
Abstract
Introduction:
Nursing and medical schools and universities are increasingly integrating palliative and end-of-life care education in their curricula. However, research on the impacts of training and education on future nurses and physicians remains sparse.
Aim of the review:
The aim of this review was to systematically appraise existing research evidence on undergraduate nursing and medical students’ knowledge, perception, and orientation towards palliative and end-of-life care.
Methods:
This international systematic review was conducted between April and May 2021 and was updated in May 2024. A systematic search was conducted in four databases: Hinari ‘Research4Life’, Cumulated Index to Nursing and Allied Health Literature (CINAHL), Google scholar and PubMed. Methodological quality of the included studies was assessed using the Mixed-Methods Appraisal Tool. A data extraction sheet was developed for this review. A convergent integrated approach to mixed-method data synthesis and integration was used to analyse and report the evidence. Braun and Clarke’s inductive and deductive thematic analysis approach was used to identify main themes.
Results:
A total of 64 peer-reviewed research articles met eligibility criteria and were included in the review. Of the 64 eligible research articles, 34 employed a descriptive quantitative cross-sectional design, 11 studies were qualitative, 14 used a quantitative non-randomised design and 5 were mixed methods. The review identified three major thematic categories: (1) students’ knowledge of palliative and end-of-life care, (2) attitude, perception and orientation towards palliative and end-of-life care and (3) predictors of knowledge, orientation, attitude and perception towards palliative and end-of-life care.
Conclusion:
Findings suggest inadequacy and variability in knowledge levels, self-efficacy, willingness, perception and orientation towards palliative care and end-of-life care. Surprisingly, this is common across studies, including those from high-resource countries. Inadequate, limited and/or inconsistent curricula and training content about palliative and end-of-life care is a common theme in the literature.
Plain language summary
Why was the study done? Globally, many nursing and medical training schools and universities are now integrating teaching and training on how to care for people facing life-limiting illnesses in their curricula. However, the distribution and nature of research evidence about future nurses’ and medical doctors’ understanding, views, attitudes, willingness and ability to care for those facing serious illness and the dying remains under reported. What did the researchers do? The researchers searched four online databases which store research publications on healthcare. These were-: Hinari ‘Research4Life’, CINAHL, Google scholar, and PubMed. The search was conducted between April and May 2021 and was updated in May 2024. Retrieved articles were screened against an established eligibility criterion and were assessed for scientific quality using the Mixed Methods Appraisal Tool (MMAT). A sheet was designed for data extraction. Data extracted from eligible studies were analysed, combined and reported using main topics derived both from the study aims and the data. What did the researchers find? 64 research articles were found eligible for inclusion. Of these, 34 reported findings using statistics, 11 studies reported findings in narrative form, 14 involved experimentation, and four used mixed methods. Three main themes emerged-: student’ views and understanding, students’ attitudes and orientation, and factors that influence students’ understanding and attitudes regarding caring for people with life-limiting illness. What do the findings mean? Findings suggest inadequacy and variability in views and understanding, perceived ability, willingness, and attitudes towards working with people with life-limiting illnesses. Inadequate teaching and training and lack of and/or limited real-life and problem-based learning opportunities, particularly interaction with the dying is a common finding in this study.
Keywords
Introduction
Over the last few decades, there has been significant palliative care (PC) development in countries across the globe, including integration of PC training and education into nursing and medical undergraduate curricula. However, PC and end-of-life care (EOLC) are still considerably underappreciated in many parts of the world.1,2 Most of the studies reporting PC development are based in resource-rich regions of the world, mainly Europe3–7 and in Asia.8,9
Education and training in PC are recognised as a core component of the WHO Public Health Model for increasing equitable access to PC.10–12 This is consistent with the 67th World Health Assembly resolution ‘Strengthening of palliative care as a component of comprehensive care throughout the life course’ which mandates governments to ensure PC training is integrated routinely in undergraduate medical and nursing curricula and professional education, and as part of in-service training (continuing professional development) of primary health caregivers. 13 The goal is to ensure trainees acquire knowledge, skills and positive attitudes towards providing appropriate PC and EOLC. Thus, it is important to review and appraise existing literature to understand whether, and to what extent, training and teaching in medical and nursing schools are realising this goal.
The benefit of PC and EOLC, particularly for patients with life-limiting illness, cannot be overemphasised. Research shows that good quality basic as well as specialised PC not only improve patients’ quality-of-life but also reduce costs and spending on healthcare.14–16 In her early grounded theoretical model of death education, experiential and transformative learning in nursing students, Quint 17 reported the positive role of education in influencing students’ attitudes towards caring for seriously ill and dying patients. She found that students who lacked death education held negative attitudes towards the provision of PC and EOLC, and they eventually abandoned caring for dying patients.
Sadly, literature indicates significant deficiencies in knowledge and negative attitudes towards PC among undergraduate nursing students (UNSs) and undergraduate medical students (UMSs).7,18 Inadequate knowledge is cited as one of the commonest barriers to the provision of supportive and PC to patients.19–22 As a result, nursing and medical students continue to graduate from training schools with negative attitudes and lacking basic knowledge, skills and confidence about PC and EOLC, and as a result are often unprepared to provide PC and EOLC to patients and their families.23–26 Inadequate education and deficient curricula in training schools are cited as predominant reasons for this phenomenon.9,27
Furthermore, low to poor knowledge levels and negative perceptions and orientation towards PC and EOL are a growing concern in the general population, patients, and among healthcare professionals (HCPs).10,12,22,28,30,31 Surprisingly, inadequate and/or lack of attention to PC in universities and clinical education has also been cited as one of the main possible factors explaining low/inadequate levels of knowledge of PC among health professionals in high-income countries (HICs) and also in many African countries.22,32,33
The main purpose of this international review is therefore to systematically appraise the available evidence on undergraduate medical and nursing students’ knowledge and perceptions of and orientation towards PC and EOLC and their correlates. The review has the potential to examine crucial insights about the nature, extent, distribution, strengths and gaps in existing evidence and generate actionable recommendations for practice, policy and future research. The review was performed as part of a mixed-methods study that examined UNSs and UMSs knowledge and perceptions of and orientation towards PC in Uganda. The review questions were:
(1) What are final-year medical and nursing undergraduate students’ level of knowledge of PC and EOLC?
(2) What are final-year UMSs and UNSs’ perceptions and orientation towards PC and EOLC?
(3) What are the predictors of knowledge and perceptions of final-year UMSs and UNSs’ towards PC and EOLC?
(4) What factors predict UMSs and UNSs’ orientation towards PC and EOLC?
Methods
Registration
This systematic review is registered on PROSPERO-international register of systematic review, registration number CRD420251171843.
Design and data collection methods
This was an international systematic review of empirical literature on at least one of the three main variables: knowledge, perception and orientation towards PC and EOLC among UNSs and UMSs. A data extraction sheet was developed for this review, including authors’ names, year of publication, country, aims, design, data collection tool, sample and summary of the main findings.
Literature search and search strategy
An iterative and rigorous systematic literature search was conducted by the lead author (G.N.) in trusted databases, that is, Hinari ‘Research4Life’, Cumulated Index to Nursing and Allied Health Literature (CINAHL), Google Scholar and PubMed for rich literature to inform this review. An additional online search was conducted on Google for relevant articles.
The search integrated key free text and of Medical Subject Headings (MeSH) search terms across the databases (Figure 1). Boolean connectors ‘OR’ to widen the search and capture as many relevant articles as possible and ‘AND’ to narrow the search to include articles with literature relevant to the aims of this study were utilised. Key search terms used were: (Undergraduate) AND ((nursing) OR (nurses) OR (medical)) AND (students) AND ((knowledge) OR (attitudes) OR (perceptions) OR (orientation)) (Self-efficacy)) AND ((Palliative Care) OR (end-of-life-care)).

PRISMA flow chart showing search strategy for studies included in the review.
Eligibility criteria
The inclusion and exclusion criteria for this review were underpinned by the PICOST framework 34 as outlined in Table 1:
The PICOST framework for the review question.

EOLC, end-of-life care; PC, palliative care; RCT, randomised controlled trials; UMSs, undergraduate medical students; UNSs, undergraduate nursing students.
Screening of the articles for inclusion
A preliminary screening based on the titles and abstracts of all the search results (n = 860 articles) was conducted by GN. At this stage, 764 articles were excluded as it was obvious they were either not about the topic of interest or the papers were not research based or were duplicates. Full-text screening was then performed independently by GN and PE on each of the remaining (n = 96) articles, and an additional 32 papers were excluded as these were either about knowledge, attitudes, or experiences of working or active nursing and/or medical professionals rather than undergraduate students. To note, there were two disagreements on full-text screening, and these were resolved through consensus. The two papers were excluded as these were about qualified nurses/medical doctors but not undergraduate students, leaving 64 articles that met the inclusion criteria (see Figure 1).
The review was conducted and reported in accordance with Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines for conducting and reporting systematic reviews. 35
Methodological quality of included studies critiqued using Mixed-Methods Appraisal Tool
The remaining 64 articles were screened for methodological quality using the Mixed-Methods Appraisal Tool (MMAT). 36 The MMAT includes criteria for appraising the methodological quality of five broad categories of study designs: (i) qualitative studies, (ii) randomised controlled trials, (iii) non-randomised studies, (iv) quantitative descriptive studies and (v) mixed-methods studies. MMAT was deemed the most appropriate tool as this is a mixed-methods systematic review involving qualitative, quantitative and mixed-methods studies. The screening and critiquing of articles were independently conducted by the first author (G.N.) and second author (P.E.), and disagreements were resolved by consensus.
Each of the studies was appraised using an appropriate MMAT category with seven screening questions. The first two screening questions assessed whether an individual study met basic eligibility criteria – a clear research question and relevance and suitability of the data in answering the research question. Studies that passed initial screening were further subjected to category-specific screening for suitability of the study design, data collection methods, analysis and findings. Each of the seven screening items was assessed against three main responses ‘Yes’, ‘Can’t tell’ and ‘No’. All the papers had an acceptable level of methodological quality on critiquing. Detailed results are presented in Supplemental File.
Synthesis approach
A convergent integrated approach to data synthesis and integration was used. 37 Data extracted from quantitative studies (including data from the quantitative component of mixed-methods studies) and qualitative studies (including data from the qualitative component of mixed-methods studies) were combined and transformed.
Narrative synthesis was utilised for quantitative studies. Quantitative findings were summarised using tables and text, which were later integrated and analysed thematically using Braun and Clarke’s framework. 38
Thematic synthesis integrated both deductive-predetermined themes based on the review aims and inductive approaches, identifying themes from the data. The synthesis followed a four-stepwise approach. (1) Data extraction: GN and PE extracted data from the eligible studies and summarised them in a table (Table 2). (2) Data transformation: Quantitative data was qualitised-converted into qualitative or textual descriptions, categories, typologies, narratives or themes. (3) Integration: Here, qualitised data were compared, combined and pooled with the qualitative data extracted from qualitative studies. The pooled data were read and re-read to identify homogenous data segments that overlapped in meaning to generate broad-based categories or themes. Furthermore, emergent themes were iteratively compared with predetermined themes to generate final master themes. (4) Interpretation: Discussion of the results of the synthesis of qualitative and quantitative evidence in the context of the study aims. The discussion was constructed in such a way that it identified, compared and accounted for areas of convergence (similarities), divergence (differences and contradictions) and complementarity between evidence in the studies, while placing the evidence in the context of the aims of the review (Figure 2).
Summary of findings from eligible articles included in the review.

BSN, Bachelor of Science in Nursing; CDS, Coping with Death Scale; CES, Caring Efficacy Scale; CI, confidence interval; C-JSE-HPS, Chinese version of the Jefferson scale of empathy–health profession students; CYP, children and young people; DAP-R, Death Attitude Profile-Revised Scale; DAS-E, Death Anxiety-Extended Scale; EOLC, end-of-life care; FATCOD, Frommelt Attitudes Toward Care of the Dying Scale; KAOP, Kogan’s Attitudes toward Older People Scale; KAP, knowledge, attitude and practice; KAS, knowledge and attitudes survey; KASRP, knowledge and attitudes survey regarding pain; p, probability at an acceptable confidence level; PBL, problem-based learning; PC, palliative care; PCAK, palliative care assessment knowledge; PCN, palliative care nursing; PCQN, palliative care quiz for nursing questionnaire, PLWHA, people living with HIV/AIDS, PPC, paediatric palliative care; PY, practical year; Q13, interdisciplinary subject 13 palliative care in Germany; SD, standard deviation; SEPC, Self-Efficacy in Palliative Care Scale; TS, Thanatophobia Scale; UMSs, undergraduate medical students; UNSs, undergraduate nursing students.

Convergent integrated approach to data synthesis and integration.
Results
Methodological characteristics of the articles included in the review
Disaggregating the articles based on study design: of the 64 research articles 31 employed a descriptive quantitative cross-sectional design.3,5,6,7,9,18,24–26,29,39–59 Twelve studies were qualitative,60–71 two had mixed-methods design,72,73 eight were quasi experimental with a pre-post intervention design,74–78,81,83,84 three employed a quasi-experimental with a pre-post mixed-method design,79,80,82 two were outcome-evaluations,85,86 two descriptive correlational,87,88 two prospective longitudinal,89,90 one was an intervention control group comparative study 91 and one descriptive analytical study. 92
Stratifying the articles by geographical region and country where the studies were conducted: 28 were conducted in Europe: Turkey,3,6,44,54,91 Germany,55,64,79,85,86 Sweden,5,49,76 United Kingdom,61,67,72 Spain,63,73,78 Poland,7,74 Greece, 42 Ireland, 82 Netherlands, 45 Finland, 66 Switzerland, 46 Italy, Spain and UK, 48 and Greece and UK 19 . Twenty-nine studies were conducted in Asia including: 12 in East Asia: China,9,50,52,57,59,65,70,71,84,88 Hongkong56,80; 10 in West Asia: Palestine,24,25,51 Jordan,26,39,40,47,58 Saudi Arabia, 43 Iran 75 ; 4 in South Asia: India,53,83,87 Nepal 92 ; and 3 in Southeast Asia: Singapore, 68 Thailand, 69 Indonesia. 81
Five studies were conducted in North America (all in United States).29,41,77,89,90 Australia 60 and Africa (Cameroon) 62 had only one study each. See Figure 3.
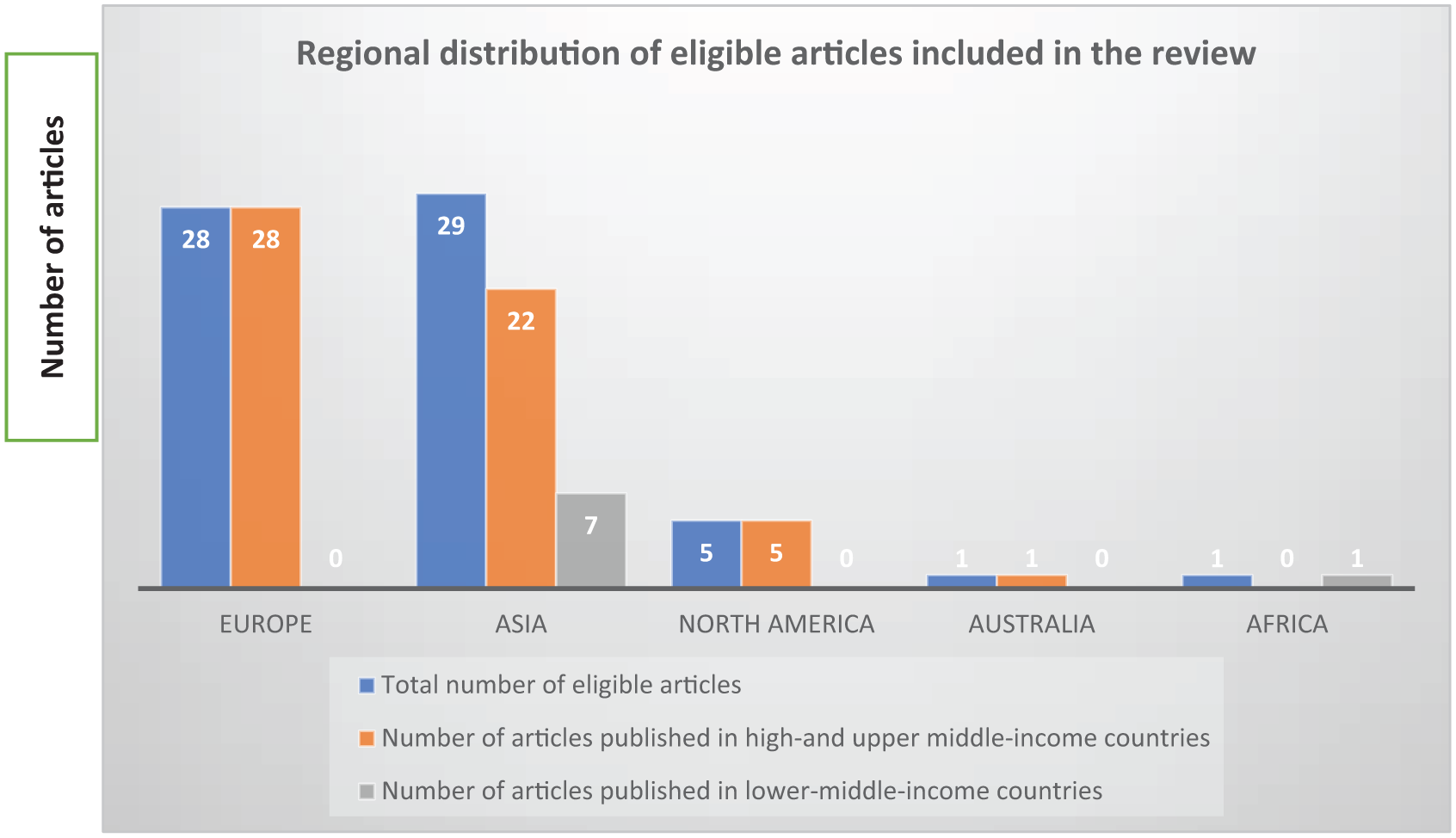
Showing geographical distribution of eligible studies included in the review (n = 64).
Regarding field of study, 40 studies were conducted with UNSs,5,6,9,19,29,24–26,39–41,43,46,48,49, 51 ,52,54,57,59–62,65–72,75,76,78,80,81,84,87,88,91 20 with UMSs3,42,44,45–47,50,55,58,63,64,73,77,79,82,83,85,86–89,90,92 and 4 with both groups7,53,56,74 (See Table 2).
Emergent themes
The review identified three major thematic categories as shown in Figure 4: (1) students’ knowledge of PC and EOLC, (2) Students’ attitude, perception and orientation towards PC and EOLC and (3) predictors of knowledge, attitude and perception towards PC and EOLC.

Interaction between emergent master themes.
Theme 1: Nursing and medical student’s knowledge of PC and EOLC
A wide body of research from both LICs and HMICs reports inadequate and poor knowledge levels of PC and EOLC among UNSs, for example, in Canada, 23 Jordan, 39 Palestine,25,51 Cameroon, 62 Turkey, 6 Poland, 7 United States, 29 China49,85 as well as among UMSs, for example, in Germany,55,79 Turkey,3,44 Greece, 42 Poland,7,74 Netherlands, 45 Hong Kong, 56 Jordan.47,58 Other studies report similar findings in UNSs.9,18,43,93,94
In their study to determine Turkish nursing students’ knowledge of PC, Polat and Karatas 6 found only, 5%, 26% and 5% correctly answered all questionnaire items, PC theoretical framework and symptom management respectively. These findings are similar to those of Çıtıl et al. 44 who found 52% of the 210 Turkish UMSs they studied had never heard about PC, 64% felt anxious to communicate with the patients and their families, and only about 10% of those who were aware of PC felt the known information was adequate. In the United States, Cleary et al. 29 found UNSs knowledge of PC and EOLC were low at 45% and 47% respectively. In India, Karkada et al. 87 found 80% of students had poor knowledge on PC practices with only 43% being aware of the term PC, with similar findings among pre-final and final-year Indian medicine and nursing students. 53 Very few studies report intermediate knowledge among UNSs and UMSs.54,58,68 In the United States, Pope 41 found 61% of UNSs were knowledgeable about PC, similar to findings reported earlier by Brajtman et al. 23 who found 61% of Canadian UNSs knew about PC.
Alhamdoun et al. 95 identified students had poor knowledge of PC, especially in the symptom management and the definition of PC domains. In Palestine, Harazneh et al. 25 found the overall PC knowledge among third- and fourth-year level UNSs was 41%. With regard to mean knowledge scores on the PCQN questionnaire in UNSs, both narrow and wide variations across countries and regions exist. For example, 10.41 in China, 96 8.20 in Greece, 18 9.04 in China, 25 5.23 in Saudi Arabia. 97 The commonalities in findings in these studies underscore a global problem and an urgent need to address training deficiencies to improve PC knowledge among future physicians and nurses. However, on the other hand, the findings should be interpreted with caution, owing to variability in sample characteristics, curricula and course content, methodologies and outcome measurements.
Theme 2: Undergraduate nursing and medical students’ attitudes, perceptions of and orientation towards PC and EOLC
Subtheme 2.1: Undergraduate students’ attitudes and perceptions towards PC
Unfavourable attitudes ranging from low to high negative attitudes towards PC and EOLC, particularly caring for PC and the dying patients was reported by eight studies conducted with UNSs24,26,39,49,57,66,69,75 compared with only one study conducted with UMSs. 92 A Polish study conducted with both UNSs and UMSs reported similar findings. 7 These unfavourable attitudes have varied manifestation with students experiencing perceived or actual emotional or occupational feelings of distress, fear, helplessness, powerlessness, unpreparedness and uncertainty to handle patients with terminal disease.
However, 11 studies reported favourable attitudes ranging from limited to intermediate positive attitudes towards care for the dying among UNSs5,18,46,48,51,59,61,68,87,88 and UMSs. 58
Hagelin et al. 5 found a majority (67%) of Swedish first-year UNSs had an overall positive attitude towards caring for dying patients. Similarly, Karkada et al. 87 reported higher positive attitude scores towards EOLC among Indian UNSs. Earlier research postulated that nurses’ attitudes towards death might influence their attitudes towards caring for dying patients.98,99
Subtheme 2.2: Students’ orientation towards PC and EOLC
There is a common emergent theme about how students navigate multiple difficulties ranging from basic to complex difficulties in performing tasks such as managing emotional reactions around death and dying, communicating with the dying patient and their family, handling challenging EOL conversations and disease incurability, and providing basic nursing and clinical care to the dying patient.7,44,45,50,55,56,60,62,66,67,69,79,88 Two studies found UNSs and UMSs were unprepared to cope and provide care for children and young people at EOL,56,67 even when they recognised EOLC for children and young people as a sad but important part of the job role. 56
Elsewhere, in Turkey, two studies conducted with UMSs found participants felt unprepared to provide PC and anxious about communicating with patients and families.3,44 Pieters et al. 45 also found 60% of final-year Dutch UMSs at four medical faculties reported they did not feel confident in providing PC, especially addressing spiritual needs/issues (77%) of patients. This finding is corroborated by Leung and Wong 50 in China who found that 60% of UMSs felt they were not confident to provide EOLC. Furthermore, Sweeney et al. 82 in their mixed-methods study assessing UMSs’ Self-Efficacy in PC found only 15% of the Irish students assessed selected PC as their first choice.
Theme 3: Predictors of students’ knowledge, perceptions of and orientation towards PC
Subtheme 3.1 Education and training curricula as a predictor of students’ knowledge
The literature identifies numerous associated factors that have a significant bearing on knowledge of PC and EOLC among students. One of the central themes is inadequate, limited and or/ inconsistent training content about PC and EOLC in nursing and medical curricula, widely cited as a predominant predictor of students’ lack of knowledge or inadequate, awareness, skills, confidence and the competences they need to provide high-quality PC. Surprisingly, this phenomenon is prevalent in resource-rich countries as well, for example, Germany,55,64 Poland, 74 Turkey,3,6,44 Jordan, 39 Australia,40,60 Greece, 42 China,52,57,88 Netherlands, 45 Greece and United Kingdom, 18 Poland, 7 Hong Kong, 56 Saudi Arabia, 97 Jordan, 47 Finland 66 and Palestine. 51
Watts, 61 in their qualitative study of final-year nursing undergraduates’ understandings of PC found that, whereas participants had reasonably broad knowledge of PC (especially scope, compassionate care and emotional support domains), their understanding was superficial.
Conversely, literature shows education and training orientates nurses and medical doctors to the concepts and principles of PC, resulting in improved knowledge and practical competences (skills) necessary for them to provide PC and EOLC. Jiang et al. 9 found nearly all (96%) Chinese UNSs in their study reported additional learning on PC as necessary. Studies conducted with UMSs report similar findings. Argyra et al. 42 found that 60% of Greek students who attended a PC course believed the majority of patients with chronic pain do not receive adequate treatment, while another study conducted in the Netherlands reported students felt several topics were inadequately and superficially covered in the curriculum. 45
Numerous studies conducted with UNSs and UMSs report increased knowledge and improved positive attitudes, perceptions, practices and orientation towards PC and EOLC following education and training. These studies include an interventional repeated measures evaluation study in India, 83 outcome and pre- and post-intervention evaluation studies in the United Kingdom, Poland, Iran, Sweden, Spain, Hong Kong, United States, Indonesia,72,74–78,80,81,85 prospective longitudinal studies in United States,89,90 a descriptive analytical study in Nepal, 92 a qualitative evaluation in Cameroon 62 and Spain, 70 cross-sectional evaluations in Greece, Ireland and Poland,7,42,82 and an intervention comparative study in Turkey. 91
Centeno et al. 73 found that a PC course exposed second to sixth year Spanish UMSs to the concepts and principles of PC, including improved awareness of PC, holistic approaches and self-awareness, positive attitudinal and behavioural change and helped dispel myths and misconceptions, and increased awareness of patient-centred care.
To note, the literature emphasises the importance of problem-based learning (PBL) and simulation-based scenarios in strengthening students’ knowledge and competences to provide PC and EOLC in both UNSs68,70,75,78,80,81 and in UMSs.85,89,90
Education and training as a predictor of students’ perceptions of and orientation towards PC
There is wide evidence in the studies showing that education is an important predictor of positive attitudes towards PC and EOLC among UNSs and UMSs. They include higher and/or better knowledge scores about PC, higher grade or academic level,18,26,46,52 prior training and experiential learning or exposure to PC or death education and clinical practice.5,29,57,58,70,73,75–78,80,81,85,86,89 Reflexive teaching and practice are also cited as important predictors of positive attitudes towards death and dying among UNSs and UMSs. 71
The role of PC and death education in improving positive attitudes, particularly decreasing death avoidance, fear of death and overall death anxiety, and increasing students’ competencies and self-efficacy, including communication skills in the care of the dying patients, is widely supported by experimental studies with both UNSs72,75,76,80,81,84 and UMSs.82,85,89,90 Two recent descriptive qualitative studies in UNSs corroborate the findings.70,71 Similar finding are reported in cross-sectional studies.87,88
Kudubes and Bektas 91 in their study investigating the effect of web-based PPC education on Turkish UNSs knowledge level and practices related to PC found positive correlations especially knowledge increase, self-reported efficacy and PC practices. In a qualitative study exploring the experiences of attending an undergraduate course in PC, Centeno et al. 73 reported Spanish UMSs viewed PC as combined clinical, humanistic and holistic medicine. Through the course, they rediscovered medicine and developed an understanding of the need to be reflective and more humane and compassionate towards patients with PC needs. These findings are consistent with those of Çıtıl et al. 44 who found that 76% of Turkish UMSs emphasised the need for PC education, while 45% wished for PC training at a postgraduate level. A recent qualitative study conducted in the United Kingdom found participants recognised EOLC for children and young people as a sad but important part of the job role. 67
Notably, this review found that there is limited evidence on attitudes towards PC and EOLC among UMSs and UNSs in LMICs, with only one study conducted in Africa. In a Cameroonian qualitative study evaluating the impact of a PC course on nursing students’ practice, Bassah et al. 62 found the course improved the majority of students’ knowledge and competences, especially in the areas of physical care, communication with patients and family, spiritual and psychosocial care.
Inappropriate perceptions and inadequate orientation towards PC and EOLC are prevalent among students, as well as qualified HCPs. Again, the studies attribute this phenomenon to deficient education and training curricula.9,27 In Turkey, Eyigor 3 found 65% of their study participants stated they had received insufficient education on PC, especially pain and symptom control, 90% had received no training on communication skills regarding PC patients, while 34% and 54%, respectively reported opioids use in cancer patients and pain management were inadequate.
However, conflicting findings also exist, for example, in their study of third-year Australian nursing students’ attitudes, experiences, knowledge and education concerning EOLC, Adesina et al. 60 found that whereas students’ confidence, and competence to provide care to dying patients improved with education, as many as 63% indicated they felt inadequately prepared.
Sociodemographic factors
Age, religion/religious beliefs, level of education, gender differences and prior history of working with PC patients are identified in the literature as some of the significant predictors of knowledge of PC among medical and nursing students. These include being older,9,47,54,87,93 history of exposure or training in PC or EOLC education,39,51,52,54,70,73,76,80,81,86 having cared for a dying patient or relative or clinical practice experience39,42,51,52,54,60,64,65,77,89,90 and higher level of education,51,65 school,9,18 being female, 54 religious beliefs and personal background or birthplace 9 and empathy. 59
In their study of 324 Turkish UNSs, Usta et al. 54 found the knowledge scores of PC of older and higher-grade students were higher compared to younger and lower grade students. A combination of mental maturity and life experiences and information absorption accumulated in clinical practice could explain this finding. 18 Similar findings are reported in India 87 and Jordan. 93 In a study of perception of PC among UMSs in Nepal, Pandey et al. 92 found participants’ knowledge of PC increased from 12.5% at the beginning of their medical education to 94% in final year.
Regarding gender, two studies, in Turkey 54 and in China, 9 reported higher knowledge of PC among undergraduate female students than males; Ross et al. 100 reported similar findings among hospice and generalist nurses in the United States. On the contrary in Palestine, Alwawi et al. 51 found male UNSs had significantly better knowledge of PC than their female colleagues.
Regarding students’ perceptions and orientation towards PC and EOLC, predictive factors included being female,18,58 older age (being a ‘mature’ student),26,46 experience of caring for a dying family relative and family atmosphere,9,57 religion or religious beliefs and empathy, 56 previous death work 9 and profession. 7 Dobrowolska et al. 7 found more medical than nursing students predicted more challenges when working with PC patients. Few studies report contrary findings. For example, in China, exposure to death of a family member or friend resulted in reduced confidence to care for the dying among Chinese UMSs, while education and personal experience were found to have a negative correlation with positive attitudes towards EOLC. 59
Some studies found no significant association between sociodemographic factors and students’ perceptions and attitudes and orientation towards PC, including gender and previous experience of caring for PC and dying patients among UNSs24,75 and UMSs. 101
Discussion
This international systematic review aimed to appraise existing research evidence on UNSs and UMSs knowledge, perceptions of and orientation towards PC and EOLC.
The review found insufficient knowledge about PC and EOLC despite training is common to nearly all the studies. Inadequate and inconsistent teaching and training on PC and EOLC, including in communication skills, is cited and/or appears to be the main perpetuating factor for this phenomenon, reported in numerous studies conducted with nursing3,40,93,102–104 and medical students,44,105–107 as well as among qualified graduates.108–110
Other contributing factors include paucity of expertise and role models to effectively teach and mentor students in PC and EOLC.105,106,111 In particular, there is a recurrent theme in the literature about the training being predominantly theoretical and didactic with very limited, or virtually no attention and opportunities for simulated and experiential teaching and learning. Handling challenging conversations is a hardship and dilemmas for student participants in most, nearly all of the studies.19,44,79 Very few studies report students possessed positive attitudes towards caring for palliative and dying patients, particularly in communication and relationship with patients.58,82 These observations highlight major deficiencies in the design or adequacy and delivery of the curriculum and teaching. To foster appropriate attitude and skills development among trainees, the need for urgent reforms in curricula is imperative. In particular, teaching and training should integrate a blend of both theory- and practice-based approaches. The important role of curricula and training that combines simulated, real-world experiences and interactions with palliative and dying patients in improving and consolidating students’ grasp of PC and EOLC concepts, including developing appropriate knowledge, positive attitudes, self-efficacy, communication skills, patient management, emotional and self-awareness and confidence, and patient centredness has been emphasised by numerous studies.39,51,52,64,65,73,78,80,82,89 Watts 61 qualitative evidence revealed that interactive, reflective pedagogical approaches significantly increased nurse students’ confidence, high-order cognitive skills and critical thinking with sound clinical judgement in clinical practice.
Mastroianni et al. 112 found training which integrates both theoretical and practical learning improves students’ knowledge and also their attitudes towards PC, death, dying and EOLC. In a prospective cohort study assessing the effectiveness of a PPC PBL among third-year American UMSs, Moody et al. 90 reported improved knowledge, self-assessed competency and attitudes among the study participants. Findings are consistent with those of other earlier studies which reported PBL methods as effective for teaching PC to students.113–115 In their study in the United States, Morrison et al. 89 found UMSs pain knowledge improved after exposure to patients following an online pain module and reflective essay. A German study found UMSs whose encounters with patients and their caregivers went beyond a review of patients’ medical notes had a better understanding of the holistic approach of PC compared to their colleagues. 64 These results corroborate the findings of numerous other studies.113,116–122 These studies, with their differing methodologies, add to the triangulation of findings. However, the time between the intervention and assessment of outcomes in these studies was predominantly short, which precludes longitudinal assessment of the impact of interventions (training) on outcomes, particularly knowledge, attitudes and confidence. It is also worth noting that the evidence is predominantly skewed towards high resourced settings.
Handling death work, performing tasks related to death and dying is a major challenge for students in this review. The students have negative views and inappropriate attitude towards caring for the seriously ill and the dying. To them, PC is a hard and emotionally demanding job and so they dislike it. Similar findings on fear and avoidance behaviours have been reported in studies elsewhere in UNSs and UMSs98,118,123–127 as well as among practicing health professionals.7,99,104 The low number of studies reporting positive attitudes among UMSs could be explained by limited research on death and dying in UMSs. This begs the question whether curricula and training pay adequate attention to death education. It can be hypothesised that preference rates could even be lower among UMSs and UNSs in many parts of the world, especially in developing countries where barriers such as limited resources, research, training, prohibitive cultural beliefs and practices and limited recognition of the role of EOLC and PC are predominant. This underscores the urgent need for nursing and medical schools the world over to prioritise and strengthen death education but also introduce introductory and refresher training for those in practice.
Despite contradictory results from few studies which found no significant relationship between exposure to death work and attitude and confidence towards EOLC,50,60 several studies emphasise that exposure to death work and prior clinical experience improve students’ confidence and positive attitudes towards care for the dying.59,128–132 These differences in observations could be explained by variations in sociocultural norms, teaching and training, cultures of care, as well as sampling and the methodological designs used. Research suggests appropriate education is a good way to enable students to develop an appropriate understanding of death work including recognition of death as a natural life process.7,88,133–135. Mastroianni et al. 112 argues attitudes towards PC, death and EOLC are psychological and are learned as part of a person’s social and cultural experiences, and as such they can be influenced by education, training and encounters in the clinical settings.
This review has found limited research among key populations such as children and young people47,67,74,90,91 and persons living with dementia. 77 This presents a critical evidence gap and raises the question whether this stems from deficiencies in the curricula or it is just that research is not prioritising these special populations. Furthermore, the wide disproportionate distribution of the research with as many as 56 of the 64 studies (88.5%) located in high-income and upper middle-income countries with just one study in Africa is a worrying observation. Low- and middle-income countries shoulder the greatest unmet need for PC, hence it is imperative there should be research to inform their evidence base. That is to say, research is needed to inform the design of curricula to adequately prepare and empower future nurses and doctors for their job role, including caring for PC and EOLC patients including special or key populations.
Some of the observations in this review are striking. Dobrowolska et al. 7 in their study of predicted difficulties, educational needs and interest in working in EOLC among UNSs and UMSs in Poland found medical students were more interested in curing than in caring. Similar finding was reported by Jeffers and Ferry among nursing students in the United States. 99 The urge and preference to cure could explain a knowledge gap and a lack of understanding of the important holistic, person-centred nature of PC and EOLC. The review has also identified that a students’ interest in PC might be influenced by their profession, for example, Dobrowolska et al. 7 found UNSs demonstrated significantly lower interest in receiving training in PC than their medical colleagues.
Limitations and strengths of this review
This review has a few limitations. First, only four databases were searched for articles published and the articles are all in English. It is hypothesised that some eligible articles published in other databases and languages could have been missed. Nonetheless, the review searched credible and broad databases so it is likely very few articles published elsewhere were missed. Second, owing to heterogeneity in the data due to diverse study designs, methodologies and outcome measures used in the studies, meta-analysis was not feasible, which could potentially limit deeper analysis and understanding of the findings.
However, this review has noteworthy strengths. First, the rigorous literature search, appraisal, syntheses and integration with a clear and detailed audit trail and transparent reporting of results enhance the interpretation as well as clarity, auditability and credibility of the review results. Second, this systematic review integrates data from studies with various methodologies, aiding triangulation of the results. Third, the international nature of the review provides a reasonable generalisable picture of available evidence and evidence gaps on the topic, laying a foundation for future research. For example, the disproportionate concentration of research evidence in high resourced parts of the world identified in this review highlights an urgent need for investment and prioritisation of research to build an evidence base in LMICs. Moreover, the latter shoulder the hugest burden of unmet need for PC globally.
Conclusion
This review found that students’ knowledge levels of PC are predominantly low with rates ranging from 5% to 61% across different regions of the world, including in HMICs regions like the United States, Canada, Europe and Asia.
Similarly, nursing and medical students’ perceptions and orientation towards PC are rated with scores ranging from poor to low in most of the studies with participants manifesting low self-efficacy in providing PC and EOLC, that is, unpreparedness, unwillingness and incompetence in areas such as pain and symptom management, and communication skills, particularly in handling challenging conversations with patients and families.
There is a dearth of documented research from Africa on the topic with only one study identified in this review. The little research that exists is concentrated in HICs and MICs. There is need for more research studies with emphasis on LMICs, including studies which use interventional, longitudinal, evaluation and qualitative designs. Qualitative research (grounded theory) should examine how sociocultural variables, such as religion and gender, influence students’ knowledge, attitudes and orientation towards PC and EOLC.
Inadequate, limited and/or inconsistent curricula and training content about PC and EOLC is a common theme in the literature, including in studies undertaken in upper MICs and in HICs. There is need for regular review of curricula to ascertain their adequacy in meeting learners’ training needs.
Furthermore, more emphasis is needed on death education, including handling challenging or conversations to orientate and empower future doctors and nurses to be able to do death work rather than shunning it. There is need for educational institutions and other stakeholders to ensure those who teach PC receive appropriate and adequate training to empower them also. The mode of instruction should be more comprehensive, integrating various pedagogical approaches such as simulation and PBL as well as practical, case studies and field attachments in cancer, palliative and hospice care settings. The latter will allow trainees to gain exposure and experience learning in a real-world environment rather than relying on theoretical teaching and knowledge.
Supplemental Material
sj-docx-1-pcr-10.1177_26323524261433191 – Supplemental material for Palliative and end-of-life care from an education lens. An international systematic review of undergraduate medical and nursing students’ knowledge, perceptions, and orientation towards palliative and end-of-life care
Supplemental material, sj-docx-1-pcr-10.1177_26323524261433191 for Palliative and end-of-life care from an education lens. An international systematic review of undergraduate medical and nursing students’ knowledge, perceptions, and orientation towards palliative and end-of-life care by Germanus Natuhwera, Peter Ellis and Eve Namisango in Palliative Care and Social Practice
Footnotes
Acknowledgements
The authors wish to acknowledge the participants and researchers whose information and research informed this review.
Ethical considerations
As this was a review of published research, no prior ethical approval was required. However, to note, the review was part of a larger multi-institution mixed-methods study examining UNSs’ and UMSs’ knowledge and perception of and orientation towards PC in Uganda which was reviewed for ethical conformance by Hospice Africa Uganda Research Ethics Committee (HAUREC). Ethical approval was granted on 20th September 2022, protocol number HAU-2022-03-A. In addition, the study received administrative clearance by Makerere University School of Medicine Research Ethics Committee (SOMREC) on 28th October 2022. Each of the articles included in this review had a clear ethics statement indicating the name of a credible research ethics committee or body that reviewed the study protocol and granted ethical approval, the reference number of the approval letter, and that written informed consent had been obtained from study participants.
Author contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
All data generated in this systematic review are included in this article and its supporting information files.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.