
Abstract
A young, 18-year-old lady presented with history of chest pain on exertion typical of angina. General examination revealed multiple tendon xanthomas. Systemic examination was unremarkable. Electrocardiogram showed segment (ST) depression in inferior and lateral leads. Echocardiogram revealed normal left ventricular systolic function and no left ventricular regional wall motion abnormalities. Diastolic flow turbulence was noted in the left main coronary artery and proximal left anterior descending artery on color Doppler interrogation across the coronary arteries. Lipid profile showed unusually high total cholesterol and low-density lipoprotein cholesterol. Subsequent evaluation with coronary angiogram revealed triple vessel coronary artery disease. The patient underwent coronary artery bypass surgery and is on antiplatelet and lipid-lowering drug therapy.
Introduction
Premature coronary artery disease (CAD) occurs as a result of various conditions like familial hypercholesterolemia (FH), aorto-arteritis, systemic lupus erythematosus, anomalous coronary arteries, coagulation disorders, spasm or inflammation of the coronary arteries, radiotherapy for thoracic tumors, cocaine abuse, or thromboembolism. FH is an autosomal-dominant disorder leading to primary dyslipidemia, and it affects 1 in 200 to 300 of general population. 1 It results from the genetic mutations in low-density lipoprotein (LDL) cholesterol receptors in liver and other organs. This leads to hyperlipidemia with markedly elevated LDL cholesterol and severe atherosclerosis and premature atherosclerotic cardiovascular disease.
Case Presentation
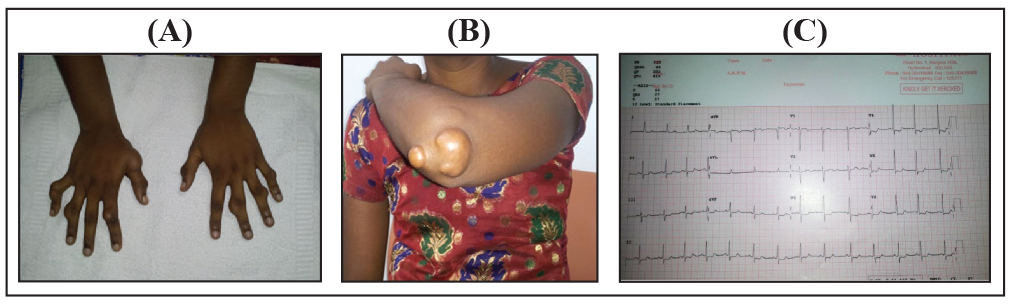
An 18-year-old young lady presented with chief complaint of exertional angina since 2 months. Initially grade II angina according to Canadian Cardiovascular Society Angina Grading Scale, and gradual progression to grade III angina since 1 week. She also had dyspnea on exertion with palpitations. There was no history of syncope. She had family history of CAD and her mother had died at young age due to myocardial infarction. On examination she was hemodynamically stable. General examination revealed multiple tendon xanthomas over fingers (Figure 1[A]), elbow of both upper extremities (Figure 1[B]), and extensor aspects of tibia of both legs. She did not have arterial bruit over any of the arteries. Cardiovascular and other system examination was unremarkable. 12 lead electrocardiogram showed ST depression in inferior and lateral leads and ST elevation in aVR (Figure 1[C]).
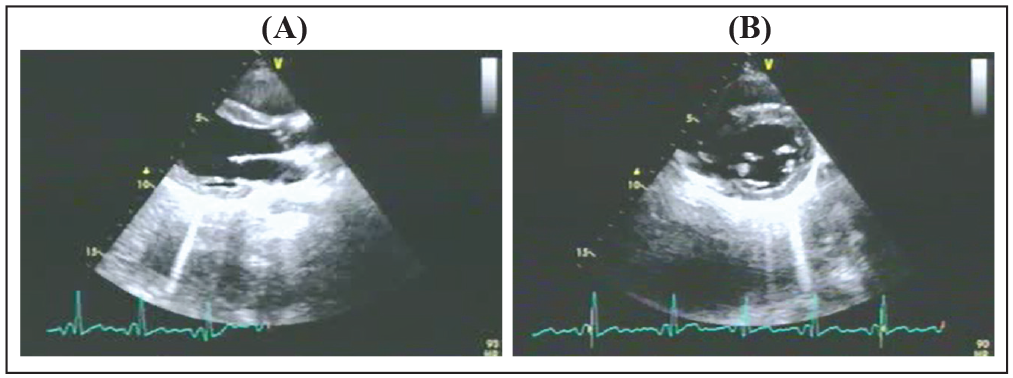
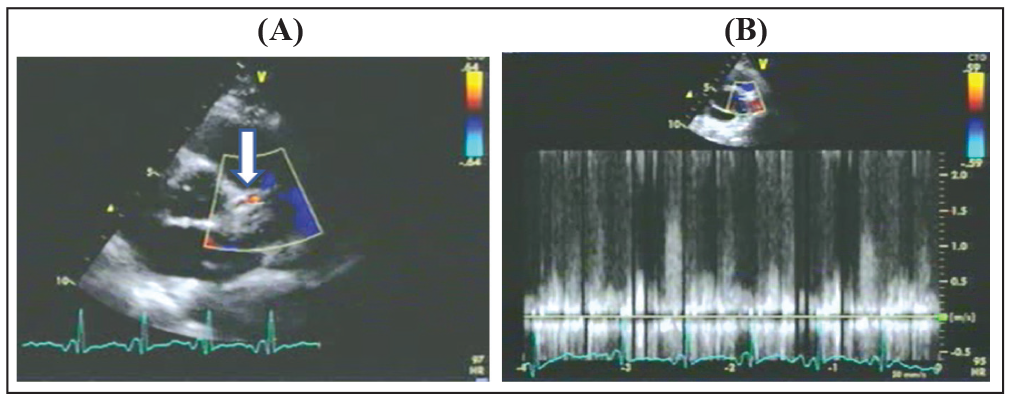
Transthoracic echocardiogram revealed normal size cardiac chambers (Figure 2[A] and [B]) with normal left ventricular systolic function and no left ventricular regional wall motion abnormalities. Atrioventricular and semilunar valves were normal with the presence of mild aortic regurgitation. Color Doppler interrogation across the coronary arteries revealed flow turbulence in the left main coronary artery (LMCA) and proximal left anterior descending (LAD) artery (Figure 3[A]). Pulsed wave Doppler interrogation at the proximal LAD revealed peak diastolic flow velocity >1.5 m/s (Figure 3[B]). Mosaic flow and/or peak diastolic velocity of greater than or equal to 1.5 m/s is considered abnormal and has sensitivity of 85% and positive predictive value of 82.5% for LMCA stenosis by coronary angiography. 2 Echocardiographic study was suggestive of significant LAD stenosis.
Fasting lipid profile showed unusually high total cholesterol of 652 mg/dL, LDL of 551 mg/dL, a high-density lipoprotein (HDL) of 35 mg/dL, a very low-density of 17 mg/dL, and triglycerides of 100 mg/dL.
Genetic studies could not be done due to cost constraints. Although homozygous FH is very likely diagnoses in this case, it could not be confirmed by genetic analysis.
She was diagnosed as a case of familial hypercholesterolemia with CAD with unstable angina, normal sinus rhythm with normal left ventricular systolic function.
(A and B) Photographs show skin xanthomas over fingers and left elbow. (C) 12 lead electrocardiogram showing ST depression in leads 2, 3, aVF and V3 to V6, and ST elevation in aVR.
(A and B) Transthoracic echocardiographic images demonstrating parasternal long axis and parasternal short axis views showing normal size left atrium and left ventricle, respectively.
(A) Transthoracic echocardiographic image demonstrating the color flow turbulence in the proximal LAD coronary artery indicated by the arrow. (B) Pulsed wave Doppler interrogation at the proximal LAD artery showing the peak diastolic flow velocity >1.5 m/s.
(A, B, and C) Coronary angiographic images demonstrating the stenotic lesions in the left anterior descending, left circumflex, and right coronary arteries, respectively.
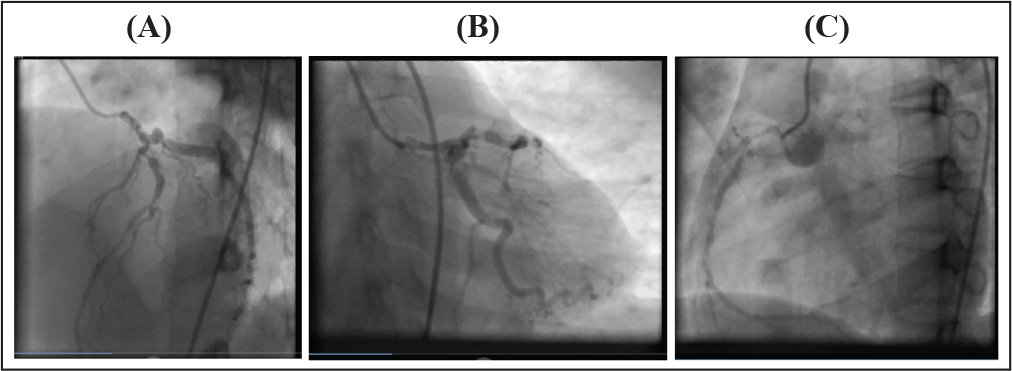
Coronary angiogram was done. It revealed 40% to 50% eccentric stenosis in the LMCA. LAD had proximal 90% stenosis followed by discrete 90% stenosis at second diagonal (D2) bifurcation (Figure 4[A]). Nondominant left circumflex artery had proximal 90% stenosis (Figure 4[B]). Dominant right coronary artery showed ostial 90% stenosis followed by proximal 90% stenosis and diffuse disease in the mid-segment with 40% to 50% eccentric lesion (Figure 4[C]). She was diagnosed to have LMCA with triple vessel disease and advised coronary artery bypass surgery.
Treatment
The patient underwent coronary artery bypass surgery and continued on drug therapy with antiplatelets (aspirin 150 mg once daily and clopidogrel 75 mg once daily) and statin (atorvastatin 80 mg once daily). Patient was also advised proprotein convertase subtilisin/kexin type 9 (PCSK9) antibody inhibitor: evolocumab. But due to cost constraints she was not able to get it. Ezetimibe 10 mg once daily was started at follow-up. Patient’s father was informed about the familial nature of the disease and also the need for screening himself and other family members with lipid profile. The family members were also explained that even after coronary artery bypass graft surgery there may be rapid progression of atherosclerosis and there may be recurrence of the disease. The need for rigorous lipid lowering therapy after surgery was also discussed. The need for liver transplant as the definitive therapy was also discussed with family. They wanted to get the coronary artery bypass graft surgery done to tide over the crisis and plan for liver transplant later, if possible.
Discussion
FH results from mutations in the genes responsible for clearing the LDLs, ie, the LDL receptor (LDL-R) gene (>80% of cases), apolipoprotein B-100 (Apo- B100) gene (5%-10% cases), and proprotein convertase subtilisin/kexin type 9 (PCSK9) gene (<1% cases). Few patients with FH do not exhibit mutation in these 3 genes and may have a polygenic hypercholesterolemia. 3 Heterozygous FH occurs due to genetic mutation in single allele and consequent plasma LDL-C > 190 mg/dL, whereas homozygous FH occurs due to genetic mutation in both alleles and consequent plasma LDL-C > 500 mg/dL. Secondary causes of hyperlipidemia like nephrotic syndrome, hypothyroidism, and liver disease should be excluded. 4
The diagnosis of familial hypercholesterolemia is based on the presence of at least 2 of the following 3 characteristic clinical features.
5
Elevated levels of LDL-C ≥ 190 mg/dL. Skin or tendon xanthomas. Family history of FH or premature (men <55 years, women <60 years) CAD.
The Dutch Lipid Clinic Network criteria are most frequently used for the diagnosis of FH. According to these criteria, the diagnosis of FH is based on the overall score derived from family history, clinical history, physical examination, and biochemical marker: LDL-C level and genetic analysis.
Dutch Lipid Clinic Network Criteria for the Diagnosis of FH 6
Criterion Score Family History
First-degree relative with premature (men <55 years, women <60 years) CAD 1.
OR
First-degree relative with LDL-C > 95th percentile by age and gender for country 1. First-degree relative with tendon xanthoma and/or corneal arcus 2.
OR
Children <18 years with LDL-C > 95th percentile by age and gender for country 2.
Clinical History
Premature (men <55 years, women <60 years) CAD 2.
Premature (men <55 years, women <60 years) cerebral or peripheral vascular disease 1.
Clinical Examination
Tendon xanthomas 6
OR
Corneal arcus at age <45 years 4
Biochemical Marker LDL-C Levels
>330 mg/dL (8.5 mmol/L) 8
250 to 329 mg/dL (6.5-8.5 mmol/L) 5
190 to 249 mg/dL (4.9-6.4 mmol/L) 3
155 to 189 mg/dL (4.0-4.9 mmol/L) 1
Genetic Analysis
The presence of functional LDL-R mutation (in the LDL-R, Apo B, or PCSK9 gene) 8
Diagnosis Based on the Overall Score
Definite >8
Probable 6 to 8
Possible 3 to 5
Unlikely <3.
FH is associated with markedly accelerated atherosclerosis in coronary arteries and other major arteries such as thoracic aorta, carotid arteries, and renal arteries. Premature coronary heart disease manifests in childhood and adolescence with angina and myocardial infarction. Aortic valve is affected by the involvement of the aortic root, resulting in supravalvular aortic stenosis. 7
Early detection of the FH through detailed family history, clinical history, and thorough clinical examination and biochemical tests is mandatory. The management goals in treatment of FH are LDL <100 mg/dL (in adults) and LDL <135 mg/dL (in children) for primary prevention and <70 mg/dL for secondary prevention. 5
The treatment modalities include lifestyle modification, lipid lowering drug therapy, LDL-apheresis, percutaneous or surgical intervention, and finally, liver transplantation in unresponsive cases. Intensive drug therapy with combination of 3-hydroxy-3-methyl-glutaryl-coenzyme A inhibitors, and cholesterol absorption inhibitors such as ezetimibe, fibrates, and nicotinic acid can be used judiciously. Novel drugs include oligonucleotide inhibitors (mipomersen and lomitapide) and PCSK9 antibody inhibitors (alirocumab and evolocumab). These 2 groups of drugs lower the LDL cholesterol on the top of statins. Oligonucleotide inhibitors are costly and associated with high incidence of adverse effects. Hence, PCSK9 antibody inhibitors are preferred over oligonucleotide inhibitors. 8 LDL-apheresis is advocated in patients with FH who are unresponsive to multidrug regimen. However, it is expensive and requires to be done twice a week. Symptomatic patients with critical lesions require percutaneous or surgical intervention according to the number, location, and characteristics of the lesions. It is important to note that there is high risk of recurrence of the disease even after the revascularization. The recurrence is the consequence of the aggressive progression of atherosclerosis due to the genetic defect. Intensive lipid lowering therapy is mandatory even after revascularization. Orthotopic liver transplantation is the curative treatment modality in patients who cannot achieve optimal LDL levels after drug therapy and for patients not able to tolerate LDL apheresis. 9
Conclusion
FH is autosomal-dominant disorder associated with premature coronary heart disease. Early detection and effective therapy improve clinical outcomes. The index case satisfied the criteria for FH and is treated accordingly. Screening of the family members is necessary for early detection of the disease. Intensive drug therapy for lowering the lipids is advocated. Statins are the first line of lipid-lowering drug therapy. The treatment has evolved considerably with the advent of new potent LDL-cholesterol lowering molecules. PCSK9 antibody inhibitors are preferred over oligonucleotide inhibitors. LDL apheresis can be considered in resistant cases. Liver transplant is the definitive therapy.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.