
Abstract
Transcatheter aortic valve replacement (TAVR) has become the mainstream option for patients with symptomatic severe aortic valve stenosis and is preferably performed by the transfemoral route. However, a subset of patients requires alternative access with comorbidities associated with femoral access routes, and alternative access such as transapical, transaxillary, transcarotid, subclavian, and transcaval can be considered. However, access options are further limited by the presence of severe comorbidities. This case reports TAVR performed through a transfemoral approach in a patient with previous aorto bi-iliac bypass graft surgery.
Case Report
A 76-year-old elderly man with a history of aorto-iliac occlusive disease 9 years back for which aorto bi-iliac bypass graft surgery using a dacron graft was done now presented with heart failure. Echocardiography and contrast-enhanced computed tomography (CT) revealed a severe calcific aortic valve stenosis (mean gradient 45 mmHg, peak gradient of 65 mmHg, AVA [aortic valve area] 0.8 cm2) with normal left ventricular function. Relevant comorbidities included morbid obesity. The patient had a high perioperative risk profile (STS PROM score 10.2%; EuroSCORE II 13.8%).
Therapy Decision-making
Due to our patient’s medical and surgical history with recurrent heart failure, and high risk for surgical AVR, computed tomography (CT) scanning was performed for preoperative planning of transcatheter aortic valve replacement (TAVR) procedure.
Preoperative Planning of the Procedure
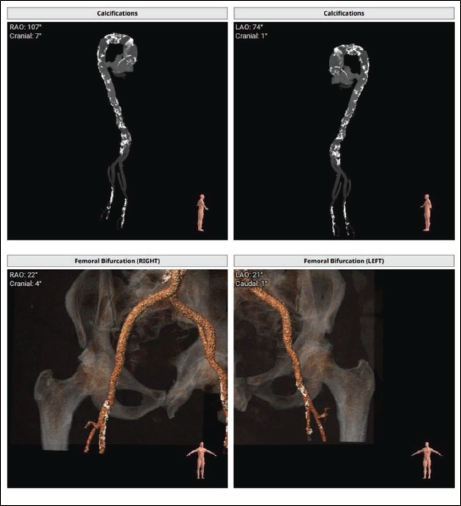
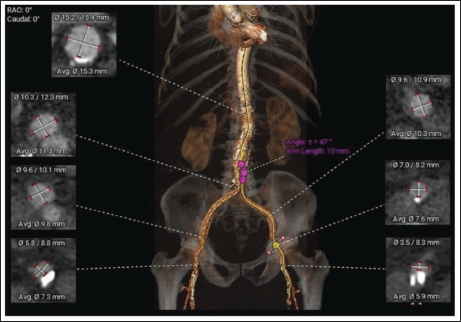
The structural heart software (3 Mensio by Pie Medical Imaging) was used for preoperative three-dimensional CT reconstruction and measurements. Multislice computed tomography (MSCT) showed severe calcification of abdominal aorta and femoral arteries (Figure 1), with occluded distal abdominal aorta and patent aorto bi-iliac bypass grafts. The diameters of the left and right femoral arteries were 7.3 and 5.9 mm, respectively (Figure 2). The right femoral artery was considered appropriate for access. In view of severe calcification, it was planned to proceed with femoral artery cutdown.
3-dimensional Reconstruction of the Aorta and Left and Right Femoral Arteries Showing Severe Calcification.
Minimum, Maximum, and Average Diameters.
Procedure
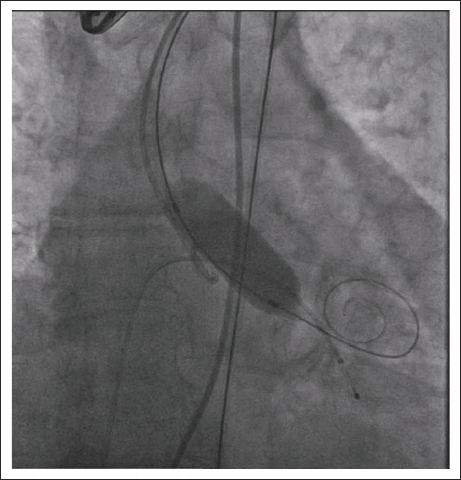
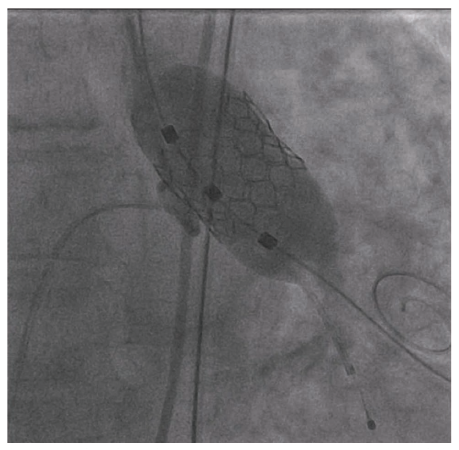
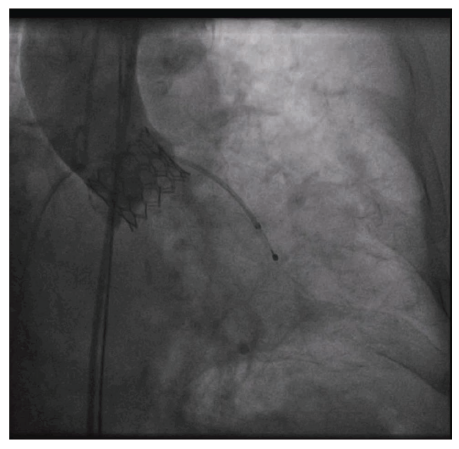
The right common femoral artery was punctured after a surgical cutdown, and it was dilated with a 12Fr sheath and a 14Fr Python sheath. After predilating, the valve with a 16 × 40 mm Mammoth balloon (Figure 3), a 23 × 30 mm Navigator delivery system with 23-mm MERIL Myval mounted over it was positioned across the valve and deployed under rapid pacing at 180 bpm (Figures 4 and 5). The delivery system was removed, the pigtail was inserted into LV, and the measured transvalvular gradient was less than 10 mmHg (Figure 6). The pigtail angiogram of the aortic root showed no aortic regurgitation (AR) (Figure 7). The large-bore access site was closed surgically attained hemostasis, with no complications. Post-procedure echocardiography showed a well-functioning valve with a mean gradient of 9 mmHg, with no paravalvular leak, and he was discharged 3 days later.
Predilatation of the Valve with 16 × 40 mm Mammoth Balloon.
23-mm MERIL Myval Positioned Across the Aortic Valve.
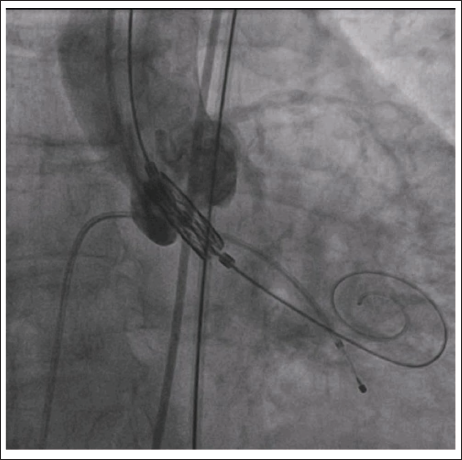
23-mm MERIL Myval Positioned Across the Aortic Valve and Deployed Under Rapid Pacing at 180 bpm.
Pressure Tracing Showing a Drop of Peak-to-Peak Gradient From 49 mmHg to Less Than 10 mmHg.

Aortic Root Angiogram Showing No Paravalvular Leak or Aortic Regurgitation.
Discussion
The selection of the TAVR valve and the approach is dependent of the size of the annulus, tortuosity and degree of calcification of the femoral and iliac arteries, and the calcification of the aortic arch. For patients in whom femoral access is not suitable, alternative approaches include the transapical, transaxillary, transcarotid, transcaval, subclavian, 1 and direct aortic 2 can be considered.
The relatively large diameter of the delivery catheter has been a major limitation of transarterial TAVR. First-generation systems used 22F–25F sheaths, and, in the absence of adequate screening, the prevalence of arterial dissection and perforation was relatively high. Newer low-profile systems are compatible with smaller sheaths (14F). The risk of vascular complications is reduced with the use of these lower-profile delivery systems. 3 The Navigator delivery system and Python sheath are the latest generation.
Our patient had the appropriate right femoral artery diameter but with severe calcification, in the femoral artery. Because of severe calcification, percutaneous closure may fail; hence, we decided to go with surgical cutdown. 4 His annular diameter was 22.2 mm. We used the new-generation 23-mm Meril MyVal transcatheter heart valve and the corresponding Navigator transfemoral delivery system. The procedure was performed successfully through the 14F sheath via the transfemoral approach, with no complications.
Conclusion
TAVR in patients with previous aorto bi-iliac bypass grafting can be considered through a transfemoral approach in the case of severe comorbidities or TAVR by alternative access.
Percutaneous closure of the access site is usually the preferred approach in TAVR. However, if there is severe calcification of the access site where percutaneous closure failure will be high, surgical cutdown is also an option, and a thorough preprocedural planning with CT is recommended.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author received no financial support for the research, authorship and/or publication of this article.
Ethical Approval
Institutional Ethics Committee approved prior to publication of this case report. A written informed consent was obtained from the patient.
Patient Approval
Patient consent was obtained for publication.