
Abstract
Introduction:
About a decade after the introduction of palliative care teaching for undergraduate nurses and medical students in Uganda, no research has examined students’ knowledge and self-efficacy to provide palliative and end-of-life care and their correlates.
Aims:
To: (1) estimate final-year undergraduate nursing and medical students’ knowledge of and self-efficacy to provide palliative and end-of-life care, (2) identify correlates of knowledge and self-efficacy to provide palliative and end-of-life care.
Design:
A multicentre cross-sectional quantitative study.
Setting/participants:
Final-year undergraduate medical and nursing students in eight medical and nursing schools in Uganda. Instruments included biodata sheet, the Palliative Care Quiz for Nursing questionnaire and the Palliative Care Self-Efficacy scale. Statistical analyses were performed using STATA version 14.0.
Results:
The mean age of the participants (n = 466) was 24.45 ± 3.31 years. Participants’ knowledge of palliative care scores was low in all domains ‘Philosophy and principles of palliative care’ 1.46 ± 0.93 (range: 0–4), ‘Psychosocial and spiritual care’ 0.61 ± 0.73 (range: 0–3) and ‘Management of pain and other symptoms’ 6.32 ± 1.75 (range: 0–13). Predictors of knowledge were Gender (p = 0.0242), course of study (p = 0.0001) and religion (p = 0.0338). Participants had very low self-efficacy scores in the three domains of the Palliative Care Self-Efficacy scale.
Conclusion:
Participants generally demonstrated limited knowledge and insufficient self-efficacy in providing palliative and end-of-life care. There is a need to integrate and strengthen practical, pedagogical and experiential teaching, review the palliative care curriculum. Future evaluative, longitudinal and interventional as well as qualitative studies are needed to gain deeper insights into this topic.
Background
Over recent decades, the demand for palliative care (PC) has risen significantly in line with a rise in the global disease burden (both communicable and non-communicable) and an ageing population.1 –3 High-quality palliative and end-of-life care are now well recognized as an indispensable human right to dignity. 3 The unmet need for palliative care services is still, however, huge, particularly in low-and-middle-income countries where at least 76% of adults require palliative care.4 –6
Yet, globally, only 14%, of about 53 million adults and 4 million children, who need palliative care receive it. 5 Furthermore, at least 25.7 million adults and 2.5 million children, including at least 80% of adults and 98% of children residing in low-and-middle-income countries, experience serious health-related suffering at the end of life.5,7 The need for palliative care at the end of life is projected to double by 2060. 4
In Africa, disparities in access to palliative care are vast, with an estimated 5% of those in need able to access services. 8 Cancer cases are rising exponentially and are projected to rise by 400% by the year 2050. 9 It is estimated that in the World Health Organization Africa region, 2000 adults (⩾18 years) per 100,000 of the population and 369 children (0–17 years) per 100,000 of the population require palliative care. 5
In Uganda an estimated minimum of 400,000 adults and 86,000 children need palliative care every year. 10 Furthermore, an estimated 84% and 80% of adult and children cancer patients respectively require palliative care (pain relief) as an integral component of their cancer care. 7 But only 11% of Ugandans in need of palliative care can access services.5,11
This phenomenon highlights an urgent need for a correspondingly significant increase in the availability of palliative care services. 12 Integrating education and training in palliative care and care for the dying (end-of-life care) within undergraduate health curricula is critical in preparing future nurses and medical doctors to provide high-quality palliative and end-of-life care.5,6,13,14
Education has the potential to improve students’ knowledge and promote positive attitudes towards palliative and end-of-life care.15 –20 Exposure to palliative and end-of-life training has been shown to improve nursing and medical students’ knowledge, skills, self-confidence, self-awareness and competence to provide holistic and person-centred care.21 –24 Numerous evaluation and interventional studies from high-income countries have corroborated that palliative care training orientates and improves students’ knowledge and attitudes towards palliative care.25 –29
A wealth of research evidence indicates nursing and medical students continue to graduate from training institutions possessing gross negative perceptions and being unprepared to provide culturally sensitive and person-centred palliative and end-of-life care.30 –33 This unpreparedness usually manifests as inappropriate attitudes and insufficient or lacking knowledge, skills and confidence in essential domains such as principles of palliative care, pain and symptom management, provision of psychosocial and spiritual care, and communication with dying patients and their families.34 –40 Very limited research has found good knowledge of palliative among undergraduates. 41 Inadequate curricula, education and training have been cited as a major predictor for this common observation.42,43
Around a decade since the introduction of palliative care teaching into the nursing, allied health and medical training curricula in Uganda, it remains unclear as to what extent, if at all, it is positively influencing nursing and medical students’ knowledge and self-efficacy to provide palliative and end-of-life care or what characteristics of students are predictive of this. In the context of this study, self-efficacy is defined as students’ ability to develop the appropriate attitude, skills and self-confidence necessary to apply learned knowledge to provide palliative and end-of-life care.
Furthermore, there is a dearth of documented research on the topic from Africa. In particular, no documented research on the topic was identified at the time of this study. A global systematic review conducted prior to this study revealed that nursing and medical students continue to graduate from training schools with low and inadequate knowledge of palliative and end-of-life care, ranging from 5.3% to 61%. Students’ knowledge levels of palliative care are predominantly low with rates ranging from 5.3% to 61% across different regions of the World. Anecdotal observations in practice point to deficient levels of knowledge, negative perceptions and a lack of competence among students and qualified healthcare professionals.
Hence, this study sought to examine this under-researched topic. The evidence generated could reveal training needs and gaps in the scope and delivery of palliative care training, and suggest appropriate remedial action, including future research to optimize the impact of the course on students’ training needs.
Aims of the study
The study aimed to
1. Estimate final-year undergraduate nursing and medical students’ knowledge of palliative and end-of-life care.
2. Examine participants’ self-efficacy to provide palliative and end-of-life care.
3. Examine the correlation between knowledge and self-efficacy, knowledge and socio-demographic and professional variables (independent variables).
Methods
Study design, population and context
This cross-sectional quantitative study was part of a larger multicentre parallel mixed-methods study of final-year undergraduate medical and nursing students in eight public and private tertiary education institutions in Uganda. The qualitative element of the study (preprint) is being considered for publication elsewhere. 44 The purpose of recruiting participants from different settings was to generate generalisability.
In Uganda, undergraduate medical students undergo training for 6 years including 1 year of clinical internship before they qualify to be awarded a Bachelor of Medicine and Bachelor of Surgery. Nursing students pursuing a Bachelor of Science in Nursing complete four years of training and an additional 1 year of internship in a clinical setting under supervision. Diploma-level participants were nursing and midwifery students in their final semester of a 2-year extension programme after initially attaining a 2.5-year certificate and practiced for at least 2 years. Regarding the palliative care course unit, based on the design of the curriculum, the course is allocated a whole semester and is taught in-; fourth year for undergraduate medical students, third year for undergraduate degree and diploma direct nursing students, second year for undergraduate diploma nursing students on extension and certificate level nursing students.
Sampling and sample size estimation
The sample size was estimated using Cochran’s formula for unknown population 45 as n = 384. To increase the power of the study, an additional 38 participants, 10% was included to cater for 10% non-response rate, so total n = 422.
Data collection methods and instruments
Data collection took place between 21November 2022 and 1 March 2023. Participants were accessed through their respective department within which the students are registered after securing institutional approval. A biographic data sheet including age, gender, discipline of study (nursing or medical), history of training in palliative care and or working with palliative care patients was used to collect participants’ biographic data.
Students’ knowledge of palliative care was assessed using the Palliative Care Quiz for Nursing questionnaire. According to Ross et al., 46 the scale has a high internal content validity and acceptable reliability (test–re-test = 0.56 and Kuder–Richardson 20 = 0.78). The questionnaire is self-administered and consists of 20 multiple-choice items (true/false/does not know/did not answer) to assess three main domains of palliative care: philosophy and principles of palliative care (4 items), control of pain and other symptoms (13 items) and psychosocial aspects of palliative care (3 items). These 20 items refer to knowledge applicable in clinical settings.
The questionnaire has been proven to be a valid and reliable tool (with adequate internal consistency in different languages) for assessing knowledge and identifying perceptions of palliative care among health professionals in both developed settings, for example, China 47 and developing countries, for example, Ethiopia. 48 Originally developed to assess knowledge in nursing, the questionnaire has further been proven to be an effective tool to assess knowledge of palliative care in other health cadres including active medical doctors and students. 49
Students’ self-perceived efficacy was assessed using the Palliative Care Self-Efficacy scale, a validated 23-item self-assessment structured questionnaire that seeks to examine how clinicians/nurses manage various situations in a palliative care environment, for example, confidence in communicating with the dying, managing symptoms, etc. 50
The scale has three distinct subscales covering palliative care domains: Communication Skills; Multidisciplinary Teams; and Pain and Symptom Management. Possible responses are rated on a Likert scale ranging from 1 to 4 with a score of 1 denoting ‘need further basic instruction’, a 2 denotes ‘confident to perform with close supervision/coaching’, a 3 suggests ‘confident to perform with minimal consultation’ and a 4 denotes ‘confident to perform independently’. The entire scale has a strong validity, as demonstrated by a Cronbach’s alpha coefficient of 0.92, and 0.87 and 0.91 for the subscales ‘perceived capability to answer end-of-life care concerns of patients’ and ‘perceived capability to respond to patients’ end-of-life symptoms’, respectively. 50 Data were collected face-to-face by GN and research assistants who were trained and oriented by GN prior to commencing data collection.
Sampling and recruitment
Convenience sampling was employed to recruit participants who were readily accessible and willing to participate in the study. A total of 466 participants from eight teaching institutions volunteered to participate (Figure 1). Convenience sampling was preferred as the researcher could not get the sampling frame to fulfill the criteria for random sampling given the nature of the settings of the participants.

Participants’ recruitment scheme.
Eligible participants were: (i) nursing or medical students in the final year of their undergraduate training; (ii) Ugandans (to increase sample homogeneity and minimize possible skewed data variations due to cultural or contextual differences); (iii) able to grant their individual voluntary consent verbally and by signature; (iv) able to talk, read and write in English.
A prospective participant was excluded if they: (i) were non-finalist; (ii) non-Ugandan/international students to minimize confounders related to home country factors such as prior experiential training or exposure to palliative care; (iii) declined to give their consent; (iv) were unable to hear, read and or write in English; (v) chose to opt out of the study.
Data handling and analysis
Completed questionnaires were screened manually for completeness and the data entered into a coded Microsoft Excel spreadsheet. The generated datasets were then exported into STATA version 14.0, StataCorp LP, College Station for analysis.
Participants’ demographic characteristics and knowledge scores on the Palliative Care Quiz for Nursing scale were summarized using descriptive statistics, mainly frequencies, percentages, minimum and maximum (range), means and standard deviations. ‘True’ responses were scored as one, and ‘False’ or ‘I don’t know’ responses scored as zero. For each questionnaire, the total score was computed by summing up the number of correctly answered items, with range of 0 (minimum score) to 20 (maximum score). The mean scores of each of the Palliative Care Quiz for Nursing items were computed by summing up the scores in the subscale and dividing the total score by the number of items. Hence, philosophy and principles had a theoretical score range (minimum–maximum) of 0–4, pain and symptom had a score range of 0–13, and psychosocial and spiritual care had a score range of 0–3.
Analysis of variance (ANOVA) and Bartlett’s equal-variances tests were performed to examine relationships between students’ palliative care knowledge scores on the Palliative Care Quiz for Nursing subscale and independent variables within and between groups. Weighted regression analysis was performed to further examine relationships between predictor variables (age, gender and course of study) and students’ palliative care knowledge scores. Results were interpreted as odds ratios.
Descriptive statistics (proportions and percentages) were used to summarize students’ responses on the Palliative Care Self-Efficacy scale. ANOVA and Bartlett’s equal-variances tests were performed to examine the relationship between students’ self-efficacy scores and predictor variables. The scores for each completed questionnaire were summed up to get the total score. The lowest and highest possible scores for each questionnaire were 23 and 92, respectively.
A value of p < 0.05 was considered statistically significant for all the statistical tests. All study datasets are stored on GN’s computer secured with a password.
Results
Four hundred sixty-six students completed the questionnaire compared with an estimated sample size of 422, translating to a response rate of 110%.
As seen in Table 1, of the 466 students that participated in the study, 253 (54.3%) were female and the majority were in the age range of 20–29 years 428 (91.9%). Their mean age was 24.45 ± 3.31 years and the age range was 20–44 years.
Socio-demographics of participants (n = 466).
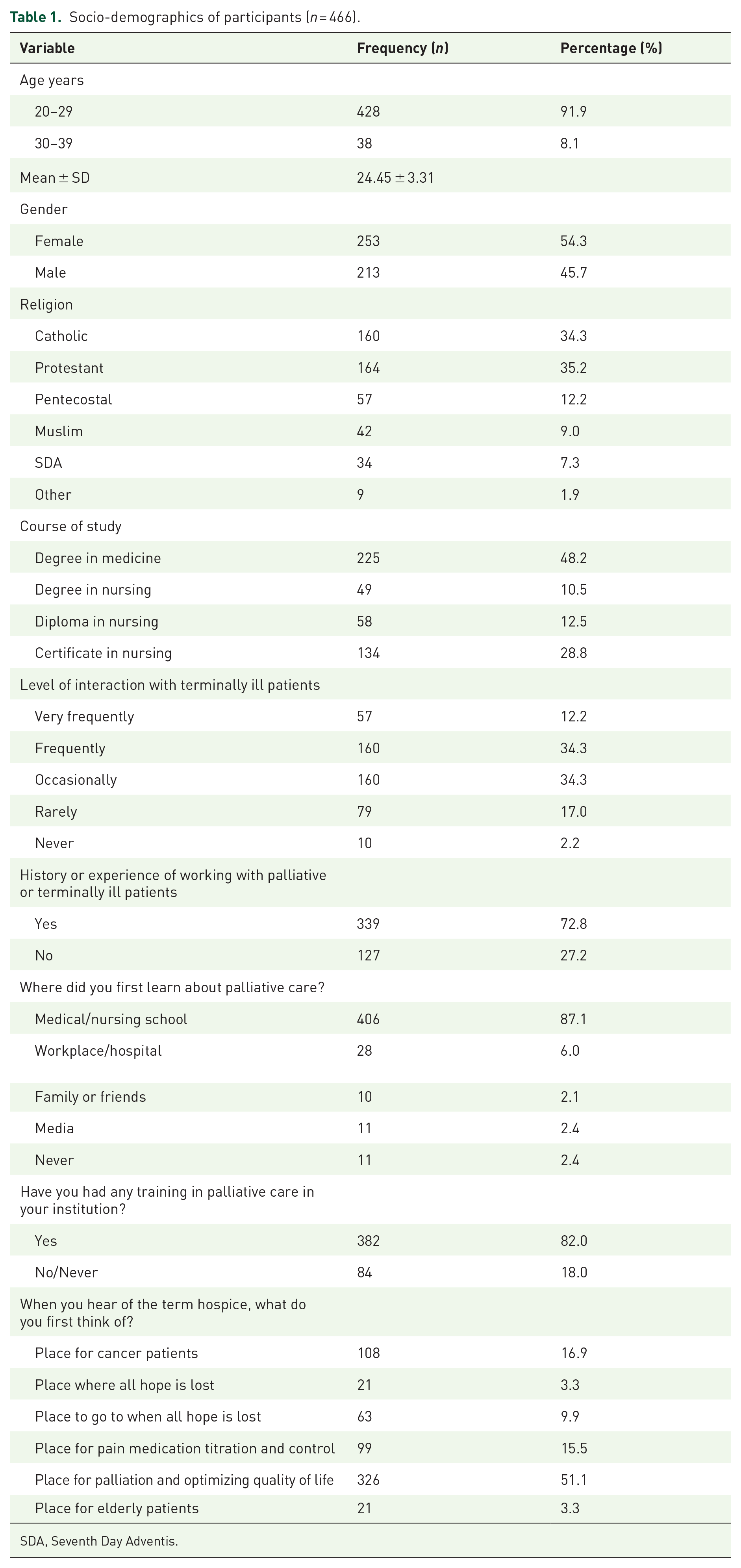
SDA, Seventh Day Adventis.
As can be seen in Table 2, a higher frequency of correct responses was observed in the ‘management of pain and other symptoms’ subscale especially questions 2, 4, 8 and 18. However, the rest of the 10-scale items had below-average (50%) number of correct responses.
Frequency and percentage of responses of participants on the Palliative Care Quiz for Nursing scale (n = 466).

Scoring: True (T) is a correct response (T) = 1 score, False (F) and ‘I don’t know’ (I) are incorrect responses and each = 0 score.
PCQN, Palliative Care Quiz for Nursing.
The least correctly answered scale items questions 3, 7 and 13 refer to pain management and the use of opioids.
In the ‘philosophy and principles of palliative care’ subscale, a low number of correct and a higher number of incorrect/unsure responses was observed. Notably, the number of correct responses for all four scale question items was below average (50%).
The ‘psychosocial and spiritual care’ subscale recorded the least number of correct responses. Of the three question items in the subscale, the highest number of correct responses were observed in Q11 (31.6%).
Participants’ knowledge of palliative care was generally poor. Good knowledge scores were observed in only four subscales (Q2, Q4, Q8, Q18) in the ‘management of pain and other symptoms’ category, with overall mean knowledge scores (6.32 ± 1.75). The rest of the subscales had knowledge scores below 50% (see Table 3).
Overall minimum and maximum, means, and mean knowledge scores of participants on the three conceptual categories of the PCQN scale.

PCQN, Palliative Care Quiz for Nursing.
In Table 4, in the ‘philosophy and principles of palliative care’ subscale, ANOVA show a statistically significant relationship for gender (F = 5.12, p = 0.0242) with males showing higher knowledge scores, and course of study (F = 7.68, p = 0.0001), with medical and diploma in nursing students having better knowledge than certificate and degree nursing colleagues. Bartlett’s test shows the mean knowledge score variances within and between groups are equal for age (F = 2.01, p = 0.072), gender (F =5.12, p = 0.217), religion (F = 2.10, p = 0.675) and course of study (p = 0.301).
Comparison of palliative care knowledge scores of the students according to the Palliative Care Quiz for Nursing with their socio-demographic characteristics (n = 466).

ANOVA, analysis of variance; df, degrees of freedom; F, statistic; p, probability value; PCQN, Palliative Care Quiz for Nursing; SD, standard deviation of the sample; x¯, mean knowledge score of the sample; χ2, Bartlett’s Chi-square test statistic.
In the ‘management of pain and other symptoms’ subscale, religion was statistically significant (F = 5, p = 0.0338). Muslims and Pentecostals demonstrated higher knowledge scores than Protestants and Catholics. Bartlett’s equal-variances test further shows that the mean variances within and between groups are significantly unequal (p = 0.040).
In the ‘psychosocial and spiritual care’ subscale, the course of study shows a statistically significant positive association with knowledge of palliative care (F = 3.06, p = 0.0279). Notably, medical students had higher scores and diploma in nursing students had the lowest scores.
In Table 5, in model one, philosophy and principles of palliative care, the odds of having knowledge of PC was 30% lower if the participant offered a certificate in the nursing course (p = 0.001) OR 0.7008269 (95% CI: 0.5805999–0.8459498). Older students (30–39 years) were 32% (p = 0.050) OR 1.3226 (95% CI: 0.9995–1.7499) more likely to have better knowledge of PC compared with younger students (20–29 years). Being male was 14% (p = 0.101) OR 1.1386 (95% CI: 0.9759–1.3296) more likely to have better knowledge of PC compared with being female.
Weighted logistic regression analysis to test correlations between students’ knowledge of palliative care and independent/predictor variables.

Variables marked with an asterisk (*) represent the reference group.
In model two, management of pain and symptoms, being older, male, and taking on courses other than degree in medicine was associated with reduced odds of having knowledge of palliative care.
In model three, ‘psychosocial and spiritual care’, the odds of having knowledge of palliative care was lower by 26% (p = 0.037; 95% CI: 0.5531–0.9819) if the student was on a degree in the nursing course compared with if they were on a degree in medicine. The odds of having knowledge of palliative care was 21% lower (p = 0.028) OR 0.7924 (95% CI: 0.6437–0.9755) if the student was doing a certificate in nursing course compared with if they were doing a degree in medicine course.
In Table 6, results indicate that participants had the lowest self-efficacy scores in all the eight items in the communication subscale with items regarding discussing death and dying, discussing impending death with the patient and with the patient’s family, bereavement, and answering the patient question ‘how long have I got to live?’ registering very low scores.
Participants’ Palliative Care Self-Efficacy scale results.

Scoring: Need further basic instruction = 1, Confident to perform with close supervision / coaching = 2, Confident to perform with minimal consultation = 3, Confident to perform independently = 4.
Somewhat better but low self-efficacy scores were observed in the patient management subscale. Notably, participants demonstrated low self-efficacy scores in their ability to prescribe appropriate and adequate pain control medication and provision of psychosocial care for the patient and their family. Similarly, results showed participants had low self-efficacy to provide palliative care in all the seven items in the multidisciplinary teamwork subscale. Participants scored the lowest scores in the ‘referring palliative care patients for complementary therapies and to a lympheodema service’ subscale items.
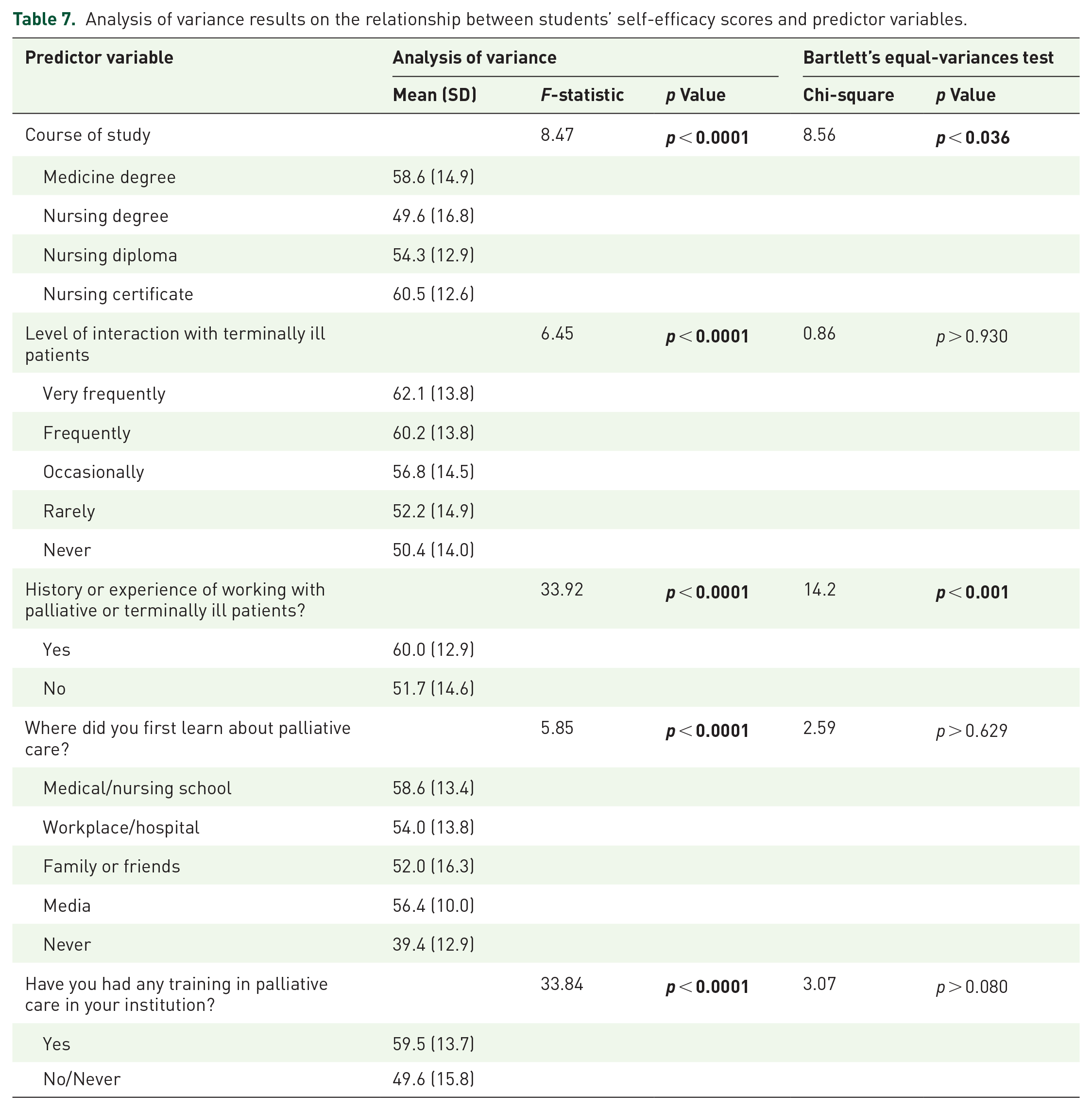
In Table 7, ANOVA was performed to investigate the relationship between students’ self-efficacy scores and selected predictor variables. The course of study (p < 0.0001), level of interaction with terminally ill patients (p < 0.0001), history of working with terminally ill patients (p < 0.0001), an environment where one first learned about palliative care (p < 0.0001) and history of training in palliative care (p < 0.0001) all showed statistically significant relationships with students’ self-efficacy scores. Bartlett’s equal-variances test showed statistically significant results in only two variables; course of study (p < 0.036) and history or experience of working with palliative or terminally ill patients (p < 0.001). Certificate-level nursing participants had better self-efficacy scores than their diploma and degree in nursing and medicine counterparts.
Analysis of variance results on the relationship between students’ self-efficacy scores and predictor variables.
Discussion
The main aim of this study was to examine final-year undergraduate nursing and medical students’ knowledge and perceptions of, and orientation toward, palliative care. The study found participants had low knowledge of palliative care with correct response scores ranging between 11.0% and 49.8% in all but 3 of the 20 items of the Palliative Care Quiz for Nursing questionnaire.
Regarding participants’ demographics, statistically significant predictors of knowledge of palliative care were found to be gender (p = 0.0242) and course of study (p = 0.0001) in the ‘philosophy and principles of palliative care’ subscale. Males and degrees in medicine and diplomas in nursing students showed higher knowledge scores of palliative care than their certificate and degree in nursing colleagues. Notably, Escribano et al. 51 found that females had better knowledge of and self-efficacy to provide end-of-life care than their male counterparts.
Previous studies conducted in high-income countries found that females had higher knowledge of palliative care than their male counterparts.52 –54 In the management of pain and other symptoms subscale, religion (p = 0.0338) was statistically significant with Muslims and Pentecostals having higher knowledge scores than Protestants and Catholics. Similarly, in the Psychosocial and Spiritual Care subscale, the course of study was significant (p = 0.0279) with medical and diploma nursing students having higher knowledge scores. This latter observation could be linked to prior exposure to the clinical setting given that most of the diploma nursing students are already qualified certificate-level nurses. Clinical exposure and higher level of education have been reported as predictors of knowledge of palliative and end-of-life care among nursing and medical students in previous studies.19,37,42,54 –56
The low and insufficient knowledge of medical students observed in this study is documented in research conducted elsewhere among undergraduate nursing and medical students in high-income countries.53,54,57,58 This study found no association between age and students’ knowledge of palliative care, contrary to a wide body of evidence from previous research.35,52,54,59,60
All the students in this study demonstrated low to poor understanding of palliative care concepts with the lowest mean knowledge scores in the philosophy and principles of palliative care (1.46 ± 0.93) and psychosocial and spiritual care (0.61 ± 0.73) subscales, while generally, students had better knowledge scores in the management of pain and other symptoms subscale (6.32 ± 1.75). This could be due to the predominant disconnect between theory and practice. To note, in the qualitative findings of the study, 44 students blamed the training which they said is mainly theory (classroom) based with virtually no or very limited opportunities for them to experience learning in a real-life clinical setting. Similar findings of inadequate to poor knowledge of palliative care among nursing students are reported in previous studies in both middle-income and high-income and countries37,61 –66 and medical students in high-income countries.35,41,67 –71 This underlines a global need for concerted action strengthening palliative and end-of-life training.
Regarding perceptions and self-efficacy to provide palliative care, the results of the Palliative Care Self-Efficacy scale found student participants scored low in nearly all the scale items. This could be linked to, and stemming, from deficiencies in training in the classroom; notably training that is predominantly theoretical when numerous evaluation and intervention studies, all in high-income countries, have demonstrated that palliative care training integrating problem-based learning improved students’ knowledge, attitudes and skills.26 –29
Low self-efficacy to provide palliative care to patients and families with life-limiting illnesses has been widely reported in studies with medical and nursing graduates.22,33,40,57,64,66,68,72,73 Numerous studies corroborate that this is due to inadequate training about palliative and end-of-life care which has been widely reported in nursing,37,53,56,74 –76 medicine,77 –79 and high-income countries.27,67,69,80 –82 Intervention and evaluation studies have shown how education and training increase knowledge of, and confidence to provide palliative and end-of-life care.26,28,55,83,84 Surprisingly, certificate-level nursing students showed higher self-efficacy scores compared to diploma and degree nursing and degree medicine students. Hypothetically, it may be that the former has more clinical exposure (hands-on) than the latter. In their study in Portugal, Martins et al. 85 found that self-efficacy was the variable that had the most significant impact on qualified nurses’ and doctors’ ability to provide end-of-life care.
Notably, all participants scored the lowest scores in all three elements of the Psychosocial and Spiritual Care subscale and Palliative Care Self-Efficacy scale, particularly handling death work, that is, discussions around death, dying and bereavement, further underlining the training gap. This finding is consistent with previous studies conducted with qualified health professionals.36,86 However, some studies conducted found that qualified health professionals were moderately prepared and qualified to provide end-of-life care.85,87,88 Previous research has demonstrated adequate education and training improve students’ capacity to handle death work.54,66,89 In fact, adequate education and training were found to reduce emotional distress, death avoidance and anxiety related to death and dying in nursing students,57,90 and among medical students.27,29,91,92 Adesina et al. 42 in their study reported a negative correlation between training and students’ knowledge of, and confidence and competence to provide end-of-life care.
Strengths and limitations of the study
The study has some salient strengths. First, this is one of the first studies to examine knowledge of and self-efficacy to provide palliative and end-of-life care and their correlates among undergraduate nursing and medical students in Uganda. Second, the multicentre nature of the study, with participants from different courses makes the findings more generalizable. Third, validated measurements were used to collect data, this adds to the reliability, dependability and validity of the study findings. Fourth, although the study employed non-probability convenience sampling, a large sample size of 466 increased the statistical power of convenience data, and so minimization of type II error.
The study has a few limitations. First, the cross-sectional and multicentre design could potentially be associated with contextual differences such as variations in course content and scope which may to some extent, contribute to differences in students’ knowledge and perceptions of and orientation towards PC. Yet, this study may not be able to adequately explain such contextual and causal differences and relationships.
Second, this is a one-point inquiry, hence, it is not possible to give clear accounts for some salient observations and causal trends. For example, the influence of religion and other important tenets of culture on students’ knowledge, perceptions and orientation towards PC, and also the extent to which the curriculum contributes to the study findings. Hence, limited ability to control confounders.
Third, the study was conducted in only eight teaching institutions, hence, the findings may not be wholly generalizable or a true representative and reflection of the reality in other non-participating institutions.
Fourth, the authors acknowledge the inadequacy of question items to assess students’ knowledge of ‘spiritual care’ aspect in the ‘psychosocial and spiritual care domain of the PCQN scale’, though the aspect was further adequately explored in the qualitative part.
Conclusions and recommendations
The study findings highlight participants generally had low and inadequate knowledge of and low self-efficacy to provide palliative care, underlining deficiencies in training and perhaps curricula. There is an urgent need to integrate and strengthen practical, pedagogical and experiential teaching to foster skills development but also to allow for translation of knowledge into practice. In particular, students should be placed, or rotated through clinical settings including hospices, cancer centres and wards that look after patients with palliative care need for them to experience learning in a real-life setting.
The study found participants had serious low self-efficacy or self-confidence, most notably in handling death work or end-of-life care. Teaching and training should urgently address existing gaps in death work, including difficult conversations around death and dying. Importantly, there is a need to review the palliative care curriculum to establish its adequacy in meeting the training needs of students.
Evaluative, more robust qualitative study designs, for example, grounded theory and ethnography and longitudinal studies are needed to further examine how culture and the palliative care course and mode of delivery orientate and impact students’ knowledge and perceptions of palliative and end-of-life care.
Supplemental Material
sj-docx-1-pcr-10.1177_26323524251316901 – Supplemental material for Knowledge, Self-Efficacy, and Correlates in Palliative and End-of-Life Care: Quantitative Insights from Final-Year Nursing and Medical Students in a Mixed-Methods Study
Supplemental material, sj-docx-1-pcr-10.1177_26323524251316901 for Knowledge, Self-Efficacy, and Correlates in Palliative and End-of-Life Care: Quantitative Insights from Final-Year Nursing and Medical Students in a Mixed-Methods Study by Germanus Natuhwera, Eve Namisango and Peter Ellis in Palliative Care and Social Practice
Supplemental Material
sj-docx-2-pcr-10.1177_26323524251316901 – Supplemental material for Knowledge, Self-Efficacy, and Correlates in Palliative and End-of-Life Care: Quantitative Insights from Final-Year Nursing and Medical Students in a Mixed-Methods Study
Supplemental material, sj-docx-2-pcr-10.1177_26323524251316901 for Knowledge, Self-Efficacy, and Correlates in Palliative and End-of-Life Care: Quantitative Insights from Final-Year Nursing and Medical Students in a Mixed-Methods Study by Germanus Natuhwera, Eve Namisango and Peter Ellis in Palliative Care and Social Practice
Supplemental Material
sj-docx-3-pcr-10.1177_26323524251316901 – Supplemental material for Knowledge, Self-Efficacy, and Correlates in Palliative and End-of-Life Care: Quantitative Insights from Final-Year Nursing and Medical Students in a Mixed-Methods Study
Supplemental material, sj-docx-3-pcr-10.1177_26323524251316901 for Knowledge, Self-Efficacy, and Correlates in Palliative and End-of-Life Care: Quantitative Insights from Final-Year Nursing and Medical Students in a Mixed-Methods Study by Germanus Natuhwera, Eve Namisango and Peter Ellis in Palliative Care and Social Practice
Footnotes
Acknowledgements
The authors thank the following individuals who supported data collection for this research. Mr. Kintu Herbert, Mulago School of Nursing and Midwifery, Kampala, Uganda. Dr. Rogers Abaho, Kampala International University and Medical Officer, Bushenyi District Local Government, Bushenyi, Uganda. Dr. Victor Niwamanyire, Makerere University College of Health Sciences, Kampala, Uganda. Dr. Kibet Emmanuel, Mbarara University of Science and Technology, Mbarara, Uganda. Dr. Robert Alinda, Uganda Christian University and Mulago National Referral Hospital, Kampala, Uganda. Ms. Mercy Akoragye, Student Midwife, Mayanja Training Institute, Mbarara, Uganda.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.