
Abstract
Background: Complex cardiac surgery in neonates and small-weight babies is a challenge. In addition to the surgical expertise and skill required, accurate diagnosis, management of anesthesia, perfusion, and postoperative critical care are equally challenging.
Methods: We have analyzed the data of 4 different examples of complex cardiac surgery in neonates and small-weight babies from February 2012 to July 2019 in our unit. The first group included 118 cases of arterial switch operations for transposition of great arteries with and without ventricular septal defect (group 1). The second group included 52 patients of aortic arch repair from midline using selective cerebral perfusion avoiding total circulatory arrest (group 2). The third group included 75 patients of repair of coarctation of aorta from thoracotomy using the modified end-to-side technique (group 3). The fourth group included 40 neonates and small-weight babies who underwent repair of total anomalous pulmonary venous connection (group 4).
Results: In group 1, there was hospital mortality in 6 babies. In group 2, there was no hospital mortality. In group 3, there was 1 hospital death; in group 4, there were 5 hospital deaths. The major contributing cause of death was respiratory or blood-borne infection causing respiratory issues leading to prolonged ventilation. Left diaphragm palsy contributed to morbidity and eventual death in 2 babies. Only 2 patients required tracheostomy to wean off the ventilator.
Conclusions: In the present day, it is possible to achieve satisfactory results with acceptable mortality in neonatal cardiac surgery. Morbidity associated with very early repair in neonatal age, low weight, and infection-related issues is manageable with good outcomes.
Introduction
It is a well-known fact that operating on a small-weight baby/neonate with congenital heart disease is a challenge. In the present-day practice, more focused subspecialities have emerged in this field that include pediatric/neonatal cardiac surgery, pediatric cardiology, pediatric cardiac anesthesia and critical care, and pediatric cardiac perfusion technology. Apart from the surgical skill and expertise required, accurate diagnosis by the pediatric cardiologist, careful intraoperative anesthesia and perfusion management, and postoperative critical care are equally important to run a successful neonatal cardiac surgical program. Significant progress has been made in neonatal cardiac surgery in the recent two decades.1, 2, 3, 4 The mortality and morbidity after neonatal cardiac surgery have decreased considerably in the recent past.5, 6 Biventricular complete repair in neonates and small-weight babies can be performed with good early- and mid-term results. 7 The hospital mortality after neonatal cardiac surgery from the European Association for Cardio-Thoracic Surgery (EACTS) Congenital Database was 10.7%. 8 Similarly, the Society of Thoracic Surgeons (STS) Congenital Heart Surgery database reported a mortality rate of 10.1%. 8 The essential factor for improved results in neonatal cardiac surgery is the collaborative effort of surgeons, cardiologists, anesthesiologists, and postoperative critical care specialists acting as a comprehensive team. 9
Even though neonatal cardiac surgery can be done with acceptable mortality, there is significant morbidity associated with these operations in low-weight babies. However, in today’s practice, this morbidity can be appropriately managed. 10 In a country like India, it is a challenge to establish a neonatal cardiac surgical program in a limited resources environment. This is especially important when a pediatric cardiac intensive care unit (ICU) is planned because of the requirement of a dedicated ICU in this setting. 11 If the surgical outcomes in these babies have to be good, a dedicated unit has to work out its own ways to fight the odds and tackle the problems associated with late presentation, malnutrition, respiratory and blood-borne infections, and limitations of financial resources to perform these complex operations.12, 13, 14
Methods
Organizing the Appropriate Infrastructure and Managing Administrative/Social Issues
The appropriate infrastructure for a neonatal cardiac surgical program in a hospital includes the following:
Modular operating theatre room with laminar flow and adequate air-conditioning with the ability to control the temperature as and when required. In other words, when the neonate arrives in the operating room, the ambient temperature should not be cold and should be appropriate so that there is no metabolic derangement while induction and anesthesia. After a cardiopulmonary bypass (CBP) when the baby is being cooled, the ambient temperature should also be cool and during rewarming it must be appropriately adjusted. In addition, having a warming and a cooling blanket on the operating table to control the surface temperature of the baby is essential. State-of-the-art anesthesia machine and heart–lung machine for perfusion. A dedicated postoperative ICU with adequate bed-to-bed spacing to prevent infections. The ambient temperature in the ICU needs to be adjusted to keep it optimum. A neonate after a complex cardiac surgery will require an isolation room with separate inlet and outlet ducts for air-conditioning. Adequately equipped blood bank that is capable of providing various components of blood such as the packed cells, platelet concentrates, and fresh frozen plasma. These are essential for handling postoperative bleeding in the operating room in these babies. Financial constraint is the most challenging problem to handle when we operate on small-weight neonates. Families from low-income group have to generate finances and need additional financial support from various sources; equally, the hospital has to be considerate and needs to encourage the unit for operating a patient from such income groups. Careful management of the baby from the diagnosis to the surgery and then in the ICU involves dedicated team work and organizational skills at all levels. Organizing an emergency switch operation in a busy ICU involves careful planning and several adjustments at all levels without affecting the overall care in the ICU.
Patient Profiles and Surgical Techniques of Specific Complex Cardiac Surgical Procedures
We have analyzed the data of 4 different examples of complex cardiac surgery in neonates and small-weight babies from February 2012 to July 2019 in our unit.
Arterial Switch Operation for Transposition of Great Arteries (Group 1)
Transposition of Great Arteries (TGA) (Group 1)
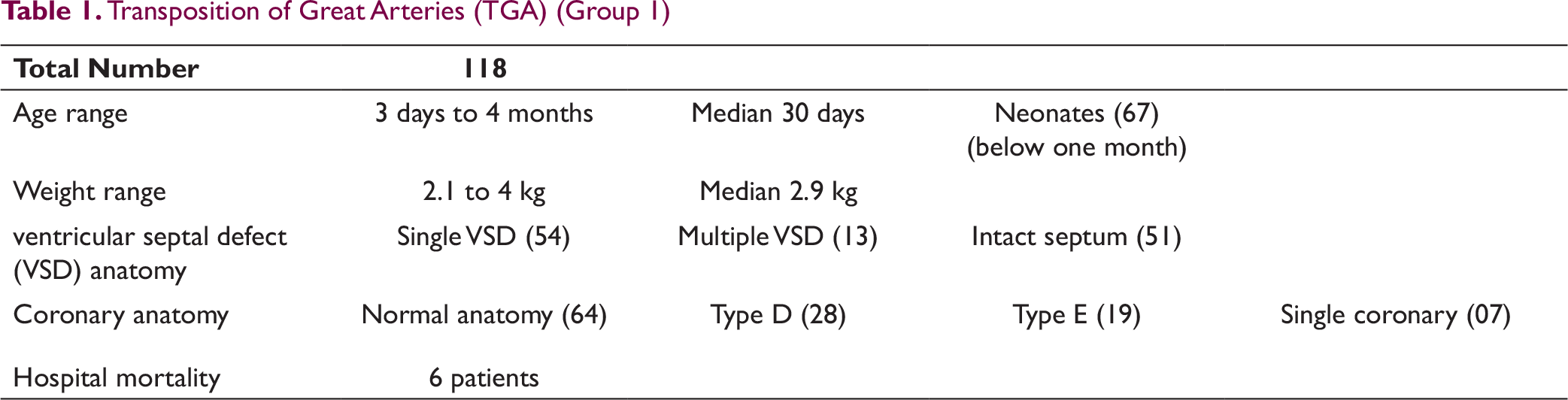
51 patients had intact ventricular septum, 54 patients had single ventricular septal defect (VSD), and 13 patients had multiple VSD. Among the intact septum group, 13 patients underwent balloon atrial septostomy, 4 patients underwent patent ductus arteriosus stenting and 2 patients underwent left ventricular (LV) training with pulmonary artery (PA) banding.
Coronary Anatomy: 64 patients had normal coronary anatomy, while 54 patients had abnormal coronary anatomy. Among them, 28 patients had type-D anatomy, 19 patients had type-E anatomy, and 7 patients had single coronary anatomy. The single coronary anatomy includes very close orifices of left and right to the commissure, wherein the commissure was detached and a wide cuff was taken as a single coronary artery.
In type-D anatomy, the button of the right coronary artery + left circumflex artery was implanted high into the neoaortic anastomosis and the left anterior descending artery button was implanted as a separate punch hole using aortic punch. In type-E anatomy, the anterior button of the right coronary artery + left anterior descending artery was implanted as a punch hole using aortic punch and the posterior left circumflex artery was implanted high into the neoaortic anastomosis. In single coronary artery anatomy, the anterior origin button was implanted with a wide cuff into a generous V incision in the neoaorta. The posterior-origin single coronary artery button was implanted with an anterior pericardial hood into the neoaorta.
Ventricular Septal Defect: The single perimembranous VSD was repaired from the right atrium. The outlet VSD was repaired either from the neo-PA or from the neoaorta. Multiple VSDs were repaired as follows: The single large VSD was repaired with a pericardial patch and the others with endothelial suturing.
Aortic Arch Repair from Midline (Group 2)
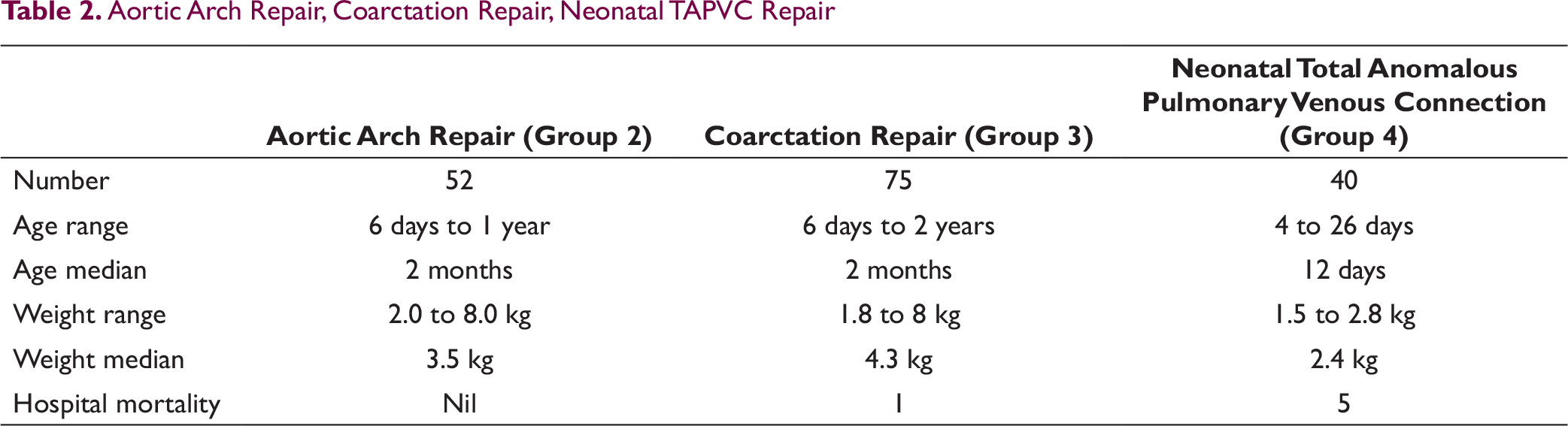
From February 2012 to September 2019, 52 patients underwent aortic arch reconstruction without the use of deep hypothermic circulatory arrest using selective cerebral perfusion by direct innominate artery cannulation. The age range was from 6 days to 1 year (median 2 months). The weight range was from 2.0 to 8.0 kg (median 3.5 kg; Table 2).
Repair of Coarctation of Aorta from Thoracotomy (Group 3)
Between February 2012 and July 2019, 75 patients underwent repair of coarctation of aorta from thoracotomy without the use of CBP (Table 2). The age of the patients ranged from 6 days to 2 years (median 2 months), and the weight ranged from 1.8 to 8.0 kg (median 4.3 kg). We published this experience earlier from our unit under the title “Early outcomes of modification of end to side repair of coarctation of aorta with arch hypoplasia in neonates and infants.” 16
In this group of patients, there was no intracardiac defect and the coarctation of aorta was an isolated lesion associated with arch hypoplasia. We modified the technique of repair of coarctation of aorta from an extended end-to-end anastomosis to an end-to-side repair. This modification helped us to prevent restenosis of the coarctation which was seen in a few patients that underwent extended end-to-end anastomosis. By using the modified end-to-side repair, the descending aorta was mobilized aggressively and moved to anastomose to the arch and the side of the ascending aorta reaching almost to the base of the innominate artery. After this modification, our patients did not develop any restenosis of the lesion. This was discussed in our publication. 16
Repair of TAPVC in Neonates (Group 4)
In neonates with total anomalous pulmonary venous connection (TAPVC), we repair the lesion using moderate hypothermia without the use of deep hypothermic circulatory arrest (Table 2). Between February 2012 and July 2019, 40 neonates underwent repair of TAPVC in our unit. The age of the neonates ranged from 4 to 26 days (median 12 days). The weight ranged from 1.5 to 2.8 kg (median 2.4 kg).
Aortic Arch Repair, Coarctation Repair, Neonatal TAPVC Repair
Results and Gratification
TGA Group (Group 1)
Outcomes and Mortality
There was hospital mortality in 6 patients. 2 patients died after discharge at home after duration of 2 months due to sudden unexplained events. Both the patients had good LV function before discharge.
Among the hospital mortality, the major number of deaths occurred in the first 2 years of our experience in this hospital.
2 patients had low cardiac output related to abnormal coronary anatomy (type E in one patient and type D in another patient) and died on the same postoperative day. Both these deaths occurred in the first 2 years between February 2012 and July 2014. 1 patient had left diaphragmatic palsy that required diaphragmatic plication. The baby died due to persistent lung infection secondary to lung collapse that did not recover. 1 patient had a regressed LV with intact septum and died due to low cardiac output after 48 hours. 2 patients had prolonged ventilation due to persistent lung issues associated with culture-positive lung infection and died due to sepsis. Both these patients had low weight (2.2-2.4 kg).
Aortic Arch Repair from Midline (Group 2)
In this group, the median duration of the antegrade cerebral perfusion was 35 minutes (range: 28-45 minutes). There was no operative mortality. 10 patients had documented evidence of preoperative infection in the form of positive blood culture and endotracheal tube culture. Among them, 2 patients had to be taken up for surgery on a ventilator. These 2 patients required prolonged ventilation and needed a tracheostomy for weaning off the ventilator and had the longest postoperative stay in the hospital (72 and 88 days, respectively).
The median duration of ventilation in the postoperative period was 38 h (range: 11-95 h) in the rest of the patients. In 20 patients, noninvasive ventilation was used after extubation to manage respiratory issues. The median duration of hospital stay was 14 days (range: 8-88 days).
Repair of Coarctation of Aorta from Thoracotomy (Group 3)
1 neonate in this group died in the postoperative period due to a cause not related to the repair of coarctation. This neonate had to be taken up on an emergent basis on ventilator and was proven to have culture-positive infection in the lungs. The neonate died in the postoperative period due to sepsis.
After using the modified end-to-side repair technique, there was no incidence of restenosis in this group of patients. All patients were doing well in follow-up. There were no respiratory issues like obstruction of the left bronchus related to extensive mobilization of the descending aorta from the posterior mediastinum and pulling it up aggressively into the anterior mediastinum to anastomose in an end-to-side fashion.
Repair of TAPVC in Neonates (Group 4)
In this group, there were 5 hospital deaths in the postoperative period. 2 patients among them had obstructed infradiaphragmatic TAPVC and both the patients had a small common pulmonary venous chamber associated with small pulmonary veins; the preoperative chest X-ray had a reticular pattern type of lung parenchyma. Both patients had persistent pulmonary hypertensive crisis that was not responding to management. In the other 3 patients, 1 had an obstructive supracardiac TAPVC and the other 2 had obstructive infradiaphragmatic TAPVC. All the 3 patients had to be placed on a ventilator and had preoperative positive endotracheal tube cultures. They had persistent lung issues related to infection in the postoperative period and died.
In the remaining patients, the median duration of ventilation in the postoperative period was 84 h (range: 52-110 h). In all patients, noninvasive ventilation was used after extubation and was gradually weaned off after decreasing cycles. The median duration of hospital stay was 20 days (range: 14-30 days). No patient in this group required tracheostomy for weaning off the ventilator.
Discussion
Lessons Learnt Overtime in Our Unit from the Surgical Standpoint for Arterial Switch Operation
A neonate with an intact septum and less than 1 week of age, especially 2 or 3 days, will require longer ICU stay after operation, especially with the associated issues related to the newborn group.
We have been operating TGA with VSD usually after 3 weeks of age and sometimes at 2 months of age depending on the clinical features of failure and feeding-related issues. This decision has always been a challenge so that the neonate will not land up in an emergency and on the ventilator. For this reason, taking up a TGA with VSD on ventilator has always been a risk factor for lung infections and associated prolonged ventilation and ICU stay. However, if carefully planned and executed, we have found that VSD with TGA after 1 month of age is an easily reproducible operation.
In small babies with VSD and TGA, the VSD closure has always been a challenge. We have found that using 7/0 Prolene suture for careful and delicate suturing and a pericardial patch for the VSD closure causes minimum rhythm disturbances. In fact, in our experience we had no incidence of heart block in all these babies with VSD with TGA.
In the early experience, using surgical glue for hemostasis in the aorta was initially encouraging as far as the bleeding management was concerned. Eventually and quickly, we noticed that the glue could be a risk factor for constriction of the coronary arteries and unexplained and sudden onset LV dysfunction in the later postoperative period in the first week. We feel that this could be the cause of death in the initial experience in some babies who had an otherwise good anastomosis and good LV function intraoperatively. For this reason, we stopped using surgical glue for the past 5 years and used only thrombin gel foam locally for hemostasis.
As far as the left diaphragm palsy is concerned, we noticed that using very low cautery at 10 during removal of the thymus and dissection of the branch PAs has been helpful in prevention of this complication. In addition, we have stopped putting stay sutures on the pericardium on the left side keeping the pull of the left phrenic nerve in mind. Furthermore, myocardial protection with cold saline only on the myocardium and not going onto the phrenic nerve area has been helpful.
For myocardial protection after aortic cross clamp and delivery of cardioplegia for cardiac asystole, shifting to Del Nido cardioplegia from the previous solution for the past 5 years has tremendously changed the outcomes; this manifested as improved LV function and less incidence of arrhythmia.
Right ventricular outflow tract sinuses have always been reconstructed with separate glutaraldehyde-treated pericardial patches. Earlier, the neo-PA reconstruction was done without augmenting additional pericardial hood anteriorly. However, after noticing a few cases of neo-PA restenosis, we modified the technique of PA reconstruction with incorporation of a generous anterior pericardial hood. This modification has helped us to prevent PA restenosis.
Using the aortic punch to make a button hole in the neoaorta during coronary implantation has helped us to tackle the mismatch problem of the neoaorta to the native aorta.
Perfusion-Related Issues
Maintenance of high hematocrit during CPB has definitely caused improved outcomes. This high hematocrit is important both during cooling and also after rewarming before coming off CPB. The use of hemofiltration continuously during CPB has been adequate. We have never used modified ultrafiltration.
Technical advances in surgical procedures with CPB have been possible due to minimization of the bypass circuits resulting in minimal priming volumes, decreased hemodilution on CPB to achieve higher hematocrit, and fewer blood product transfusions. 17
Peritoneal Dialysis After Complex Neonatal Cardiac Surgery
Neonates and small-weight babies after complex cardiac surgery are prone to developing renal dysfunction. Many a time, the inflammatory response to a long CBP time will manifest as ascitic fluid in the immediate postoperative period. This fluid has high content of cytokines. Drainage of this fluid by an indwelling peritoneal dialysis catheter helps tremendously to improve the hemodynamics and reduce lactate levels.
In all neonates and small babies, we always put a silicone peritoneal dialysis catheter (Tenckoff) intraoperatively after giving protamine and platelets into the abdomen from the suprahepatic area. This is tunneled subcutaneously from the skin and brought into the subxiphoid area and inserted after a purse string of 6/0 Prolene in the peritoneum above the liver. The catheter is carefully negotiated into the abdominal cavity. This will help in the postoperative period to drain the cytokine-rich ascitic fluid and help us to do a few cycles of peritoneal dialysis in case lactates are high initially. This procedure has helped us immensely in the postoperative management of these sick babies and prevented us to put a stiff peritoneal dialysis catheter percutaneously into the abdomen (which is traumatic to the intestines). This silicone peritoneal dialysis catheter is removed after extubation if the hemodynamics and urine output are good. This technique of insertion of the silicone peritoneal dialysis catheter was published by the author earlier. 18
If neonates develop obvious renal dysfunction, early intervention and institution of peritoneal dialysis is a safe and effective method to manage the problem. 19
Neurological Issues After Complex Cardiac Surgery
Neonates and small-weight babies after complex cardiac surgery, which involves deep hypothermia and circulatory arrest, are prone to neurological injury.20, 21, 22 To prevent this, we have adopted to use selective cerebral perfusion during arch repair in neonates and infants, and our outcomes have been published without neurological injury or seizure activity in these babies. 15
Neurological Evaluation After Arch Repair in Our Unit
All neonates and small infants had a preoperative neurosonogram from the anterior fontanelle whenever feasible. All patients had normal neurological clinical examination. There was no seizure activity in the immediate and late postoperative period. The bedside and predischarge neurosonogram was normal in all patients.
Feeding Difficulties in Neonates Following Cardiac Surgery
Complex cardiac surgery many a time is associated with prolonged ventilation and gradual weaning after extubation on noninvasive ventilation. The babies lose weight during recovery and it is very important to manage the feeding issues during this period so that the morbidity associated with the operation can be reduced. 23 In our own experience in our unit, we have evolved a protocol of institution of nasogastric feeding by the Ryles tube. However, we have always supplemented enteral feeds with intravenous amino acids and dextrose and avoided lipids.
Infection-Related Problems
The most challenging factor in managing the neonates after complex cardiac surgery has been the control of infection. Postoperative prolonged ventilation due to lung-related infection has been the main reason for prolonged ICU stay in our experience. Many a time, the infection is related to the referral unit from where the baby has been referred. Even though the C-reactive protein and the white blood cell count and the platelet count are normal in these babies on admission, they always have associated risk factors that make them susceptible to develop major infections causing significant morbidity. This was published by a multivariable risk estimation model and analysis involving the STS Congenital Heart Surgery Database. 24
In recent years, better antibiotic stewardship, better monitoring of blood cultures and endotracheal tube cultures, taking notice of the decrease in the platelet counts, and relating all these factors to the clinical behavior of the baby have improved the outcomes related to the infection-associated morbidity. In a developing country like us with resource limitations, improvements in infection-control practices have contributed significantly to reduce the morbidity and mortality associated with infection. 25
Summary
To conclude, neonatal cardiac surgery can be performed with acceptable mortality and morbidity. Even though there are many issues in the postoperative period that contribute to morbidity and prolonged ICU stay, with a dedicated team effort it is possible to manage the complications associated in this setting and achieve good outcome ultimately.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.