
Abstract

Introduction
Learn continually. There’s always ‘one more thing’ to learn. —Steve Jobs
With our fast-paced work life, we often find ourselves hard-pressed for time for personal life, let alone find time to update ourselves. But then if we don’t stay up-to-date, we risk getting left behind. Cardiology is changing at a breath-taking pace. I hereby present 10 latest articles across the gamut of cardiology published between Jan 2022 and April 2022. In my limited capacity, I have made a few comments regarding the utility and impact of these articles on our practice. Hope these articles make for interesting reading!
Article 1a: Cardiac Implantable Electrical Device Therapy
Left Bundle Branch–Optimized Cardiac Resynchronization Therapy (LOT-CRT): Results From an International LBBAP Collaborative Study Group
Heart Rhythm. 2022, January 1; 19(1):P13-21.
Marek Jastrzębski, Paweł Moskal, Wim Huybrechts, Agnieszka Bednarek, Marek Rajzer, Pugazhendhi Vijayaraman.
Abstract
Background: Cardiac resynchronization therapy (CRT) based on the conventional biventricular pacing (BiV-CRT) technique sometimes results in broad QRS complex and suboptimal response.
Objective: We aimed to assess the feasibility and outcomes of CRT based on left bundle branch area pacing (LBBAP, in lieu of the right ventricular lead) combined with coronary venous left ventricular pacing in an international multicenter study.
Methods: LBBAP-optimized CRT (LOT-CRT) was attempted in nonconsecutive patients with CRT indications. Addition of the LBBA (or coronary venous) lead was at the discretion of the implanting physician, who was guided by suboptimal paced QRS complex, and/or on clinical grounds.
Results: LOT-CRT was successful in 91 of 112 patients (81%). The baseline characteristics were as follows: mean age 70 ± 11 years, female 22 (20%), left ventricular ejection fraction 28.7% ± 9.8%, left ventricular end-diastolic diameter 62 ± 9 mm, N-terminal pro–B-type natriuretic peptide level 5821 ± 8193 pg/mL, left bundle branch block 47 (42%), nonspecific intraventricular conduction delay 25 (22%), right ventricular pacing 26 (23%), and right bundle branch block 14 (12%). The procedure characteristics were as follows: mean fluoroscopy time 27.3 ± 22 min, LBBAP capture threshold 0.8 ± 0.5 V @0.5 ms, and R-wave amplitude 10 mV. LOT-CRT resulted in significantly greater narrowing of QRS complex from 182 ± 25 ms at baseline to 144 ± 22 ms (P < .0001) than did BiV-CRT (170 ± 30 ms; P < .0001) and LBBAP (162 ± 23 ms; P < .0001). At follow-up of ≥3 months, the ejection fraction improved to 37% ± 12%, left ventricular end-diastolic diameter decreased to 59 ± 9 mm, N-terminal pro–B-type natriuretic peptide level decreased to 2514 ± 3537 pg/mL, pacing parameters were stable, and clinical improvement was noted in 76% of patients (New York Heart Association class 2.9 vs 1.9).
Conclusion: LOT-CRT is feasible and safe and provides greater electrical resynchronization as compared with BiV-CRT and could be an alternative, especially when only suboptimal electrical resynchronization is obtained with BiV-CRT. Randomized controlled trials comparing LOT-CRT and BiV-CRT are needed.
Article 1b: Cardiac Implantable Electrical Device Therapy
Clinical Outcomes of Left Bundle Branch Area Pacing Compared to Right Ventricular Pacing: Results From the Geisinger-Rush Conduction System Pacing Registry
Heart Rhythm. 2022, January 1;19(1):P3-11.
Parikshit S. Sharma, Neil R. Patel, Venkatesh Ravi, Henry D. Huang, Faiz A. Subzposh, Pugazhendhi Vijayaraman.
Abstract
Background: Left bundle branch area pacing (LBBAP) has been shown to be a feasible option for patients requiring ventricular pacing.
Objective: The purpose of this study was to compare clinical outcomes between LBBAP and RV pacing (RVP) among patients undergoing pacemaker implantation.
Methods: This observational registry included patients who underwent pacemaker implantations with LBBAP or RVP for bradycardia indications between April 2018 and October 2020. The primary composite outcome included all-cause mortality, heart failure hospitalization (HFH), or upgrade to biventricular pacing. Secondary outcomes included the composite endpoint among patients with a prespecified burden of ventricular pacing and individual outcomes.
Results: A total of 703 patients met inclusion criteria (321 LBBAP and 382 RVP). QRS duration during LBBAP was similar to baseline (121 ± 23 ms vs 117 ± 30 ms; P = .302) and was narrower compared to RVP (121 ± 23 ms vs 156 ± 27 ms; P <.001). The primary composite outcome was significantly lower with LBBAP (10.0%) compared to RVP (23.3%) (hazard ratio [HR] 0.46; 95%T confidence interval [CI] 0.306-0.695; P <.001). Among patients with ventricular pacing burden >20%, LBBAP was associated with significant reduction in the primary outcome compared to RVP (8.4% vs 26.1%; HR 0.32; 95% CI 0.187-0.540; P <.001). LBBAP was also associated with significant reduction in mortality (7.8% vs 15%; HR 0.59; P = .03) and HFH (3.7% vs 10.5%; HR 0.38; P = .004).
Conclusion: LBBAP resulted in improved clinical outcomes compared to RVP. Higher burden of ventricular pacing (>20%) was the primary driver of these outcome differences.
Reviewer Comment: Strategies to achieve physiological pacing have been around ever since it was identified that RV pacing leads to deleterious effects including but not limited to LV dysfunction and increased heart failure hospitalizations. RV septal pacing and RVOT pacing sites have been explored and tried but haven’t achieved much success due to the difficulty in achieving a true RVOT pacing with traditional fluoroscopic positioning and a failure to narrow QRS in most cases. Conduction system pacing (CSP) is rapidly growing in popularity the world over; however, it still represents a small minority of implants. His bundle pacing (HBP) which was the first developed method of CSP has fast lost favor due to the problems of poor sensed R waves and high pacing thresholds leading to a more rapid battery depletion. Left bundle area pacing (LBBAP) has taken over as a promising alternative to HBP that bypasses the disadvantages of HBP. Data from the MOST trial showed that patients needing > 40% RV pacing had a greater than 2.5-fold increase in risk of heart failure hospitalization. Recent studies (Kiehl et al, Heart Rhythm, 2016;13:2272-2278) have shown that a RV pacing burden as low as 20% is associated with an increased risk of pacing-induced cardiomyopathy.
Sharma et al in a large observational study of clinical outcomes compare LBBAP with conventional RV pacing at a minimum 1-year follow-up. The results were very encouraging with good R wave amplitudes and comparable capture thresholds both at baseline and follow-up. The most encouraging was a significant reduction in the primary outcome, which was a composite of mortality, heart failure hospitalization, and need for BiV pacing with LBBAP in those needing >20% RV pacing.
Marek et al in a novel paper on left bundle branch-optimized cardiac resynchronization therapy (LOT-CRT) enrolled 112 patients in whom an LBBA pacing lead was employed at the discretion of the implanting physician to achieve better resynchronization in patients posted for BiV pacing. They reported a success rate of 81% with good R wave and comparable thresholds to conventional implant techniques. Notably, LOT-CRT resulted in significantly greater narrowing of the QRS complex than did BiV-CRT (P < .0001). At 3 months follow-up, there was a significant improvement in LVEF, reduction in LVEDD, and NT-proBNP levels with clinical improvement noted in 76% of patients undergoing LOT-CRT.
The results while truly encouraging should be interpreted with caution as observational studies are prone to selection bias. As LBBAP is at the threshold to becoming the preferred technique for bradycardia pacing, larger and long-term RCTs are needed to fully elucidate the benefits of this novel technique.
Article 2: Stable CAD
CT or Invasive Coronary Angiography in Stable Chest Pain
N Engl J Med. 2022, April 28;386:1591-1602. doi: 10.1056/NEJMoa2200963.
The DISCHARGE Trial Group
Abstract
Background: In the diagnosis of obstructive coronary artery disease (CAD), computed tomography (CT) is an accurate, noninvasive alternative to invasive coronary angiography (ICA). However, the comparative effectiveness of CT and ICA in the management of CAD to reduce the frequency of major adverse cardiovascular events is uncertain.
Methods: We conducted a pragmatic, randomized trial comparing CT with ICA as initial diagnostic imaging strategies for guiding the treatment of patients with stable chest pain who had an intermediate pretest probability of obstructive CAD and were referred for ICA at one of 26 European centers. The primary outcome was major adverse cardiovascular events (cardiovascular death, nonfatal myocardial infarction, or nonfatal stroke) over 3.5 years. Key secondary outcomes were procedure-related complications and angina pectoris.
Results: Among 3,561 patients (56.2% of whom were women), follow-up was complete for 3,523 (98.9%). Major adverse cardiovascular events occurred in 38 of 1,808 patients (2.1%) in the CT group and in 52 of 1,753 (3.0%) in the ICA group (hazard ratio, 0.70; 95% confidence interval [CI], 0.46 to 1.07; P = .10). Major procedure-related complications occurred in 9 patients (0.5%) in the CT group and in 33 (1.9%) in the ICA group (hazard ratio, 0.26; 95% CI, 0.13 to 0.55). Angina during the final 4 weeks of follow-up was reported in 8.8% of the patients in the CT group and in 7.5% of those in the ICA group (odds ratio, 1.17; 95% CI, 0.92 to 1.48).
Conclusions: Among patients referred for ICA because of stable chest pain and intermediate pretest probability of CAD, the risk of major adverse cardiovascular events was similar in the CT group and the ICA group. The frequency of major procedure-related complications was lower with an initial CT strategy.
Reviewer Comments: Chest pain is one of the commonest presenting problems encountered by any cardiologist. Making a correct interpretation of the cause of chest pain is a crucial diagnostic skill that is essential for proper management. In the preinterventional era, medical management was central to the management of patients presenting with stable angina. Currently, patients with stable angina often undergo early invasive coronary angiography with an eye toward intervention for sufficiently stenotic lesions. Considering recent data from trials like ORBITA and ISCHEMIA that have once again brought medical management to the fore in patients with stable angina, it is but prudent to ask ourselves if the initial investigative modality of choice should also be a noninvasive test like a CT angiogram vs a more conventional approach of doing an invasive coronary angiogram. This study by the DISCHARGE trial group found that initial CT angiography strategy was a safer strategy in patients with stable angina and an intermediate pretest probability of CAD.
Article 3: Structural Heart Disease Intervention
Which Patients With Aortic Stenosis Should Be Referred to Surgery Rather Than Transcatheter Aortic Valve implantation?
Eur Heart J. 2022, April 25;ehac105.
Stephan Windecker, Taishi Okuno, Axel Unbehaun, Michael Mack, Samir Kapadia, Volkmar Falk.
Abstract
Transcatheter aortic valve implantation (TAVI) has matured into a standard treatment option for patients with severe symptomatic aortic valve stenosis (AS) across the whole spectrum of risk. The advances in the interventional treatment of AS raise the question of which patients with severe AS should be referred to surgery. The myriad of clinical permutations does not allow providing a single, uniform treatment strategy. Rather, the advent of TAVI along with established surgical aortic valve replacement (SAVR) fundamentally enforces the role of the multidisciplinary heart team for decision-making, recommending the best individual choice of the 2 options based on a thorough review of clinical and anatomical factors as well as lifetime management considerations. Involvement of the informed patient expressing treatment preferences is a key for a shared decision-making process. Herein, we provide an in-depth review of evidence informing the decision-making process between TAVI and SAVR and key elements for treatment selection. Special attention is given to the populations that have been excluded from randomized clinical trials, and also lifetime management strategies of patients with severe AS are proposed.
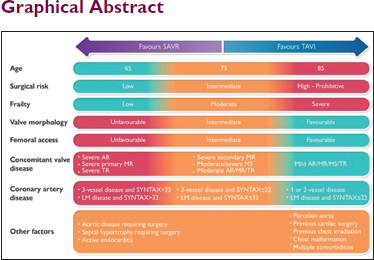
Reviewer Comments: TAVI is here to stay. It has established itself as a standard of care for patients with severe AS and not just in the high surgical risk patients anymore. So, is there a case yet to be made for SAVR? It is this pertinent question that this review beautifully focuses on.
The treatment of aortic stenosis (AS) should be accomplished aiming to restore long-term life expectancy and improve quality of life. For now, only the SAVR is established to restore the prognosis of patients with symptomatic severe AS with long-term post-operative survival becoming comparable to an age- and sex-matched general population without AS in patients over 65 years old.
The PARTNER 2 cohort A trial has shown noninferiority of TAVI at 2 years. Although no differences in the primary outcome were found at 5 years, the authors reported a 27% higher risk of death or disabling stroke between 2 and 5 years after TAVI than after SAVR. In the PARTNER-3 trial, the event-rate lines for death and disabling strokes, which significantly favored TAVI in the 1-year analysis, at the 2-year follow-up curves converge over time, which requires longer-term follow-up before making robust recommendations in this group of patients. Recently, the 5-year data of the SURTAVI trial (intermediate-risk patients with 80 years old mean age) revealed similar mortality, stroke, functional class, and quality of life outcomes between TAVI and SAVR. There was a higher incidence of pacemaker implantation, reintervention, and paravalvular leak with TAVI.
The current ESC/EACTS Guidelines have disregarded the option of SAVR in operable patients with high risk for surgery, placing these patients altogether in the same recommendation as inoperable patients. In contrast to these professional society guidelines, the National for Health and Care Excellence (NICE) taking a multidisciplinary and societal recommend surgery as first-line treatment in patients with low and intermediate surgical risk and offer TAVI only when surgery is unsuitable or at high risk.
Current evidence supports TAVI for inoperable patients or elderly, high-risk patients with short life expectancy and has confirmed the noninferiority of TAVI to SAVR in the short and intermediate term across the spectrum of surgical risk patients and therefore should be considered as a complementary treatment strategy to SAVR. Unfortunately, the evidence to conclusively support a universal preference for TAVR in all intermediate to high risk or elderly patients is not present. Until we have conclusive evidence of superiority and long-term outcomes of TAVI, SAVR is here to stay too.
Article 4: Heart Failure
Lung Function Impairment and Risk of Incident Heart Failure: The NHLBI Pooled Cohorts Study
Eur Heart J. 2022, April 25;ehac205.
Christina M Eckhardt, Pallavi P Balte, Robert Graham Barr, Alain G Bertoni, Surya P Bhatt, Michael Cuttica, Patricia A Cassano, Paolo Chaves, David Couper, David R Jacobs, Ravi Kalhan, Richard Kronmal, Leslie Lange, Laura Loehr, Stephanie J London, George T O’Connor, Wayne Rosamond, Jason Sanders, Joseph E Schwartz, Amil Shah, Sanjiv J Shah, Lewis Smith, Wendy White, Sachin Yende, Elizabeth C Oelsner.
Abstract
Aims The aim is to evaluate associations of lung function impairment with risk of incident heart failure (HF).
Methods and Results: Data were pooled across 8 US population-based cohorts that enrolled participants from 1987 to 2004. Participants with self-reported baseline cardiovascular disease were excluded. Spirometry was used to define obstructive (forced expiratory volume in 1 s/forced vital capacity [FEV1/FVC] <0.70 )or restrictive (FEV1/FVC ≥0.70, FVC <80%) lung physiology. The incident HF was defined as hospitalization or death caused by HF. In a subset, HF events were subclassified as HF with reduced ejection fraction (HFrEF; EF <50%) or preserved EF (HFpEF; EF ≥50%). The Fine-Gray proportional subdistribution hazards models were adjusted for sociodemographic factors, smoking, and cardiovascular risk factors. In models of incident HF subtypes, HFrEF, HFpEF, and non-HF mortality were treated as competing risks. Among 31,677 adults, there were 3,344 incident HF events over a median follow-up of 21.0 years. Of 2,066 classifiable HF events, 1,030 were classified as HFrEF and 1,036 as HFpEF. Obstructive (adjusted hazard ratio [HR] 1.17, 95% confidence interval [CI] 1.07-1.27) and restrictive physiology (adjusted HR 1.43, 95% CI 1.27-1.62) were associated with incident HF. Obstructive and restrictive ventilatory defects were associated with HFpEF but not HFrEF. The magnitude of the association between restrictive physiology and HFpEF was similar to associations with hypertension, diabetes, and smoking.
Conclusion: Lung function impairment was associated with increased risk of incident HF, and particularly incident HFpEF, independent of and to a similar extent as major known cardiovascular risk factors.
Reviewer Comments: The definition of heart failure has undergone a dramatic change over the last decade to accommodate for advances in our understanding of the pathogenesis of this disease. The treatment options available to the cardiologist today for the management of HF have given many a patient a new lease of life, and a good quality life at that!
Heart failure with preserved ejection fraction (HFpEF) remains an enigma. Improving clinical outcomes in patients with this subset of HF is perhaps the greatest challenge facing cardiologists today. Most of the “big boys” (ARNI/ACE/ARB, BB, MRA) that have shown benefit in HFrEF have shown little to no benefit in HFpEF. Empagliflozin by showing demonstrable mortality benefit in the HFpEF subset (EMPEROR-PRESERVED) has brought about a fresh ray of hope in the management of these patients.
Our understanding of HFpEF has changed from conceptualizing HFpEF as an entity defined by cardiogenic pulmonary edema in the setting of impaired LV lusitropy to a wider syndrome involving variable patterns of pulmonary vascular, adipose-endocrine, and neurohumoral axis dysfunction. The predominant HFpEF symptomatology of dyspnoea, exercise limitation, and diminished functional class is driven by a complex pathophysiology that often involves extracardiac organ systems, among which, pulmonary dysfunction is a major contributor to exercise intolerance of patients. This is due to an altered ventilatory reserve, impaired gas diffusion, increased dead space, VQ mismatch, restrictive and obstructive defects, obstructive and centra sleep apnea, pulmonary vascular remodeling, and pulmonary hypertension.
In this study, Eckhart et al analyzed associations between lung diagnoses and incident HF hospitalization and mortality. The study results point to the fact that probably lung disease in a patient with HF must no longer be regarded as a bystander in at-risk patients but should rather be taken as a clinically relevant component of the HFpEF syndrome which when present merits consideration as a high-risk finding in individual patients. It would be wise to remember that the ‘
Article 5: Structural Heart Disease
Association of Annual N-Terminal Pro-Brain Natriuretic Peptide Measurements With Clinical Events in Patients With Asymptomatic Nonsevere Aortic Stenosis—A Post Hoc Substudy of the SEAS Trial
JAMA Cardiol. 2022, April 1;7(4):435-444.
Edina Hadziselimovic, Anders M. Greve, Ahmad Sajadieh, Michael H. Olsen, Y. Antero Kesäniemi, Christoph A. Nienaber, Simon G. Ray, Anne B. Rossebø, Ronnie Willenheimer, Kristian Wachtell, Olav W. Nielsen.
Abstract
Importance: Recent studies have questioned the presumed low-risk status of patients with asymptomatic nonsevere aortic stenosis (AS). Whether annual N-terminal probrain natriuretic peptide (NT-proBNP) measurements are useful for risk assessment is unknown.
Objective: To assess the association of annual NT-proBNP measurements with clinical outcomes in patients with nonsevere AS.
Design, Setting, and Participants: Analysis of annual NT-proBNP concentrations in the multicenter, double-blind Simvastatin and Ezetimibe in Aortic Stenosis (SEAS) randomized clinical trial was performed. SEAS was conducted from January 6, 2003, to April 1, 2008. Blood samples were analyzed in 2016, and data analysis was performed from February 10 to October 10, 2021. SEAS included 1,873 patients with asymptomatic AS not requiring statin therapy with transaortic maximal flow velocity from 2.5 to 4.0 m/s and preserved ejection fraction. This substudy included 1,644 patients (87.8%) with available blood samples at baseline and year 1.
Exposures: Increased age- and sex-adjusted NT-proBNP concentrations at year 1 and a 1.5-fold or greater relative NT-proBNP concentration change from baseline to year 1. Moderate AS was defined as baseline maximal flow velocity greater than or equal to 3.0 m/s.
Main Outcomes and Measures: Aortic valve events (AVEs), which are a composite of aortic valve replacement, cardiovascular death, or incident heart failure due to AS progression, were noted. Landmark analyses from year 1 examined the association of NT-proBNP concentrations with outcomes.
Results: Among 1,644 patients, 996 were men (60.6%); mean (SD) age was 67.5 (9.7) years. Adjusted NT-proBNP concentrations were within the reference range (normal) in 1,228 of 1,594 patients (77.0%) with NT-proBNP values available at baseline and in 1,164 of 1,644 patients (70.8%) at year 1. During the next 2 years of follow-up, the AVE rates per 100 patient-years for normal vs increased adjusted NT-proBNP levels at year 1 were 1.39 (95% CI, 0.86-2.23) vs 7.05 (95% CI, 4.60-10.81) for patients with mild AS (P < .01), and 10.38 (95% CI, 8.56-12.59) vs 26.20 (95% CI, 22.03-31.15) for those with moderate AS (P < .01). Corresponding all-cause mortality rates were 1.05 (95% CI, 0.61-1.81) vs 4.17 (95% CI, 2.42-7.19) for patients with mild AS (P < .01), and 1.60 (95% CI, 0.99-2.57) vs 4.78 (95% CI, 3.32-6.87) for those with moderate AS (P < .01). In multivariable Cox proportional hazards regression models, the combination of a 1-year increased adjusted NT-proBNP level and 1.5-fold or greater NT-proBNP level change from baseline was associated with the highest AVE rates in both patients with mild AS (hazard ratio, 8.12; 95% CI, 3.53-18.66; P < .001) and those with moderate AS (hazard ratio, 4.05; 95% CI, 2.84-5.77; P < .001).
Conclusions and Relevance: The findings of this study suggest that normal NT-proBNP concentrations at 1-year follow-up are associated with low AVE and all-cause mortality rates in patients with asymptomatic nonsevere AS. Conversely, an increased 1-year NT-proBNP level combined with a 50% or greater increase from baseline may be associated with high AVE rates.
Reviewer Comments: N-terminal probrain natriuretic peptide (NT-proBNP) is a marker of ventricular stretch and is hence a useful diagnostic and prognostic tool in patients with HF. Apart from its role in HF, it has also been used as a prognostic tool in the assessment and follow up of patients with nonsevere asymptomatic aortic stenosis. The question is that whether an NT-proBNP level is within the reference range or an unchanged level during follow-up associated with a low clinical risk in patients with asymptomatic nonsevere AS.
In this substudy of a randomized clinical trial comprising 1,644 patients with asymptomatic nonsevere AS, an NT-proBNP level within the reference range was detected in 1,164 patients at 1-year follow-up. Patients who had NT-proBNP concentrations within the reference range had subsequent annual mortality rates of 1.05 (mild AS) and 1.60 (moderate AS) per 100 person-years; a less than 50% increase in NT-proBNP concentrations from baseline to 1 year was associated with low clinical risk. The findings of this study suggest that NT-proBNP concentrations within the reference range at year 1 are associated with low clinical risk in patients with asymptomatic nonsevere AS and hence is an effective tool for follow-up and prognostication of these patients.
Article 6: LAA Closure
Four-Year Outcomes After Left Atrial Appendage Closure vs Nonwarfarin Oral Anticoagulation for Atrial Fibrillation
J Am Coll Cardiol. 2022, January 4;79(1):1-14.
Pavel Osmancik, Dalibor Herman, Petr Neuzil, Pavel Hala, Milos Taborsky, Petr Kala, Martin Poloczek, Josef Stasek, Ludek Haman, Marian Branny, Jan Chovancik, Pavel Cervinka, Jiri Holy, Tomas Kovarnik, David Zemanek, Stepan Havranek, Vlastimil Vancura, Petr Peichl, Petr Tousek, Veronika Lekesova, Jiri Jarkovsky, Martina Novackova, Klara Benesova, Petr Widimsky, Vivek Y Reddy, PRAGUE-17 Trial Investigators.
Abstract
Background: The PRAGUE-17 (Left Atrial Appendage Closure vs Novel Anticoagulation Agents in Atrial Fibrillation) trial demonstrated that left atrial appendage closure (LAAC) was noninferior to nonwarfarin direct oral anticoagulants (DOACs) for preventing major neurological, cardiovascular, or bleeding events in patients with atrial fibrillation (AF) who were at high risk.
Objectives: This study sought to assess the prespecified long-term (4-year) outcomes in PRAGUE-17.
Methods: PRAGUE-17 was a randomized noninferiority trial comparing percutaneous LAAC (Watchman or Amulet) with DOACs (95% apixaban) in patients with nonvalvular AF and with a history of cardioembolism, clinically relevant bleeding, or both CHA2DS2-VASc ≥3 and HASBLED ≥2. The primary endpoint was a composite of cardioembolic events (stroke, transient ischemic attack, or systemic embolism), cardiovascular death, clinically relevant bleeding, or procedure-/device-related complications (LAAC group only). The primary analysis was modified intention-to-treat.
Results: This study randomized 402 patients with AF (201 per group, age 73.3 ± 7.0 years, 65.7% male, CHA2DS2-VASc 4.7 ±1.5, HASBLED 3.1 ± 0.9). After 3.5 years median follow-up (1,354 patient-years), LAAC was noninferior to DOACs for the primary endpoint by modified intention-to-treat (subdistribution HR [sHR]: 0.81; 95% CI: 0.56-1.18; P = 0.27; P for noninferiority = 0.006). For the components of the composite endpoint, the corresponding sHRs were 0.68 (95% CI: 0.39-1.20; P = 0.19) for cardiovascular death, 1.14 (95% CI: 0.56-2.30; P = 0.72) for all-stroke/transient ischemic attack, 0.75 (95% CI: 0.44-1.27; P = 0.28) for clinically relevant bleeding, and 0.55 (95% CI: 0.31-0.97; P = 0.039) for nonprocedural clinically relevant bleeding. The primary endpoint outcomes were similar in the per-protocol (sHR: 0.80; 95% CI: 0.54-1.18; P = 0.25) and on-treatment (sHR: 0.82; 95% CI: 0.56-1.20; P = 0.30) analyses.
Conclusions: In long-term follow-up of PRAGUE-17, LAAC remains noninferior to DOACs for preventing major cardiovascular, neurological, or bleeding events. Furthermore, nonprocedural bleeding was significantly reduced with LAAC.
Reviewer Comments: A stroke is probably the most debilitating disease to ever afflict man. Hence, it is imperative that we find strategies that eliminate or at least mitigate the risk of stroke to the greatest extent possible. Unfortunately, OAC carry with them a risk of bleeding which even though has been greatly reduced with the advent of NOACs, is not completely eliminated. In patients with a high risk of cardioembolic stroke and a high bleeding risk, LAAC devices are the way to go. Compared to at the time of introduction, these devices have evolved with better safety profiles and ease of deployment. With increasing physician experience, success rates have increased and complication rates have dropped. But do these devices stand the test of time?
Osmancik et al present the prespecified 4-year follow-up of PRAGUE-17 (Left Atrial Appendage Closure vs Novel Anticoagulation Agents in Atrial Fibrillation), a randomized, noninferiority comparison of percutaneous left atrial appendage closure (LAAC) vs direct oral anticoagulants (DOACs). The initial results of PRAGUE-17, reported at a median follow-up of 19.9 months, demonstrated that LAAC was noninferior to DOACs for the primary composite endpoint of stroke, transient ischemic attack, systemic embolism, cardiovascular death, major or nonmajor clinically relevant bleeding, and procedure-/device-related complications. Nearly one-third of the bleeding events in the LAAC group were procedure-related, whereas nonprocedure-related bleeding was more common in the DOAC group (26 vs 13; HR: 0.53; 95% CI: 0.26-1.06). The results of the longer-term follow-up presented in this issue, at a median of 3.5 years, are generally similar to the original report. LAAC remains noninferior to DOACs for the composite endpoint.
Unfortunately, regarding understanding late device-associated risks, PRAGUE-17 is a missed opportunity. To their credit, the investigators had planned to perform transesophageal echocardiograms in the LAAC group 6 to 8 months after randomization. But because of COVID-19, most of these follow-up transesophageal echocardiograms were cancelled. So, although the incidence of late device-related thrombosis and peridevice leaks is not known, the longer-term PRAGUE-17 data are helpful in demonstrating that rates of stroke/systemic embolism remain similar in the LAAC and DOAC groups over time, without any obvious signal of late ischemic events in the LAAC group.
Article 7: Cardiac Imaging
Myocardial Fibrosis Predicts Ventricular Arrhythmias and Sudden Death After Cardiac Electronic Device Implantation
J Am Coll Cardiol. 2022, February 22;79(7):665-678.
Francisco Leyva, Abbasin Zegard, Osita Okafor, Paul Foley, Fraz Umar, Robin J. Taylor, Howard Marshall, Berthold Stegemann, William Moody, Richard P. Steeds, Brian P. Halliday, Daniel J. Hammersley, Richard E. Jones, Sanjay K. Prasad, Tian Qiu.
Abstract
Background: Increasing evidence supports a link between myocardial fibrosis (MF) and ventricular arrhythmias.
Objectives: The purpose of this study was to determine whether presence of myocardial fibrosis on visual assessment (MFVA) and gray zone fibrosis (GZF) mass predicts sudden cardiac death (SCD) and ventricular fibrillation/sustained ventricular tachycardia after cardiac implantable electronic device (CIED) implantation.
Methods: In this prospective study, total fibrosis and GZF mass, quantified using cardiovascular magnetic resonance, was assessed in relation to the primary endpoint of SCD and the secondary, arrhythmic endpoint of SCD or ventricular arrhythmias after CIED implantation.
Results: Among 700 patients (age 68.0 ± 12.0 years), 27 (3.85%) experienced a SCD and 121 (17.3%) met the arrhythmic endpoint over median 6.93 years (IQR: 5.82-9.32 years). MFVA predicted SCD (HR: 26.3; 95% CI: 3.7-3,337; negative predictive value: 100%). In competing risk analyses, MFVA also predicted the arrhythmic endpoint (subdistribution HR: 19.9; 95% CI: 6.4-61.9; negative predictive value: 98.6%). Compared with no MFVA, a GZF mass measured with the 5SD method (GZF5SD) >17 g was associated with highest risk of SCD (HR: 44.6; 95% CI: 6.12-5,685) and the arrhythmic endpoint (subdistribution HR: 30.3; 95% CI: 9.6-95.8). Adding GZF5SD mass to MFVA led to reclassification of 39% for SCD and 50.2% for the arrhythmic endpoint. In contrast, LVEF did not predict either endpoint.
Conclusions: In CIED recipients, MFVA excluded patients at risk of SCD and virtually excluded ventricular arrhythmias. Quantified GZF5SD mass added predictive value in relation to SCD and the arrhythmic endpoint.
Reviewer Comments: Myocardial scar as visualized by cardiac magnetic resonance imaging (CMR) with late gadolinium enhancement (LGE) is associated with increased mortality in patients with cardiomyopathies of all etiologies, including ischemic, nonischemic, hypertrophic, sarcoidosis-associated, chemotherapy-associated, and others. In addition, LGE has been associated with adverse arrhythmia outcomes in patients with heart failure with and without implantable cardioverter-defibrillators (ICDs), as shown in a meta-analysis of 2,580 patients with ischemic or nonischemic cardiomyopathies.
Scar interspersed with healthy myocardium manifests on CMR as the LGE “gray zone” with intermediate signal intensity, which has been associated with re-entrant electrical circuits through viable channels in scar. In patients who are candidates for CRT, it is important to be able to predict the risk of ventricular arrhythmias, because patients with a lower arrhythmia risk may suffice to undergo a CRT pacemaker, eliminating the risk of inappropriate shocks associated with CRT defibrillators and may have a lower erosion/infection risk based on the smaller device size. If a patient’s mode of death is predicted to be arrhythmic, then the CRT defibrillator will be the best choice in most cases, while those predicted to die of progressive pump failure or noncardiac causes may best be served with a CRT pacemaker. Thus, information not only about cardiac function and scar before the CRT implant but also about the likely effect of CRT on left ventricular function would be important, as improved myocardial efficiency is associated with decreased ventricular arrhythmia risk.
Leyva et al in their study report strong associations of visually assessed myocardial fibrosis, gray zone fibrosis mass, and total fibrosis with the primary endpoint of time to SCD, the secondary composite endpoint of SCD or sustained ventricular arrhythmias observed on subsequent device interrogations, and the secondary endpoint of total mortality. The most important potential impact of the paper by Leyva et al is related to the use of CMR for long-term follow-up of ventricular arrhythmia risk. As Leyva et al found that only 2.6% of patients with the arrhythmic secondary endpoint had no LGE, these data could help with risk stratification for a CRT defibrillator versus a CRT pacemaker.
Article 8: Percutaneous coronary intervention
Five-Year Outcomes of PCI Guided by Measurement of Instantaneous Wave-Free Ratio vs Fractional Flow Reserve
J Am Coll Cardiol. 2022, March 15;79(10):965-974.
Matthias Götberg, Karolina Berntorp, Rebecca Rylance, Evald H Christiansen, Troels Yndigegn, Ingibjörg J Gudmundsdottir, Sasha Koul, Lennart Sandhall, Mikael Danielewicz, Lars Jakobsen, Sven-Erik Olsson, Hans Olsson, Elmir Omerovic, Fredrik Calais, Pontus Lindroos, Michael Maeng, Dimitrios Venetsanos, Stefan K James, Amra Kåregren, Jörg Carlsson, Jens Jensen, Ann-Charlotte Karlsson, David Erlinge, Ole Fröbert.
Abstract
Background: Instantaneous wave-free ratio (iFR) is a coronary physiology index used to assess the severity of coronary artery stenosis to guide revascularization. iFR has previously demonstrated noninferior short-term outcome compared to fractional flow reserve (FFR), but data on longer-term outcome have been lacking.
Objectives: The purpose of this study was to investigate the prespecified 5-year follow-up of the primary composite outcome of all-cause mortality, myocardial infarction, and unplanned revascularization of the iFR-SWEDEHEART trial comparing iFR vs FFR in patients with chronic and acute coronary syndromes.
Methods: iFR-SWEDEHEART was a multicenter, controlled, open-label, registry-based randomized clinical trial using the Swedish Coronary Angiography and Angioplasty Registry for enrolment. A total of 2,037 patients were randomized to undergo revascularization guided by iFR or FFR.
Results: No patients were lost to follow-up. At 5 years, the rate of the primary composite endpoint was 21.5% in the iFR group and 19.9% in the FFR group (HR: 1.09; 95% CI: 0.90-1.33). The rates of all-cause death (9.4% vs 7.9%; HR: 1.20; 95% CI: 0.89-1.62), nonfatal myocardial infarction (5.7% vs 5.8%; HR: 1.00; 95% CI: 0.70-1.44), and unplanned revascularization (11.6% vs 11.3%; HR: 1.02; 95% CI: 0.79-1.32) were also not different between the 2 groups. The outcomes were consistent across prespecified subgroups.
Conclusions: In patients with chronic or acute coronary syndromes, an iFR-guided revascularization strategy was associated with no difference in the 5-year composite outcome of death, myocardial infarction, and unplanned revascularization compared with an FFR-guided revascularization strategy.
Reviewer Comments: iFR was first presented in the ADVISE (ADenosine Vasodilator Independent Stenosis Evaluation) study in 2011. This small 157 patient study observed that it was possible to obtain similar measures of stenosis severity to FFR using iFR, but, importantly without the need for administration of hyperemic agents such as adenosine. Despite several potential benefits of iFR, this promising technology was initially dismissed by many.
Götberg et al present the final 5-year results of the iFR-SWEDEHEART (Instantaneous Wave-free Ratio vs Fractional Flow Reserve in Patients with Stable Angina Pectoris or Acute Coronary Syndrome) study. This study combined with DEFINE-FLAIR (Functional Lesion Assessment of Intermediate Stenosis to Guide Revascularization) was developed to test the applicability of instantaneous wave-free ratio (iFR) as an alternative nonhyperemic method to fractional flow reserve (FFR) for invasive revascularization decision-making in the catheter laboratory. The results of iFR-SWEDEHEART confirm the original hypothesis that iFR is noninferior to FFR and therefore can be used as an alternative to FFR for clinical decision-making. At 5 years follow-up, there was no statistically significant difference in end points between the iFR and FFR groups.
Article 9: Heart Failure
Criteria for Iron Deficiency in Patients With Heart Failure
J Am Coll Cardiol. 2022, February 1;79(4):341-351.
Gabriele Masini, Fraser J Graham, Pierpaolo Pellicori, John G F Cleland, Joseph J Cuthbert, Syed Kazmi, Riccardo M Inciardi, Andrew L Clark.
Abstract
Background: Guidelines on heart failure (HF) define iron deficiency (ID) as a serum ferritin <100 ng/mL or, when 100 to 299 ng/mL, a transferrin saturation (TSAT) <20%. Inflammation (common in HF) may hinder interpretation of serum ferritin.
Objectives: This study sought to investigate how different definitions of ID affect its prevalence and relationship to prognosis in ambulatory patients with chronic HF.
Methods: Prevalence, relationship with patients’ characteristics, and outcomes of various ID definitions were evaluated among patients with HF referred to a regional clinic (Hull LifeLab) from 2001 to 2019.
Results: Of 4,422 patients with HF (median age 75 years [range: 68-82 years], 60% men, 32% with reduced left ventricular ejection fraction), 46% had TSAT <20%, 48% had serum iron ≤13 µmol/L, 57% had serum ferritin <100 ng/mL, and 68% fulfilled current guideline criteria for ID, of whom 35% had a TSAT >20%. Irrespective of definition, ID was more common in women and those with more severe symptoms, anemia, or preserved ejection fraction. TSAT <20% and serum iron ≤13 µmol/L, but not guideline criteria, were associated with higher 5-year mortality (HR: 1.27; 95% CI: 1.14-1.43; P < 0.001; and HR: 1.37; 95% CI: 1.22-1.54; P < 0.001, respectively). Serum ferritin <100 ng/mL tended to be associated with lower mortality (HR: 0.91; 95% CI: 0.81-1.01; P = 0.09).
Conclusions: Different definitions of ID provide discordant results for prevalence and prognosis. Definitions lacking specificity may attenuate the benefits of intravenous iron observed in trials while definitions lacking sensitivity may exclude patients who should receive intravenous iron. Prespecified subgroup analyses of ongoing randomized trials should address this issue.
Reviewer Comments: Iron is essential to the maintenance of the oxygen-carrying capacity of the blood and for oxygen transport, delivery, and utilization. In addition to being a key component of hemoglobin, myoglobin, and other enzymes involved in cellular respiration, oxidative phosphorylation, citric acid cycle, nitric oxide generation, and oxygen radical production, iron is necessary to maintain the structure and function of metabolically active cells, including myocytes and skeletal muscle cells. As such, deficiency of iron is associated with significant impact on the structure and function of numerous organs, including heart.
Iron deficiency (ID) is present in almost 50% of patients with heart failure (HF), regardless of sex, race, anemia, and left ventricular ejection fraction (LVEF). ID can be due to a decrease in total body iron (absolute ID), or to iron sequestration in the storage pool (functional ID) or both. Regardless of type, ID is associated with impaired exercise capacity and quality of life and an unfavorable prognosis independently of anemia and LVEF.
Masini et al have investigated the effect of different ID definitions on the prognosis of 4,442 patients. The results provide important guidance to clinicians evaluating their patients with HF, in whom a TSAT <20% or serum iron level ≤13 µmol/L should be considered the most reliable approach for the detection of ID. These results also identify a path forward for further research efforts to best identify those with ID and study its treatment. In the future, better definitions of ID and treatments superior to intravenous iron should be investigated. Diagnostically, soluble transferrin receptor levels may have the strongest correlation with the gold standard of bone marrow iron deficit, whereas new treatments such as blockade of hepcidin, a key modulator of iron absorption and distribution, may emerge as an effective treatment for both absolute and functional ID.
Article 10: Syncope
Effect of Yoga on Clinical Outcomes and Quality of Life in Patients With Vasovagal Syncope (LIVE-Yoga)
JACC Clin Electrophysiol. 2022, February;8(2):141-149.
Gautam Sharma, Venkatakrishnan Ramakumar, Mohd Sharique, Rohit Bhatia, Nitish Naik, Sriloy Mohanty, Aman Agarwal, Mohini Meti, Akriti Shukla, Siddharthan Deepti, Raghav Bansal, Anunay Gupta, A. Shaheer Ahmed, R.M. Pandey, Rajiv Narang, Sundeep Mishra, Anita Saxena, Rajnish Juneja, and on behalf of the LIVE-Yoga Investigators.
Abstract
Objectives: This study aims to determine the impact of yoga as an adjunct to standard therapy vs standard therapy alone on the symptomatic burden in patients with recurrent vasovagal syncope (VVS).
Background: There is a significant reduction in the quality of life (QoL) of patients with recurrent VVS. Existing management therapies have been largely ineffective. Recent trials have demonstrated the efficacy of yoga in diseases with autonomic imbalance, suggesting its possible utility in VVS.
Methods: Patients with recurrent VVS were randomized to receive either a specialized yoga training program in addition to current guideline-based therapy (intervention arm, group 1) or current guideline-based therapy alone (control arm, group 2). The primary outcome was a composite of the number of episodes of syncope and presyncope at 12 months. Secondary outcomes included QoL assessment by World Health Organization Quality of Life Brief Field questionnaire (WHOQoL-BREF) scores and Syncope Functional Status Questionnaire scores at 12 months, head up tilt test, and heart rate variability at 6 weeks.
Results: A total of 55 patients underwent randomization. The mean number of syncopal or presyncopal events at 12 months was 0.7 ± 0.7 in the intervention arm compared to 2.52 ± 1.93 in the control arm (P < .01). In the intervention arm, 13 (43.3%) patients remained free of events vs 4 (16.0%) patients in the control arm (P = .02). QoL at 12 months showed significant improvement of all Syncope Functional Status Questionnaire scores and 2 domains of WHOQoL-BREF scores (P < .05).
Conclusions: Yoga as adjunctive therapy is superior to standard therapy alone in reducing the symptomatic burden and improving QoL in patients with recurrent VVS.
Article 10b
“Tadasana” Yoga Maneuver for Preventing Vasovagal Syncope Recurrences: A Pilot Study
J Am Coll Cardiol EP. 2022, February;8(2):253-254.
B. Hygriv Rao, Vyshnavi Gowlikar, Sudhindra Vooturi, David G. Benditt, H. Nagraj Rao, Mohandas Surath.
Abstract
Patients with vasovagal syncope (VVS) were randomized to Tadasana group and conventional therapy. In the Tadasana group, there was a significant decrease in syncopal (108 in 48 patients pretreatment to 0 posttreatment, P < .001) as well as near-syncope events (269 in 33 patients pretreatment to 6 in 5 patients posttreatment, P < .001). The reduction in mean total events was greater in the Tadasana group than in the conventional treatment group (P = .01). The authors concluded that Tadasana resulted in greater reduction in both syncope and near-syncope events.
Reviewer Comments: Vasovagal syncope is the commonest cause of syncope in patients presenting to any cardiovascular or neurological clinic. Recurrent VVS has a deleterious effect on the quality of life and represents a significant health-care system burden. For a disease so common, evidence-based treatment strategies are surprisingly few. There are very few clinical trial proven interventions to reduce the frequency of spells and the patients QoL. Drug therapy has shown limited benefit and is neither first line nor standard of care. Yoga practice is thought to exert its benefits through changes in the patient’s physical, psychological, and autonomic state. Two studies by Gautam Sharma et al and Hygriv Rao et al have independently shown that Yoga maneuvers can independently reduce the frequency of syncope and near-syncope events in patients with VVS. Larger studies are needed but this exciting data shows that if it is confirmed in future studies to be of benefit, yoga may become an effective and inexpensive adjunctive treatment for patients with recurrent VVS.