
Abstract
Epidemiological studies have shown that acute coronary events, heart failure, atrial fibrillation with fast ventricular rate and brain stroke events have increased prevalence in winter season. Infections have a pivotal role in triggering such events. Vaccination against influenza and pneumococcus has been documented to prevent such events in large epidemiological studies. Majority of the deaths during Corona virus-19 (COVID-19) pandemic were related to cardiovascular event apart from serious lung condition. Vaccination has been proven to reduce risk of recurrent hospitalizations and death especially in sick and frail patients with heart failure, chronic obstructive lung diseases, renal failure and acute coronary syndromes. It becomes more relevant in countries like India where patient has to pay huge amounts for hospitalization from the pocket. On the other hand, it reduces unnecessary strain on the healthcare manpower and resources. Practice of vaccination in addition to guidelines based pharmacological, device or surgical therapy, is to help both the patients and physicians.
Infection and inflammation trigger acute coronary syndrome, cause brain stroke, atrial fibrillation, and acute heart failure or decompensation of congestive cardiac failure. In the UK Biobank Study, 21.4% of patients with infections requiring hospital-based treatments had major cardiac events defined as acute myocardial infarction (AMI), cardiac death, and fatal or non-fatal stroke. 1 Another study evaluating Hospital Episode Statistics Admitted Patient Care data in England from Sept 1, 2008 to Aug 31, 2018 found that people with high cardiac risk (measured as QRISK score of 10% or more) were at high risk of acute cardiovascular events following a respiratory infection. 2
Viral Infections and Cardiovascular Disease
Viral infections have been found to increase the risk of acute cardiovascular events. On the flip side of this, patients with cardiovascular disease have an increased risk of viral and respiratory infections. 3 Coronaviruses, influenza, dengue and human immunodeficiency virus (HIV) have all been implicated in having adverse effects on the human cardiac and vascular systems.
The first coronavirus epidemic, severe acute respiratory syndrome coronavirus 1 and 2 (SARS-CoV-1 and 2), was reported from 2002 to 2004 and was caused by a single-stranded, positive-sense RNA virus. Histopathological samples from post-mortem examination revealed fibrinoid necrosis and infiltration of monocytes, lymphocytes, and plasma cells into the vessel walls of the heart, lung, liver, kidney, and adrenal glands. Spike proteins from the viral envelope attach to the angiotensin-converting enzyme-2 (ACE-2) receptor of the host cell to gain entry. This leads to ACE-2 downregulation, which increases angiotensin II, which in turn causes vasoconstriction, inflammation, and fibrosis. Vascular smooth muscle cells and the endothelium have ACE-2 receptors in abundance. 4
The Middle East Respiratory Syndrome-Related Coronavirus 5 (MERS-CoV) related epidemic was reported in 2012. It had fatality rate of approximately 34.4%. It primarily causes flu-like symptoms but also leads to acute myocarditis, heart failure, acute respiratory distress syndrome (ARDS), and multiorgan failure.
The coronavirus pandemic of 2019 (COVID-19) witnessed an increased incidence of cardiovascular issues. It is caused by SARS-COV-2 which belongs to the same family as SARS-COV and MERS-COV. Apart from severe respiratory illness, COVID-19 caused significant cardiovascular conditions like acute coronary syndrome, myocarditis, heart failure, stroke, thromboembolic events, arrhythmias, and sudden cardiac death. 6
Influenza epidemics in the past have also shown a pattern of excess cardiovascular disease-related mortality. Epidemiological studies have shown that influenza is associated with increased incidence of acute coronary syndrome, heart failure and stroke. 7 In a study involving US veterans between 2012 and 2014, it was observed that in patients with proven influenza, risk of acute cardiac injury within 30 days was 25%, the majority of which had it within the first three days of diagnosis. Of these, approximately 50% had AMI. 8 Influenza virus exerts its effect through neuraminidase which leads to ACE-2 downregulation, similar to that seen in SARS-CoV-1 and 2.
Acute myocarditis, heart failure, arrhythmias, pulmonary edema, brain stroke and tricuspid valve problems have been reported in patients suffering from dengue virus infection. 9
Patients infected with HIV have an increased risk of AMI, peripheral arterial disease, myocarditis, left ventricular dysfunction and pericardial effusion. 10
Respiratory Infection and Cardiovascular Disease
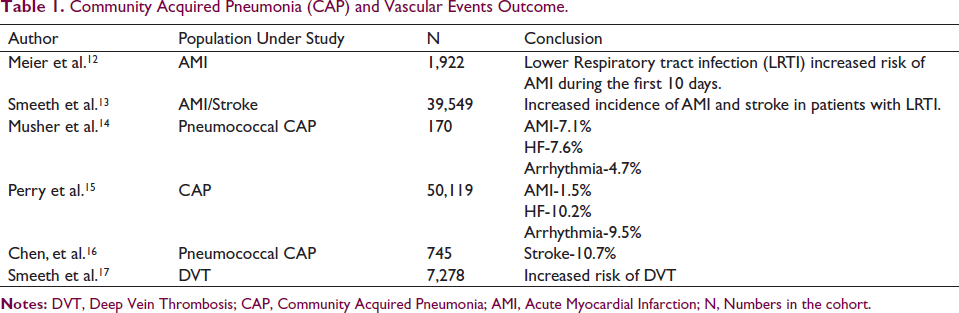
In a study by Zhao et al., in elderly patients with stable coronary artery disease (CAD), acute lower respiratory tract infection was an independent risk factor for CVD and all-cause mortality within 90 days of infection. 11 Multiple epidemiological studies have shown that pneumonia is associated with increased incidence of AMI, stroke, heart failure, atrial fibrillation and deep vein thrombosis. These have been summarized in Table 1.
Community Acquired Pneumonia (CAP) and Vascular Events Outcome.
Vaccination and the Prevention of CVD
Influenza
As early as in 1932, Selwyn Collins, a statistician from the United States Public Health Department, reported excess deaths from influenza epidemics linked to cardiovascular involvement. 7 Acute coronary syndromes and strokes have seasonal variation with a peak in winter months. In a similar vein, the peak in influenza infections has been found to be followed after two weeks by an increase in ACS and stroke in the population. 18 It has been estimated that influenza may be responsible for more than 90,000 deaths per year in the United States. 19
Evidence that Influenza Vaccination Prevents Cardiovascular Events
A study published by Naghavi et al., in 2000, found that influenza vaccination was associated with 67% reduction in CV events in the next influenza season in patients suffering from CVD. Major studies are summarized in Table 2.
Summary of Studies of Influenza Vaccination and CVD Events (Secondary Prevention).
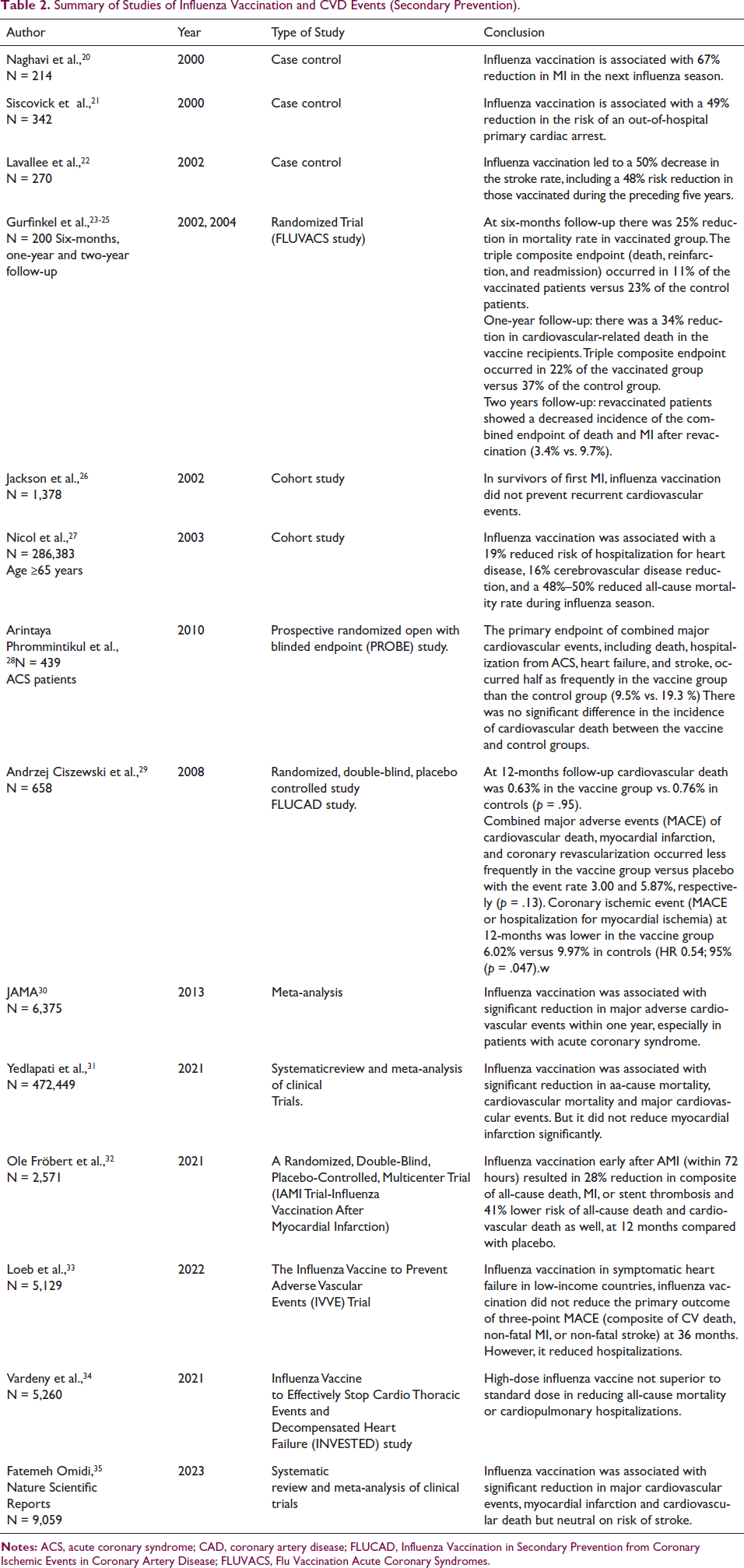
Influenza infection is associated with increased secretion of prothrombotic, proinflammatory cytokines which trigger ACS, heart failure, arrhythmias and stroke. Experimental evidence suggests that influenza infection is associated with increased platelet aggregation and derangement in coagulation factors leading to increased thrombogenicity. Mohammad Madjid et al. actually recommended to “Update cardiology practice guidelines to include flu shots” in their article in 2004. 36
Influenza Vaccine Guidelines
2023 AHA/ACC/ACCP/ASPC/NLA/PCNA Guideline for the Management of Patients with Chronic Coronary Disease (AHA - American Heart Association; ACC - American College of Cardiology; ACCP - American College of Chest Physicians; ASPC - American Society for Preventive Cardiology; NLA -National Lipid Association; PCNA - Preventive Cardiovascular Nurses Association) 37
Class IA: Patients with chronic CAD, an annual influenza vaccination is recommended to reduce cardiovascular morbidity, cardiovascular death, and all-cause death.
2021 Influenza Vaccination for the Prevention of Cardiovascular Disease in the Americas: Consensus document of the Inter-American Society of Cardiology and the Word Heart Federation 38
This consensus document evaluated causal role of influenza virus in CVD and concluded following observations:
There is definite evidence that influenza-like illnesses are associated with increased CV events of AMI, stroke, heart failure hospitalizations, AF, and CV death. The pathophysiological mechanism to explain it is clear. There is no sufficient evidence to link influenza-like illnesses with the risk of thromboembolism. Influenza vaccine in CAD is associated with reduced CV events (Class IA). The consensus recommends annual influenza vaccination in all patients with recent ACS (less than one-year duration). It also recommends annual influenza vaccination in chronic CAD patients with or without revascularization (Class IIa–b). In patients over 65 years of age, influenza vaccination is associated with reduced CV events even in the absence of established CVD, diabetes or other comorbidities (Class IA). The consensus recommends annual influenza vaccination in all adults 65 years of age or older even in the absence of CVD or risk factors. In patients with heart failure, annual influenza vaccination is associated with reduced HF hospitalizations and all-cause mortality (Class IIa–B). The consensus recommends annual influenza vaccination in all adults with HF (Class IIa–B). In patients with hypertension or diabetes, annual influenza vaccination may be associated with reduced CV events (Class IIb–C) (For Class of recommendations I, IIa, IIb and level of evidence A, B, C, please refer to society guidelines).
2023 European Society of Cardiology (ESC) Guidelines for the Management of Acute Coronary Syndromes 39
Influenza vaccination is recommended for all ACS patients (Class I recommendation, level of evidence A). The vaccine should preferably be administered during index hospitalization for ACS during influenza season if not immunized before. Administration of influenza vaccine early after ACS or in high-risk CAD patients, results in lower risk of all-cause mortality and CV death at 12 months.
The U. S. Centre for Disease Control and Prevention (CDC) 40
The CDC recommends influenza vaccination for:
Everyone six months or older. All patients with chronic illnesses—heart disease, asthma and other chronic lung conditions, stroke, chronic kidney disease, diabetes, chronic liver disease, cancers, and morbid obesity (body mass index [BMI] ≥ 40). Immunocompromised patients, patients with HIV infection. Pregnant females during influenza season. Health care providers—doctors, nurses, those who take care of sick patients, elderly, immunocompromised people, and children.
The CDC recommends flu shot in September–October every year for most of the patients.
Cardiovascular Safety and Drug Interactions of the Influenza Vaccine
In India, the commonly available influenza vaccine is an inactivated, tetravalent vaccine (four strains of influenza virus) containing a total of 60 micrograms of hemagglutinin in 0.5 ml suspension (Influvac tetra, Abbott). It contains a very negligible amount of egg albumin. Current evidence suggests that it can be given to most people, including those with egg allergies. It may be avoided in patients with prior anaphylaxis. There is no documented interaction with any cardiovascular drug including aspirin, antiplatelets, anticoagulants, anti-hypertensives, or other classes of cardiac drugs. It can be used in patients with thrombocytopenia.
In children, the combination of aspirin and Live Attenuated Influenza Vaccine (Influvac is inactivated) can cause Reye’s syndrome. Live attenuated influenza vaccine is not recommended in the elderly and is not cardio-protective.
High Versus Standard Dose Influenza Vaccines
Standard dose influenza vaccines (e.g., Influvac Tetra, Abbott Biologicals B.V., The Netherlands) have 15 micrograms of hemagglutinin per strain. High-dose vaccines (e.g., Fluzone High-Dose, Sanofi Pasteur, PA, USA) have 60 micrograms of hemagglutinin per strain.
Retrospective observations showed that the high dose was 22% more effective in prevention of influenza infection and hospital admissions. The Food and Drugs Administration (FDA), USA, has approved high-dose influenza vaccine for patients 65 years or older. 41
The Pneumococcal Pneumonia and Pneumococcal Vaccine
Community-acquired pneumonia (CAP) is a leading cause of death, especially in the elderly. Streptococcus pneumoniae or Pneumococcus are the most important pathogens associated with serious CAP. Up to 30% of CAP patients die because of cardiac complications like AMI, heart failure or arrhythmia. 42
In a meta-analysis published by Marra et al., 43 involving 716,108 participants, 23-valent polysaccharide pneumococcal vaccination (PPV23) was associated with reduced risk of any cardiovascular event, all-cause mortality and acute MI, especially in those 65 years or older. There was no notable effect on cerebrovascular disease. In another meta-analysis by Vikash Jaiswal et al. 44 including 347,444 patients, pneumococcal vaccination resulted in 24% reduction in all-cause mortality and 27% reduction in acute MI, but no difference in CV mortality and stroke as compared to unvaccinated individuals. In a pooled analysis of 163,756 patients with cardiovascular disease or at very high CVD risk, Miguel Marques Antunes et al. 45 found that this vaccination was associated with a 22% reduction in all-cause mortality. In the Cardiovascular Health Study (CHS), 46 it was associated with significant reduction in all-cause mortality, primarily cardiovascular mortality and heart failure in octogenarians.
Guidelines Recommendations for Pneumococcal Vaccine
ESC Guidelines on Heart Failure, 2021 47
Pneumococcal and Influenza vaccinations should be considered to prevent heart failure hospitalizations (Class IIa, level of evidence B).
Combined Influenza and Pneumococcal Vaccinations
Influenza and pneumococcal vaccines are routinely recommended prophylactically in adults 65 years of age or older. There is evidence that co-administration (at different sites) of influenza and pneumococcal vaccines is safe and synergistic in immune response. 48
Influenza and Pneumococcal Vaccination in Patients Receiving Antiplatelets and Oral Anticoagulants
Patients on aspirin, other antiplatelets, and oral anticoagulants can safely receive influenza and pneumococcal vaccines. There is no need to discontinue these medications. Also, checking prothrombin time prior to vaccination is not recommended. It is advisable to press the injection site for a longer period to prevent hematoma formation.
As mentioned previously in this article, Reye’s syndrome is a potential complication of aspirin and live attenuated influenza vaccine in children. Live attenuated influenza vaccine is not used in adults as it is not cardio-protective.
COVID-19 Vaccination for CVD Prevention
Acute coronary syndrome, deep vein thrombosis and pulmonary embolism are known complications of SARS-COVID-19 infection. COVID-19 vaccination has been shown to reduce chances of ACS, heart failure, cerebrovascular events and mortality in pre-existing CVD patients. 49 However, data is limited at the moment.
Combined Influenza, Pneumococcal and COVID-19 Vaccination as a Strategy to Prevent Cardiovascular Events
Theoretically, it looks scientifically attractive, but data on added benefits of COVID-19 vaccination over and above influenza and pneumococcal vaccination are lacking.
Herpes Zoster Vaccination in Prevention of CVD
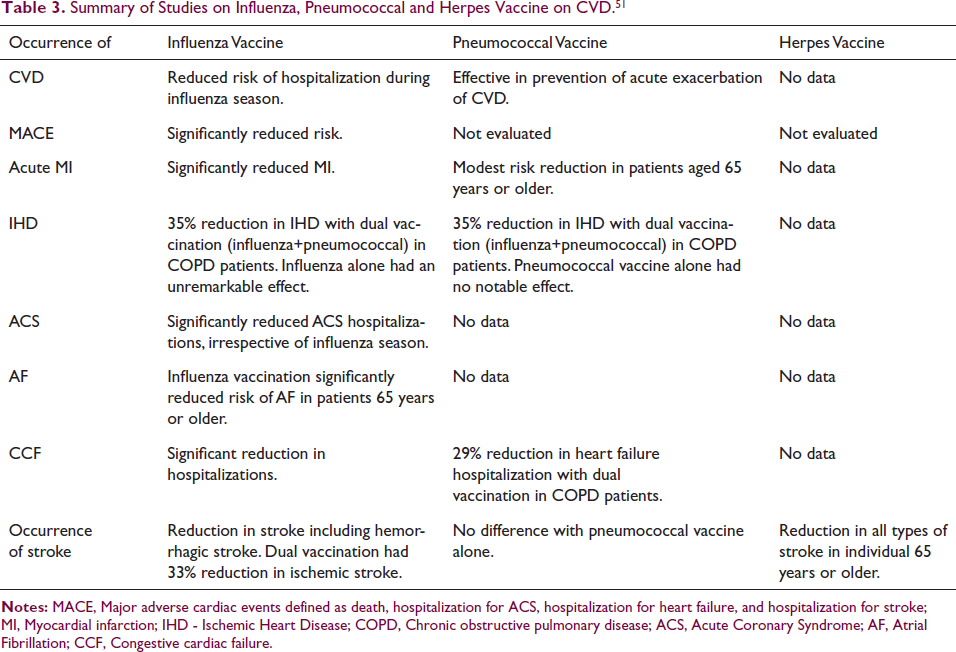
In a study by Ganapathi I. Parameswaran et al. 50 in 2,165,584 patients, Herpes zoster infection was associated with an increased risk of MI within 30 days post-infection in adults 50 years or older. It identified maleness, age ≥50 years, prior MI, CVD, renal disease, or HIV as important risk factors for developing MI post-infection. Having Herpes zoster (shingles) vaccine significantly reduced the risk of MI in this study. Table 3 summarizes important conclusions.
Summary of Studies on Influenza, Pneumococcal and Herpes Vaccine on CVD. 51
Immunization Schedule
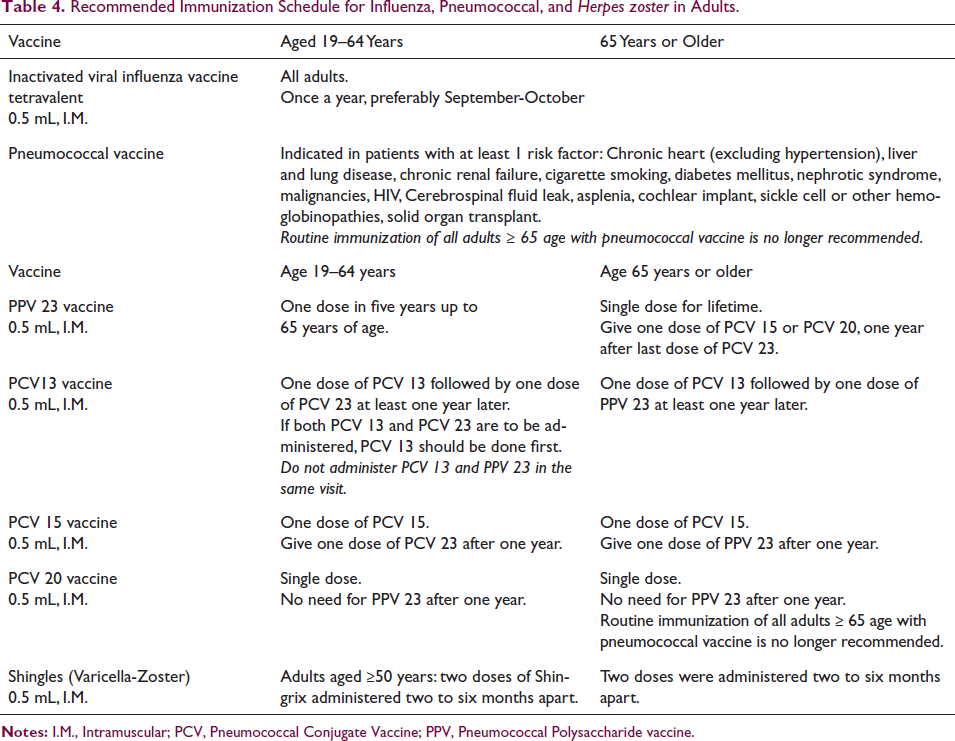
Immunization schedule, as suggested by CDC, is outlined in Table 4.
Recommended Immunization Schedule for Influenza, Pneumococcal, and Herpes zoster in Adults.
Influenza Vaccine as Compared to Other Preventive Strategies
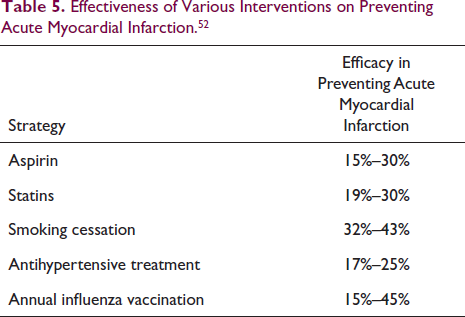
Influenza vaccination has a significant impact on preventing cardiovascular events and it compares well with other preventive strategies as shown in Table 5.
Effectiveness of Various Interventions on Preventing Acute Myocardial Infarction. 52
Conclusion
Infections play an important role in triggering acute coronary events, heart failure, AF and stroke. Annual influenza vaccination has resulted in reduction of all-cause mortality, and major adverse cardiovascular events in CAD patients. The preventive benefit of influenza vaccination is in the tune of 15%–45% which is as good as aspirin or statins. The sudden spurt in ACS, heart failure, stroke and AF admissions in winter season is not without any reason. Combined pneumococcal and influenza vaccination in COPD patients has remarkable synergistic effect in preventing hospitalizations. Considering the low cost with potential preventive benefits, influenza vaccination is strongly recommended in low and middle-income countries.
Footnotes
Acknowledgment
I sincerely thank Ms Shruti Sinha for proof-reading and editing the manuscript.
Patient Consent
Not applicable.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
Not applicable.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.