
Abstract
The major takeaway from 2022 Heart Failure guidelines (AHA/ACC/HFSA) was the 4-pillar concept of use of beta-blockers, RAAS inhibition (preferably ARNI), mineralocorticoid antagonist, and SGLT2 inhibitors (irrespective of diabetes) for HFrEF. The recommendations for HFpEF and HF mildly reduced EF are less robust. Some important heart failure trials are presented every year at ACC, AHA, ESC, and TCT, which can impact our practice even before the release of next guidelines. In this review, some select heart failure trials presented at these scientific meetings after January 2022 are briefly discussed with focus on the message they convey.
The major takeaway from 2022 Heart Failure guidelines (AHA/ACC/HFSA) was the 4-pillar concept of use of beta-blockers, RAAS inhibition (preferably ARNI), mineralocorticoid antagonist, and SGLT2 inhibitors (irrespective of diabetes) for HFrEF. 1 The other key messages were (a) for HFmrEF, SGLT2i have 2a recommendation; while rest of the 3 are considered 2b recommendation, (b) For HFpEF, SGLT2i are 2a recommended drugs and ARNI have 2b recommendation, (c) those labeled as HF-improved EF should be treated like HFrEF, (d) when EF is >40%, parameters of raised filling pressures have to be looked into, (e) recommendations for associated iron-deficiency states, anemia, hypertension, sleep disorders, type-2 diabetes, atrial fibrillation, coronary artery disease, and malignancy were refined, (f) recommendations for advanced HF as well as preventive strategies were also emphasized. The following is a selection of some important trials from the proceedings of ACC, AHA, ESC, and TCT since January, 2022, which would not have been considered at the time of the drafting of the above guidelines. 2
VALOR-HCM: [ACC-2022; Circulation 2023;147:850-63]
Mavacamten, a targeted cardiac myosin inhibitor, was tested in patients with severely symptomatic obstructive hypertrophic cardiomyopathy. The standard of therapies—alcohol septal ablation and surgical myectomy are effective to reduce gradient but are limited to a few centers needing skilled operators. In 19 centers in USA, 112 highly symptomatic patients waiting for septal reduction therapy (SRT) were randomized to the drug versus placebo. At 16 weeks only 18% remained eligible for septal reduction and showed gradient reduction, improved biomarkers, and functional score. It can be concluded that it is a good alternative or at least a stopgap to SRT. Mavacamten is available in a restricted manner, not recommended for use if LVEF is less than 50% and cannot be co-administrated with disopyramide, diltiazem, or verapamil.
SODIUM-HF: [ACC 2022; Lancet 2022;399:1391-1400]
Use of sodium 2300-2500 mg per day was compared to usual care in patients of heart failure over 12 months with respect to CV events. Both groups showed similar results and the trial was terminated early. There was modest improvement in quality of life and NYHA class in those on low sodium; but 6-minute walk test was not different in the 2 groups. In 2013 low-sodium was proven to protect the progression in heart failure. The 2022 AHA guidelines recommend to avoid excess sodium intake in stage C heart failure patients without the mention of any specific restriction.
METEORIC TRIAL: [ACC 2022]
Selective cardiac myosin activator Omecamtiv mecarbil, which showed positive benefit in HFrEF in Galactic -HF trial earlier was tested in multicentric study. After 20 weeks a cardiopulmonary test did not improve compared to pre-randomization tests. Overall safety was comparable to placebo. Recently FDA turned down the approval for this drug.
EMPULSE [ACC 2022; Eur Heart J 2022]
At 90 days in hospitalized patients of acute heart failure, Empagliflozin (vs Placebo) resulted in significant clinical benefits and improved loss of weight. These benefits were irrespective of diabetic status or the LVEF at recruitment. It has been proven in HFrEF and HFpEF in earlier trials.
PROMPT-HF: [ACC 2022]
In a single center in OPD practice the patients were randomized to a tailored electronic health record alerts recommending GDMT in patients of HFrEF or no alerts. This had a positive role in improving the GDMT and overall HF care.
DIAMOND TRIAL: [ACC 2022; Jam Coll Cardiol 2022;79:2203-2213]
Patiromer is a novel potassium binder that can lower the serum potassium levels. Patients of HFrEF are prone to develop hyperkalemia due to RAAS inhibitors or MRAs. This study included 1640 patients of HFrEF in whom Patiromer was given in a randomized fashion. Patiromer group had lesser incidence of hyperkalemia and lesser need to reduce MRA.
DELIVER study: [ESC 2022; Neng J Med 2022;387:1089-1098]*
Dapagliflozin is of proven benefit in HFrEF irrespective of diabetic status as well proven in DAPA-HF trial. DELIVER trial looks at Dapagliflozin in Heart Failure with mildly reduced and preserved ejection fraction. This was recently discussed in an earlier issue of this journal (volume 4, issues 1).
ADVOR: [ESC 2022; Circulation 2022;387:1185-1195]*
In a small study, addition of intravenous acetazolamide to loop diuretic therapy in patients in acute decompensation result in better decongestion, irrespective of baseline LVEF.
[*Both DELIVER and ADVOR trials are described in more details by Dr Mukharjee in another article in this issue.]
STRONG HF: [AHA 2022; Lancet 2022;400:1938-1952]
In hospitalized patients of acute decompensated heart failure, a systematic tailored rehabilitation if begun early and continued for 12 weeks resulted in much better physical well-being than usual care. Early ambulation and putting back on rehabilitation while coming out of acute decompensated heart failure is to be encouraged.
TRANSFORM HF: [AHA 2022; JAMA 2023;329:214-223]
In this randomized trial, in hospitalized patients of acute decompensated heart failure, the choice of loop diuretic did not make any difference in survival or readmission when either furosemide or torsemide was used. The initial expectation was that torsemide would fare better. The trial did not push down the age-old furosemides as a choice decongestant in acute heart failure.
IRONMAN [AHA 2022; Lancet 2022]
Unlike AFFIRM trial and contrary to recommendation II a of IV iron therapy for patients of chronic heart failure, intravenous ferric derisomaltose vs usual show only a nonsignificant trend towards lessened hospitalizations and CV deaths. No improvement in walking distance or quality of life were noted. The conduct and results of this trial were probably affected by prolonged COVID pandemic.
GUIDE-HF: [TCT 2022; J Am Coll Cardiol HF 2022;10:945-947]
Ambulatory sensor-Cardio MEMS HF system was randomized to patients in HF (NYHA II-IV), versus usual care. The group on the monitoring device did not show enhanced improvement in CV outcomes among stable outpatients. The 2022 guidelines gave 2b recommendation for such remote monitoring device to be used in select HF patients in NYHA class III with recent hospitalization or elevated BNP.
BMAD trial: [ACC 2023]
All 522 patients were given the µCOR—a wearable fluid sensor. But in one group thoracic fluid index was alerted to the clinician and in other group no alerts are sent. In those whose fluid alerts reached clinician resulted in better fluid management and lower risk for HF rehospitalizations. It is nonrandomized trial. Quality of life steadily improved in those who used this monitoring device. It is a silver lining after the disappointment with Cardio MEMS system in GUIDE-HF trial.
REVIVED-BCIS2 trial: [ACC 2023; Eur Heart J 2022;43:4775-4776]
It was designed to evaluate how percutaneous coronary intervention fares compared to optimal medical management in ischemic cardiomyopathy with extensive coronary artery disease. In this open label randomized trial of 700 subjects, multi-vessel PCI did not improve all-cause mortality or LV function; however, PCI did not do any harm as well. It is likely that scar burden at baseline predicts the LV recovery. Hunting for any hibernating myocardium and revascularization of that area did not work in ischemic cardiomyopathy.
BETTER-CARE HF [ACC 2023; J Am Coll Cardiol 2023;81:1303-1316]
This study had shown that among patients with HFrEF, OPD patients can be benefited if an electronic alert or message is sent to the cardiologist about prescription of a mineraloc-orticoid antagonist compared to usual care. These HER embedded tools are low cost and rapid and improve the prescription of MRAs. This trial opens up possible ways to overcome implementation barriers in HF treatment with well-proven drugs.
IMPLEMENT HF [ACC 2023; JACC March 2023]
In patients in HF, with LVEF < 45%, a physician-pharmacist team virtually gave once-a-day recommendation for optimizing GDMT to one group (n = 83) and the other group received usual care (n = 115). Effectiveness is measured by in-hospital change in optimization and safety outcomes. Such strategy was found to be a safe and effective intervention to optimize GDMT. Please read this along the lines of the results of PROMPT trial presented at ACC2022 and BETTER CARE trial mentioned above. A good prompting leads to accelerated implementation of guideline concordant HFrEF care.
The GWTG Registry: [ACC 2023; J Am Coll Cardiol 2023;11:21-223]
FDA approved vericiguat in 2021 following the Victoria trial. This registry in US has shown that approximately 4 in 10 patients met the criteria for use of vericiguat based on VICTORIA and 9 out of 10 by FDA criteria for administration of vericiguat. However, in contemporary Medicare hospitalized patients of heart failure with LVEF< 45 and used vericiguat faced higher rates of post discharge mortality and readmissions. The higher costs involved alerted the health administrators to keep check on use of vericiguat.
Conclusions
The management of heart failure is a fascinating field. With in pouring of clinical trials on a regular basis year after year our concepts get modified and the guidelines keep changing. We have to keep our eyes open to the new developments.
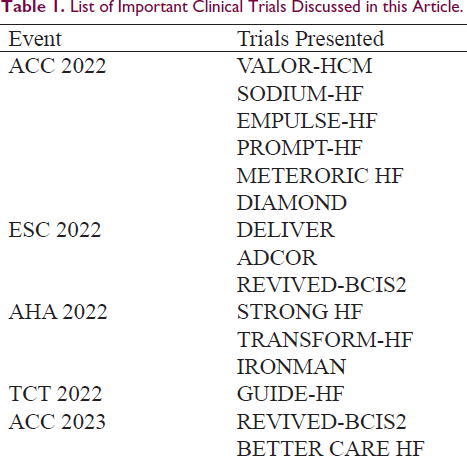
List of Important Clinical Trials Discussed in this Article.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval is not applicable as the content is not an original study. I only reviewed existing published literature.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Patient consent is not applicable as no data of an individual or a group was utilized for this manuscript.