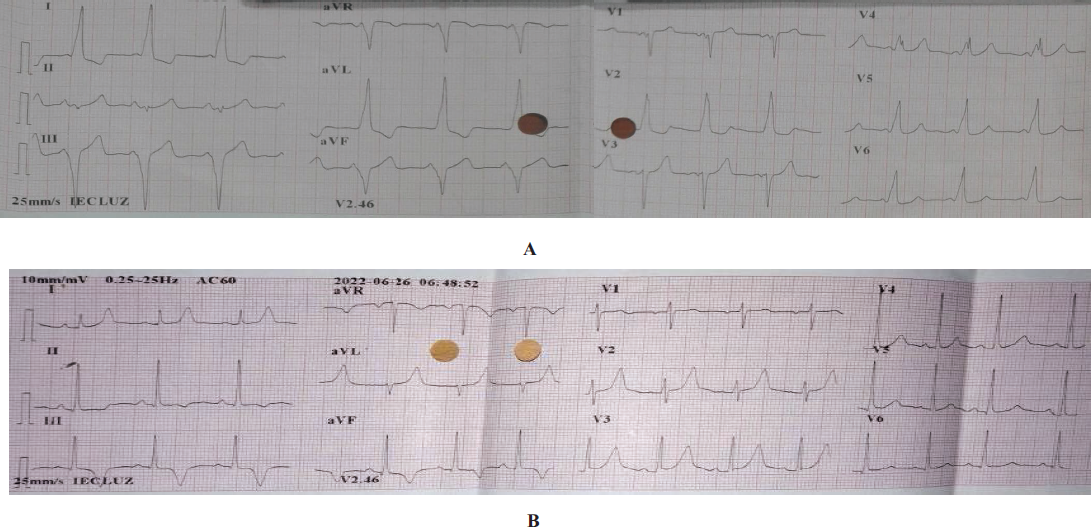
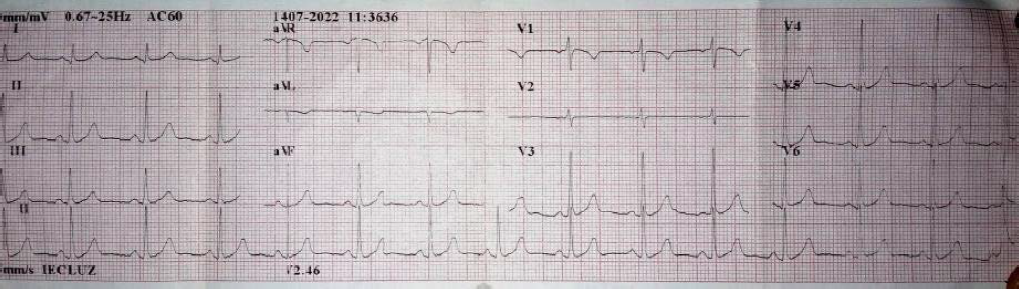
During the procedure, a right inferior paraseptal atrioventricular (previously called right posteroseptal) accessory pathway was found, with right atria stimulation radiofrequency energy applied with fixed cycles of 500 ms, acquiring atrioventricular (AV) separation and dissociation of ventriculoatrial retroconduction, and an electrocardiogram in sinus rhythm with 88 beats per minute, a PR interval of 160 ms, a QRS complex of 80 ms, a QRS axis of 60°, and symmetrical T-wave inversion (TWI) in DII, DIII, and aVF leads (Figure 1B). Radiofrequency ablation was performed without atrial pacing. The patient was discharged without instantaneous complications. During the follow-up evaluation, 10 days after the procedure, the patient was asymptomatic, with no new episodes of palpitations, and an electrocardiogram in sinus rhythm with 83 beats per minute, PR interval of 160 ms, QRS complex of 80 ms, QRS axis of 60°, and normal repolarization changes (Figure 2). The patient was managed conservatively due to a suspicion of cardiac memory phenomenon .
Electrocardiogram in Follow-up Assessment 10 Days After the Procedure, Shows Normal PR Interval and QRS Complex Without T-Wave Change.
The secondary changes in ST segment and T-wave are due to alterations in the ventricular activation sequence. When this is normalized, the repolarization changes are immediately reversed. Other T-wave changes occur in the setting of intermittent left bundle branch blocks, fascicular blocks, nonspecific intraventricular conduction disturbances, ventricular arrhythmias, artificial ventricular pacing, and ventricular preexcitation. In each of these scenarios, where there is abnormal ventricular activation, the sudden or progressive recovery of the normal depolarization sequence is not always supported with T-wave polarity normalization but rather by a persistent polarity alteration, generally compatible with the polarity of the aberrant QRS complexes that condition them. 1
The cardiac memory phenomenon was described as early as 1915 by White, but its name dates to 1982 after the experimental work of Mauricio Rosenbaum, who proposed the three premises as follows:
In sinus rhythm, the T-wave direction corresponds to the abnormal activation of the QRS complex. The amplitude of T-wave memory increases as the abnormal conduction is persistent. Repeated episodes of abnormal activation after complete T-wave normalization result in the accumulation of more rapid and prominent T-wave changes.
2
The molecular phenomena involved are not only limited to electrophysiological changes but also to mechanical changes, which in turn are divided into short-term and long-term modifications, according to the molecules involved (ion channels, receptors associated with transmembrane currents, redistribution of gap junctions, receptors activated by stretch, and stimulation of transcription factors). 3
In the context of WPW syndrome, previous studies have shown that TWI is next to abnormal ventricular activation sequences, both overt WPW syndrome and concealed connections or intermittent WPW, the latter identified using the QRST isointegral maps. 4 Similarly, the T-wave axis after ablation is related to the preexisting QRS complex, previous abnormal ventricular activation sequence, and location of the accessory pathway, regardless of the degree of preexcitation. In addition, the magnitude of the QRS-T angle is related to changes in the QRS axis due to ablation, normalizing during weeks or months associated with progressive cardiac remodeling. 5
The case study presented shows the electrocardiographic evolution of a patient with WPW syndrome undergoing radiofrequency ablation, specifically the TWI in DII, DIII, and aVF leads associated with abnormal ventricular activation through a right inferior paraseptal atrioventricular accessory pathway (connection location) and to the QRS axis change, whose normalization occurred within 2 weeks.
The cardiac memory phenomenon is a common electrocardiographic finding in patients with WPW syndrome undergoing radiofrequency ablation therapy (45%–96%) due to high activation recovery interval dispersion that can persist between 1 and 3 months after the procedure.6, 7 Although there are no official electrocardiographic criteria to distinguish this phenomenon, it has been proposed that the combination of a positive T wave in aVL, a positive or isoelectric T wave in DI, and the largest inverted T wave of any precordial lead being deeper than in DIII has high sensitivity (92%) and high specificity (100%) for cardiac memory, allowing discrimination of cardiac ischemia. 8 However, these criteria may vary depending on the location of the source that promoted the abnormal ventricular activation. In fact, according to Trajkov et al., 9 TWI in inferior leads with disappearance of the delta wave after ablation of the right posteroseptal accessory pathway would be considered an important marker of successful ablation.
Therefore, from a practical perspective, it is important to differentiate ischemic TWI from secondary T wave changes, particularly in subjects who have recently undergone an invasive procedure, consistently individualizing the clinical and electrocardiographic evaluation. In summary, the cardiac memory phenomenon consists of persistent TWI after the normalization of an abnormal ventricular activation sequence. This is a common finding in patients with WPW syndrome undergoing radiofrequency ablation and should be considered in subjects with a history of ventricular activation disorder and a low probability of myocardial ischemia or ventricular hypertrophy.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.