
Abstract
Thyrotoxic hypokalemic periodic paralysis is a rare but life-threatening complication of hyperthyroidism characterized by hyperthyroidism, hypokalemia, and transient episodes of acute proximal muscle weakness. Incidence of thyrotoxic hypokalemic periodic paralysis is more common in Asian men and extremely rare in blacks. The basic mechanism includes thyrotoxicosis-induced hypokalemia leading to muscle weakness associated with respiratory insufficiency and fatal arrhythmias. We present a rare case of atrial arrhythmia as the initial presentation of thyrotoxic hypokalemic periodic paralysis.
Background
Hyperthyroidism can lead to a rare neurological complication called thyrotoxic hypokalemic periodic paralysis (THPP), a rare but fatal complication. Thyrotoxic hypokalemic periodic paralysis is a sporadic disease characterized by low levels of serum potassium, which causes episodes of flaccid muscle weakness. 1 The pathophysiologic mechanism is hyperthyroidism causing catecholamine surge leading to the intracellular passage of potassium. 2 This leads to an increase in the number and activity of sodium/potassium ATPase, and it manifests as paralysis. Thyrotoxic hypokalemic periodic paralysis is very frequently associated with respiratory insufficiency and arrhythmias, making it fatal. We present a rare case of atrial arrhythmia, which is the initial presentation of THPP.
Case Presentation
A 38-year-old man presented to the emergency department with a 2-day history of palpitations and weakness in both lower limbs. The palpitations were sudden in onset, short, and not associated with syncope, presyncope, or angina. The weakness was insidious onset and started in both lower limbs with normal bowel and bladder habits. Vitals on presentation showed a blood pressure of 130/70 mm Hg, heart rate of 140 bpm, oxygen saturation of 99%, and afebrile. On neurological examination, motor strength in both lower limbs was 2/5 without sensory loss. Deep tendon reflexes were diminished bilaterally. Bilateral plantars were mute. Cranial nerves examination was normal. On cardiovascular examination, the patient was found to have tachycardia without any murmurs. There was no significant history.
Investigations
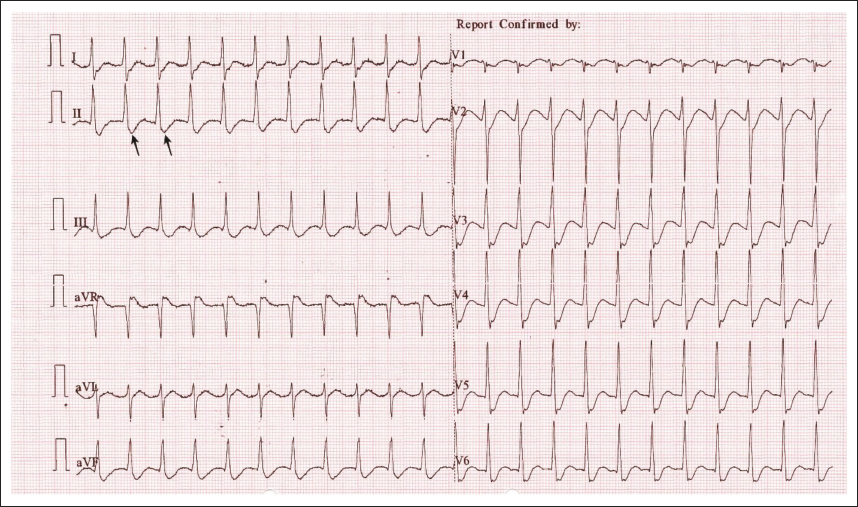
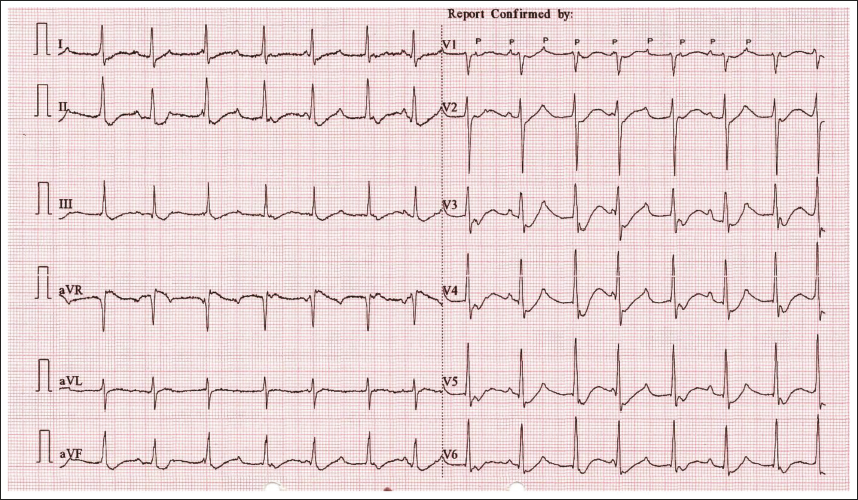
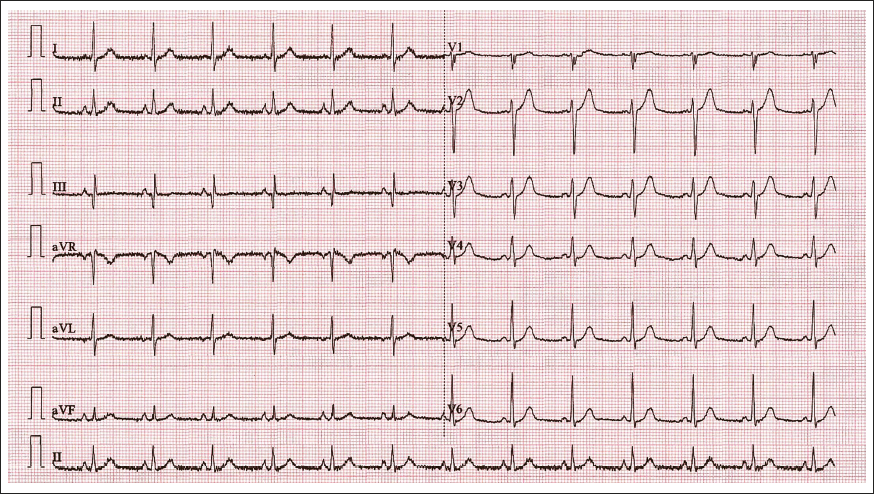
Electrocardiography (ECG) revealed a narrow complex, short RP tachycardia consistent with atrioventricular nodal re-entry tachycardia (Figure 1). As the patient was hemodynamically stable, adenosine was tried. Post-adenosine, the short RP tachycardia converted to atrial tachycardia (AT) with variable conduction (Figure 2). Arterial blood gas analysis done in emergency revealed electrolytes disturbance in the form of severe hypokalemia. Laboratory tests were done for serum potassium levels, which revealed severe hypokalemia (1.2 mEq/L, reference range: 3.5–5 mEq/L), creatinine levels of 0.8 mg/dL (reference range: 0.7–1.3 mg/dL), and hemoglobin levels of 15 gm/dL (reference range: 14.0–17 gm/dL). Thyroid function tests reported a lower thyroid-stimulating hormone (TSH) level <0.01 mIU/L (reference range: 0.5–5 mIU/L), and higher levels of free tri-iodothyronine 55 pmol/L (reference range: 3.1–6.8 pmol/L) and free thyroxine 90 pmol/L (reference range: 12–22 pmol/L). Anti-thyroid peroxidase (TPO) and TSH receptor-blocking antibody levels were higher with levels of 214 IU/mL (reference range: < 9 IU/mL) and 33 IU/L (reference range 0.79–3.47 IU/L), respectively. His other biochemical findings were within the normal range. His chest X-ray and echocardiogram did not demonstrate any abnormality.
Narrow complex short RP tachycardia with 140 bpm (Black arrow pointing p waves in lead III).
Atrial Tachycardia with variable conduction (not all P waves followed by QRS and variable RR interval)
Treatment
Intravenous potassium chloride (KCl) was administered to treat the hypokalemia. Oral KCl supplementation was started and the potassium levels gradually improved to 4 mEq/L. The patient showed rapid improvement in lower limb weakness. Treatment for hyperthyroidism was initiated with carbimazole (20 mg orally twice daily) and a high-dose nonselective beta-blocker, propranolol (40 mg orally every 8 hours), to inhibit the peripheral conversion of T4 to T3.
Outcome and Follow-up
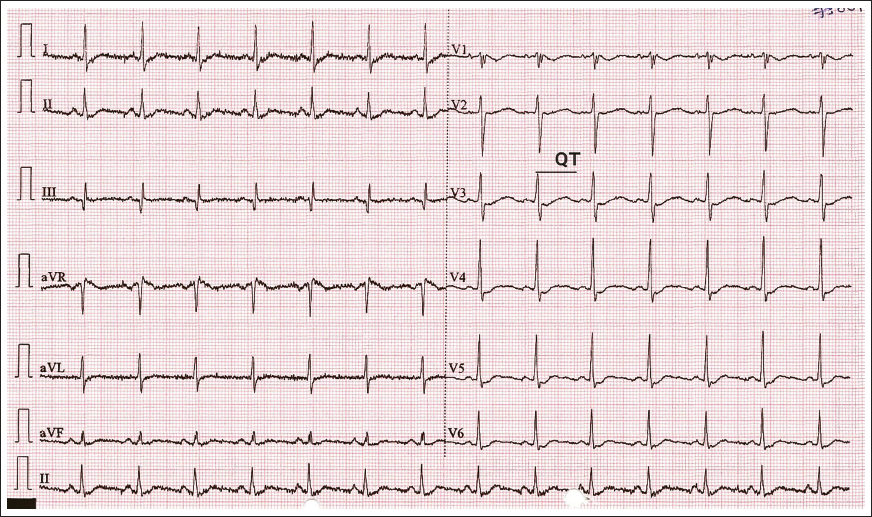
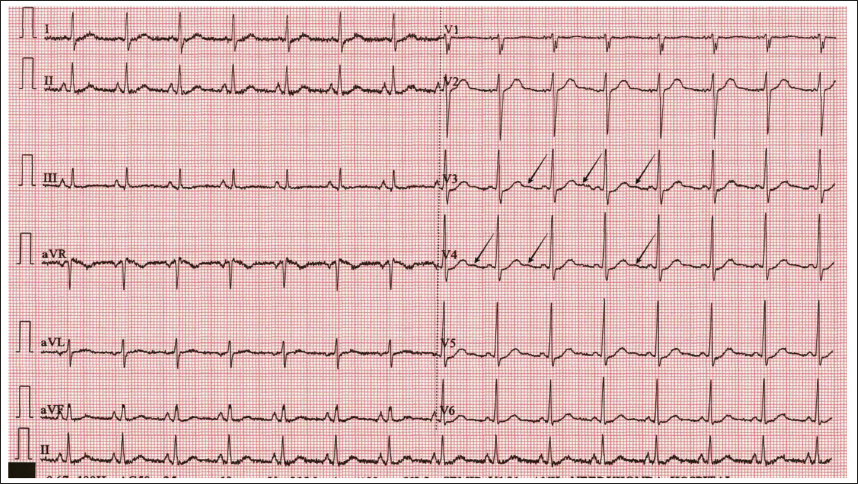
Cardiac arrhythmias resolved promptly after initiation of treatment. On day 2, ECG showed “U” waves with QT prolongation (Figures 3 and 4). Electrocardiography completely normalized on day 3 (Figure 5). His general condition improved without any additional complaints, and he was discharged on day 4. On follow-up, he did not have any recurrence and his investigations revealed significant improvement.
ECG showing prolonged QT with QTc 569 milliseconds.
“U” waves in leads V3, V4 (pointed with black arrows).
Normal ECG.
Discussion
Thyrotoxic hypokalemic periodic paralysis manifests with sporadic episodes of hypokalemia, muscle paralysis, and sometimes life-threatening arrhythmias. The basic pathology in THPP is thought to be due to the disequilibrium between intra- and extracellular potassium values. This condition is related to the increased number, and activity of Na/K/ATPase pump secondary to thyrotoxicosis with a resultant increase in intracellular potassium inflow. 1
The case presented here is consistent with the definition of THPP since the patient had elevated thyroid hormone levels, lower serum potassium, and muscle weakness. Abnormal ECG findings are found in most patients with THPP either due to the elevated sympathetic activity caused by the excess thyroid hormones or changes related to hypokalemia. 3 Arrhythmias are common with atrial arrhythmias occurring frequently; however, ventricular arrhythmias such as ventricular fibrillation can also occur. This patient had AT, prominent U waves (best seen in the precordial leads V2-V4), apparent long QT interval due to the fusion of T and U waves on serial ECG, and AV blocks, which may be due to hypokalemia.
The factors precipitating the paroxysomal attacks in susceptible patients were emotional stress, traumatic events, infections, excess alcohol intake, excess carbohydrate intake, heavy exercise, and androgenic effects, especially in males. 2 Excess intake of carbohydrates leads to excess insulin production, which induces higher beta-adrenergic activity. This in turn increases intracellular uptake of potassium leading to hypokalemia. In our case, the patient was male, androgenic effect might be present, and he also gave a history of excess alcohol intake one day prior to the presentation. One should be attentive to cardiac arrhythmias and respiratory problems in the cases of hypokalemia. Although our patient had hypokalemia, he presented with arrhythmia and muscle paralysis without respiratory abnormalities.
The most common etiology reported in patients who were diagnosed with THPP is Graves’ disease. Other less common etiologies include toxic nodular goiter, thyroiditis, and TSH-secreting adenoma. 4 In our case, TPO and TSH receptor-blocking antibody levels were high, and thyroid ultrasound showed a mildly enlarged thyroid gland with heterogeneous echotexture and diffusely increased vascularity, without evidence of thyroid nodules, consistent with Graves’ disease. Management of THPP includes treatment of hypokalemia and treatment of hyperthyroidism. Treatment of hypokalemia can be instituted based on the clinical manifestations of the patient through oral route or intravenous route in compliance with relevant protocols. For long-term effective treatment in cases with THPP, euthyroid should be ensured with control of hyperthyroidism by medical therapy with antithyroid drugs, nonselective beta-blockers, radioactive iodine, or surgery (thyroidectomy or subtotal thyroidectomy).
Conclusion
The basic pathology behind THPP is hyperthyroidism leading to hypokalemia and fatal complications. Often signs of hyperthyroidism are overt in THPP and pose a diagnostic challenge. However, having a comprehensive approach in patients presenting with muscle paralysis and hypokalemia, considering THPP would help in early diagnosis and treatment, to prevent fatal complications.
Learning Points
Early accurate diagnosis and prompt treatment for THPP is lifesaving.
To recognize THPP as a potential cause of atrial arrhythmias.
To understand and list the complications associated with THPP.
List of Abbreviations
ABG: Arterial blood gas
AT: Atrial Tachycardia
AVNRT: Atrioventricular nodal reentry tachycardia
ECG: Electrocardiography
FT3: Free triiodothyronine
FT4: Free thyroxine
KCL: Potassium chloride
TFT: Thyroid function test
THPP: Thyrotoxic hypokalemic periodic paralysis
TSH: Thyroid-stimulating hormone
Footnotes
Acknowledgment
The authors would like to thank the patient for his continuous support.
Authors’ Contribution
S.K.P. and R.C.K. equally participated in the analysis and interpretation of data, preparation of manuscript, and critically reviewed it for intellectual content and gave final approval for submission.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The Institutional Ethics Committee approved the case report before publication, and written informed consent was obtained from the patient.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
Patient consent was obtained for publication.