
Abstract
Iatrogenic left main coronary artery (LMCA) dissection is a rare complication of percutaneous coronary intervention (PCI), it is mainly attributed to the catheter-based manipulation during engagement of Ostia or during the intervention. LMCA dissections are very dynamic ranging from a small, stable, and localized tear to extensive dissection obstructing coronary branches and cardiac arrest. Without prompt intervention, it often is a fatal complication. In this case series, we report three cases of LMCA dissection and their management with intravascular ultrasound-guided PCI.
Introduction
Iatrogenic left main coronary artery (LMCA) dissections are rare, with a reported incidence of <0.2%.1, 2 It is one of the most catastrophic complications of percutaneous coronary intervention (PCI), with potentially fatal outcomes. Iatrogenic LMCA dissections are characterized angiographically by a dynamic presentation, extending from a small, stable tear to a rapid, extending dissection with flow-limiting obstruction of coronary branches. 2 Symptoms also depend on the extent of the dissection flap and the luminal narrowing caused by it, ranging from an asymptomatic finding to complete hemodynamic collapse. To tackle this complication, urgent restoration of coronary flow is required; in places without prompt surgical backup, percutaneous management is the only option for management. Intravascular ultrasound (IVUS) has been extensively used in coronary intervention, and its role is imminent in the management of this complication as it guides us in identifying the true lumen and the dissection flap. To restore flow in LMCA, it is pivotal to wire the true lumen as soon as possible. 3 In this case series, we describe three cases with iatrogenic LMCA dissection and their management percutaneously with IVUS-guided drug-eluting stent (DES) implantation.
Case Series
Case 1
A 51-year-old male presented to us with complaints of angina and dyspnea on exertion (NYHA III) from the last 3 months. His vitals were stable, and his physical examination was normal. He was a current smoker with diabetes mellitus managed with oral medications; he had a previous history of stenting to the left anterior descending artery (LAD) 5 years back. His electrocardiogram (ECG) was consistent with old anterior wall myocardial infarction (MI) with Q-waves in precordial leads, and echocardiography revealed mild LV dysfunction and an ejection fraction of 40%. The patient’s coronary angiography (CAG) revealed significant in-stent restenosis of the LAD.
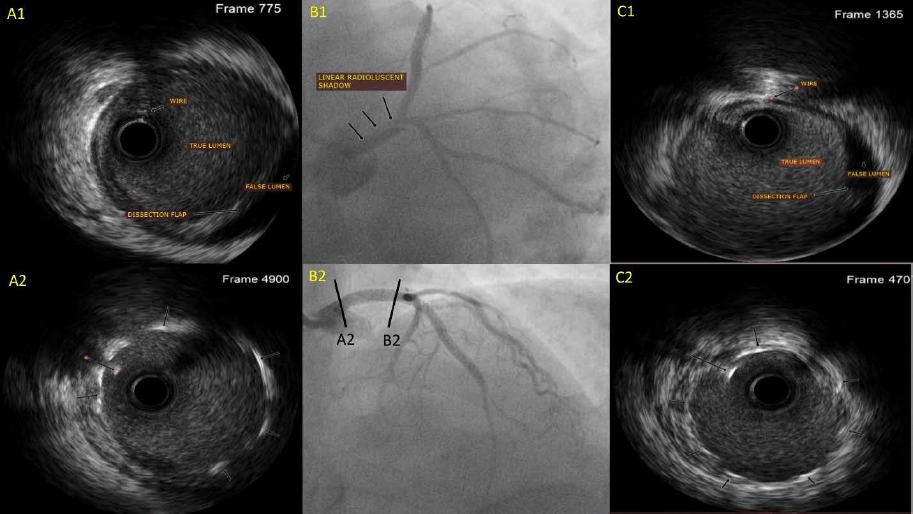
The patient was taken for ad hoc PCI, and a 7-Fench XB 3.5 (Cordis, USA) guiding catheter was advanced for engaging the LMCA Ostia. The ISR LAD lesion was dilated with a non-compliant balloon and stented using DES. After the withdrawal of the wire, the final cine-angiogram showed a large spiral type D dissection of the LMCA involving the LAD ostium (Figure 1, B1). 4 The patient immediately complained of chest pain with hemodynamic deterioration; the lesion was immediately re-wired using Fielder FC wire (Asahi INTEC, USA), IVUS was done using OptiCross (Boston Scientific, USA), which confirmed the wire in true lumen (TL) and showed a dissection flap with a false lumen in LMCA (Figure 1, A1, C1). The lesion was stented with a 3.5×28 mm DES from LMCA to LAD and post-dilated with a 4 mm non-compliant balloon, with satisfactory results (Figures 1, A2, B2, C2) and minimum lumen area (MLA) of 11.2 mm2. The patient was observed and discharged on day 2 without any further problems.
Case 2
A 52-year-old male presented to us with complaints of acute onset chest pain, radiating to the left arm for the last 4 hours. His blood pressure was 128/70 mmHg, and the rest of the physical examination was normal. He was a current smoker (15 packs per years) and was on treatment for chronic hypertension with adequate control. His ECG showed an ST-elevation in lead II, III, and aVF with reciprocal ST-depression in I and aVL. Qualitative troponin T was positive, and an echocardiogram showed hypokinesia of the inferior segment with normal valvular function and no evidence of any dissection flap in the aorta. Diagnosis of acute inferior wall MI was made, and the patient was shifted for PCI. His CAG showed terminal obtuse marginal 100% cut-off as the culprit lesion.
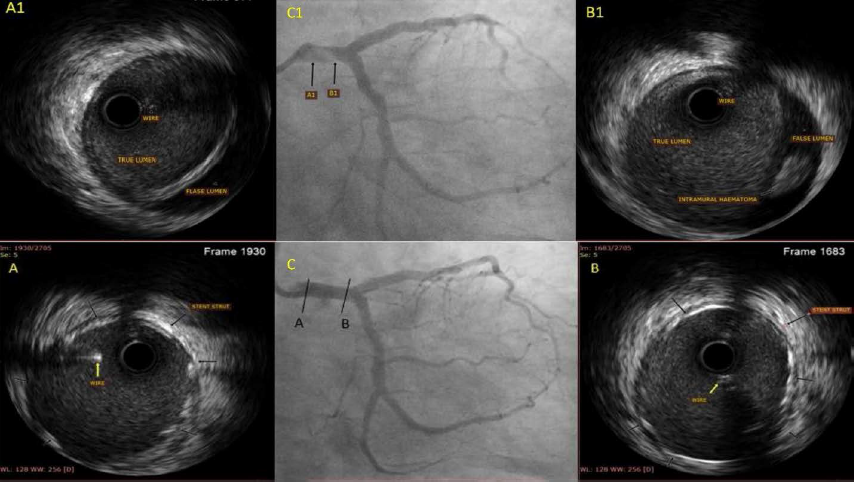
Using the right femoral artery, a 7-Fench XB 3.5 guide (Cordis, USA) LMCA was engaged, and successful DES implantation was done to the culprit’s vessel. After the guidewire was withdrawn for the final angiogram, the guiding catheter got disengaged and was manipulated for re-engaging LMCA with difficulty in the alignment of the guiding catheter as it was hugging the LMCA wall, final forceful cine-angiogram lead to the development of type D spiral dissection of limited to LMCA (Figure 2, C1). A BMW (Abbott Vascular, USA) was crossed immediately across the LMCA, and IVUS was done using an OptiCross catheter (Boston Scientific, USA), which confirmed the wire in the TL and showed a large dissection with an intramural hematoma in the false lumen (Figure 2, A1, B1). The dissection was sealed using a 4×23 mm DES from the LMCA to the LAD and post-dilated with a non-compliant balloon, with a satisfactory result (Figure 2, A, B, C) and an MLA of 14.2 mm2. The patient was observed and discharged on day 2 of the procedure.
Case 3
A 56-year-old male presented to us with a chief complaint of exertional angina and palpitations (NYHA II) from the past 6 months. His blood pressure was 110/72 mmHg, and the rest of the physical examination was normal. He had a history of smoking in the past and was on medication for diabetes mellitus and chronic hypertension with adequate control. His ECG was normal with no significant ST-T changes, and his chest skiagram did not show any signs of advanced obstructive lung disease. A stress treadmill test was performed, which showed significant ST depression during the recovery phase, and an echocardiogram showed a new regional wall motion abnormality in the anterior segments with an LV ejection fraction of 40%. The patient was planned for CAG, which revealed a tight lesion of the proximal LAD with eccentric calcium.
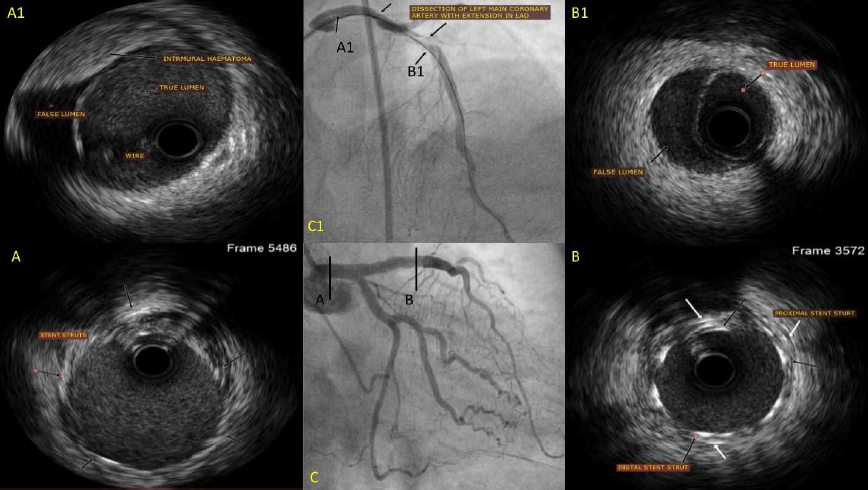
The patient was taken for ad hoc PCI using the right femoral artery. A 6-Fench XB 3.5 (Cordis, USA) was used to cannulate the LMCA, and a BMW wire (Abbott Vascular, USA) was passed across the lesion. Pre-dilatation with a compliant balloon was done, and during balloon withdrawal, the guiding catheter was pushed deep into the LAD, following which the patient developed an LMCA dissection of LMCA extending distally to LAD (Figure 3, C1), which was confirmed with IVUS using OptiCross catheter (Boston Scientific, USA) (Figure 3, A1). LMCA to LAD was stented with a DES of 3.5×48 mm, but following post-dilatation IVUS images confirmed a presence of intramural hematoma extending till distal LAD (Figure 3, B1) and compromising the lumen, for which another DES of 2.5×44 mm was implanted with satisfactory results (MLA of LMCA 13.8 mm2 and MLA of LAD 9.1 mm2) (Figures 3, A, B).
Discussion
Iatrogenic LMCA dissection during percutaneous intervention is a rare (<0.2%) but potentially catastrophic complication.1, 2 The iatrogenic injury usually results from either catheter/wire manipulation (Cases 1 and 3) or forceful injection of contrast medium (Case 2).2, 5 Due to the dynamic presentation of LMCA dissection, management also depends on the extent of dissection, ranging from an asymptomatic, small, limited tear to complete obstruction of the LMCA. Prompt intervention, such as percutaneous bail-out stenting or an urgent coronary artery bypass graft (CABG), is required, especially in patients with hemodynamic compromise and extension of dissection into the aorta. 3 Imaging in the form of IVUS 6 or optical coherence tomography (OCT) 7 plays a pivotal role in successful wiring, assessment of lesion nature, deciding length, and optimization of DES. Percutaneous management is feasible but often challenging due to the hemodynamic status of the patient and the challenge of wiring the TL, which carries an inherent risk of both extension of the dissection flap and intramural hematoma and can compromise the distal coronary blood flow and lead to further deterioration of the patient. 2 Both OCT and IVUS can be used to identify the TL, origin and extent of the dissection, and placement of the guidewire in the TL, 3 but IVUS scores better due to the lack of contrast injection for image acquisition and the limitation of aorto-ostial visualization as seen with OCT. 8
In all 3 cases, dissection was managed percutaneously with the aid of IVUS, which facilitated the procedure with prompt identification of the TL and prevention of further contrast injection to prevent extension of the dissection. In Case 3, it helped us identify the intramural hematoma extension leading to a significant narrowing of the distal LAD, which was otherwise missed in conventional angiographic views. Prevention of such complications should be the operator’s first choice and is easily achievable with gentle catheter manipulation, proper alignment of the guide catheter to prevent a contrast-induced tear of the LMCA, and anticipation of guide movement with the withdrawal of instruments from the coronary branches. The operator should be prompt and well versed in the treatment protocol of this dreaded complication of PCI. Wiring the dissection is the most important step using the double wire technique, 3 sepal wire technique, 9 or direct wiring helps save time for full restoration of distal blood flow.
Several lessons can be learned from this case series: first, it obliges us to remember that PCI is an invasive procedure with its inherent complications; second, guide manipulation should be done gently; third, the guide should be properly aligned with the LMCA during contrast injection; and fourth, in cases of dissection, IVUS plays a pivotal role in the management of this complication.
Conclusion
Although prevention is the best strategy for avoiding iatrogenic dissection of LMCA, it is not inevitable in PCI. In this case series, IVUS-guided bail-out stenting was performed in all the three cases with satisfactory results showing its feasibility and safety.
Learning objectives:
LMCA dissection is a rare complication of PCI but not unavoidable. Ensuring proper guide handling, alignment, and caution in instrumentation help in avoiding this catastrophic complication. IVUS plays an important role in understanding the underlying mechanism and extent of the dissection. With prompt intervention and image guidance, this complication can be managed effectively with percutaneous interventions.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.