
Abstract
Case of an arrhythmogenic right ventricular cardiomyopathy with associated arrhythmias discussing classical electrocardiogram and intracardiac electrogram findings.
Case
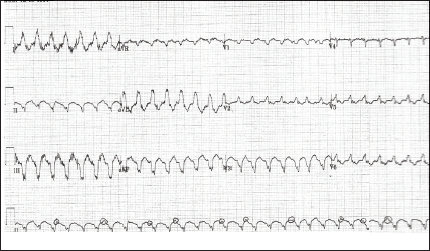
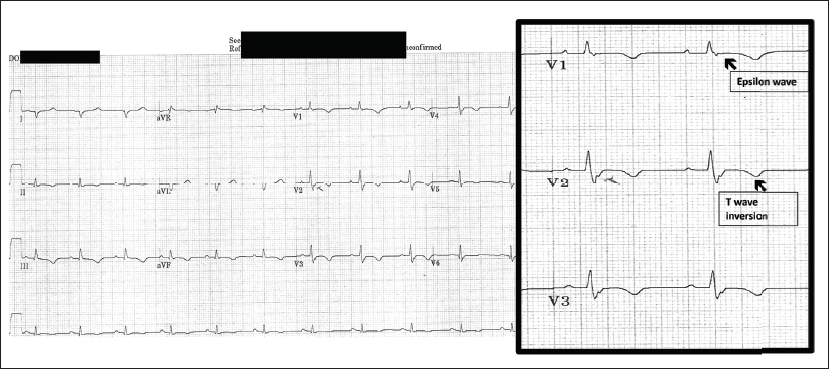
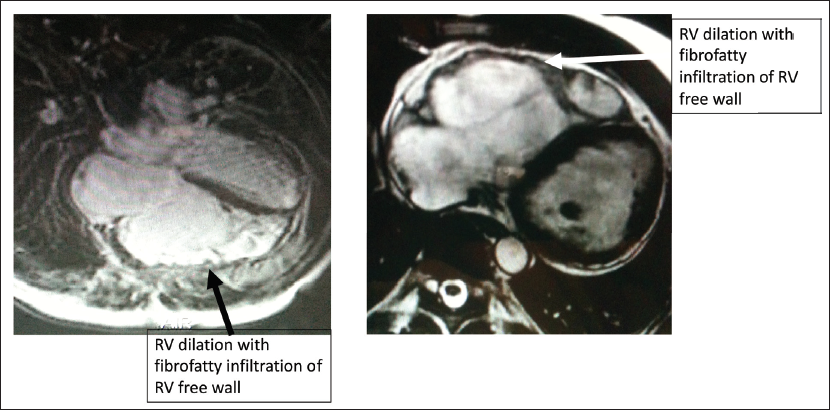
Pt is a 49-year-old male and has no prior cardiac or medical history with recurrent syncope episodes and was brought by emergency medical services to the hospital. He was noted to have hemodynamically significant (hypotension with systolic blood pressure in 70 mm Hg) wide complex tachycardia (WCT) (Figure 1) at a rate of 150 to 160 bpm requiring emergency cardioversion in the emergency room. Postconversion, sinus rhythm (SR) electrocardiogram (ECG) revealed features described in Figure 2 suggestive of arrhythmogenic right ventricular cardiomyopathy (ARVC). Pt had recurrent episodes of WCT requiring antiarrhythmic drug therapy and subsequent cardioversions. He underwent cardiac catheterization with no significant epicardial coronary artery disease. Echocardiogram and cardiac MRI demonstrated typical features of ARVC (Figure 3). He underwent an electrophysiology study (EPS) during which the presenting clinical WCT was easily inducible and was confirmed as ventricular tachycardia (VT) with ventriculoatrial (VA) dissociation (Figure 4). Voltage map of the right ventricle (RV) was also performed during the EP study. Given recurrent VT episodes and cardioversions, he underwent VT ablation and subsequently underwent implantable cardioverter defibrillator (ICD) insertion without any complications. He later underwent a genetic study which confirmed the homozygous mutation of desmocollin-2, strongly suggestive to predispose to ARVC. Pt is now >5 years postablation and ICD implant with no further clinical VT episodes and/or ICD shocks.
Electrocardiogram showing left bundle superior axis ventricular tachycardia with AV dissociation.
Electrocardiogram in Sinus Rhythm With IVCD (QRS >110 ms), Epsilon Waves, and T Wave Inversion (TWI) in Right Precordial Leads (V2 and V3).
Cardiac MRI Demonstrating Right Ventricle (RV) Dilation and Fibrofatty Infiltration of RV Free Wall.
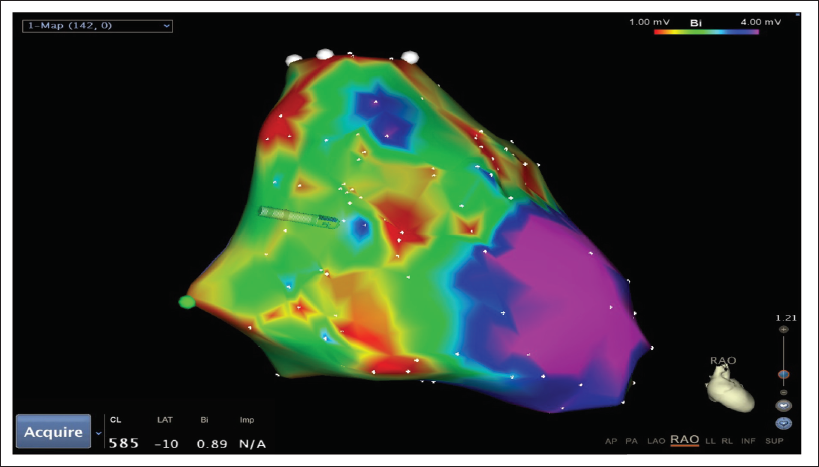
Electrophysiology Study (EPS) With Ventricular Extrastimulation (VEST) Inducing Ventricular Tachycardia With VA Dissociation Demonstrated by Ventricular and Atrial Intracardiac Electrograms.

ECG Features of ARVC During Sinus Rhythm and During Ventricular Tachycardia
Sinus Rhythm ECG (Figure 2)
Depolarization/Conduction abnormalities of intraventricular conduction delay (IVCD) with QRS duration of >110 ms and Epsilon wave.
Repolarization abnormality of inverted T waves in the right precordial leads (V2 and V3).
Ventricular Tachycardia ECG (Figure 1)
Characteristic left bundle branch block VT.
EP Study Characteristics
Patient in SR at baseline during EPS with IVCD with QRS duration of 112 ms. EPS showed normal antegrade AV nodal conduction and no VA conduction at pacing cycle length of 600 ms. V-stimulation using extra stimuli technique readily induced VT with QRS morphology (left bundle-left superior axis) with tachycardia cycle length of 380 ms. There was clear documentation of VA dissociation on intracardiac ECGs (Figure 4). Voltage map of the RV was performed during EPS in SR and demonstrated multiple low-voltage areas (<1.2 mV) at RV inferior base near the tricuspid valve, RV outflow tract (RVOT) and RV free wall (red and green areas on Figure 5). Normal voltage was noted in RV anterior apex and RV septum (Pink areas in Figure 5).
Clinical vignettes in this case:
Identification of VT on the ECG. Pathognomic ECG features of ARVC during SR and during VT. Intracardiac electrograms during EPS in ARVC.
Footnotes
Acknowledgement
Sindhu Nagarakanti for assistance with figures and editing.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.