
Abstract
Background:
There is evidence that early admission to the palliative care (PC) program in adult cancer patients improves symptoms management, reduces unplanned hospital admissions, minimizes aggressive cancer treatments, and enables patients to make decisions about their end-of-life (EOL) care.
Objectives:
This retrospective cohort study aimed to determine whether late admission to a PC program is associated with aggressive treatment at the EOL in adult patients with oncological diseases from their admission until death.
Design/Methods:
The study evaluated the aggressiveness in EOL management in patients with advanced stage oncological diseases who died between 2017 and 2019. The study population was divided into two groups based on the time of admission to the PC program. Aggressiveness at the EOL was measured using five criteria: treatment, hospital admission and duration, emergency department care, and/or intensive care unit utilization.
Results:
The study found a significant difference in the rate of aggressive EOL treatments between late admission to PC care and early admission [adjusted EOL 79.6% versus 70.4%; relative risk (RR): 1.98, 90% CI: 1.08–3.59, p: 0.061]; In the analysis of secondary variables, a significant association was observed between early admission to PC and the suspension of active treatments at the EOL, leading to a decrease in aggressiveness (77% versus 55.8%; RR: 1.38, 95% CI: 1.14–1.67, p: 0.004).
Conclusion:
Our findings suggest that early referral to PC services is associated with less aggressive treatment at the EOL, including suspension of active treatments.
Introduction
One of the crucial healthcare objectives for patients with advanced cancer is the timely referral to interdisciplinary palliative care (PC) teams. These teams provide comprehensive hospital and outpatient care throughout the disease trajectory, including after death.1 –3 The primary focus of PC is to enhance the quality of life, alleviate symptoms, and offer psychological and social support to both the patients and their families throughout the disease journey.4,5
In Latin America, despite some efforts made in certain countries, access to PC remains limited for the majority of the population. 6 In Colombia, although being pioneers in PC since the 1980s, three out of ten people still die without receiving the necessary PC services. Annually, approximately 250,000 adults require PC, and many regions have minimal coverage (0–0.2 services per 100,000 inhabitants).7,8 This situation creates national deficit in service availability, with centralized care and inadequate coverage in peripheral areas. It continues to pose a challenge for the implementation of PC services that could enhance the quality of life for patients in need. This lack of accessibility may be attributed to healthcare professionals’ limited awareness or healthcare system limitations, leading to prolonged suffering, aggressive end-of-life (EOL) treatment, and dysthanasic processes due to institutional protocols or therapeutic futility.9,10
Multiple international organizations have adopted and advocated for a significant guideline: all patients receiving oncological management should receive early PC.1,11 –13 However, few studies indicate optimal timing for referral to achieve a substantial impact on reducing aggressive EOL treatment and improving quality of life. Unfortunately, late referral are commonly observed, which limits the opportunity to alleviate refractory symptoms, engage in shared decision-making, establish advance directives, and provide health education regarding of EOL care. Consequently, the benefits of PC are often limited or absent.5,14 –18
The aim of this study was to evaluate the time between PC admission and death and assess whether late referral to a PC program is associated with treatment aggressiveness in EOL care in adult patients with oncologic disease.
Methodology/Design
This retrospective cohort study was conducted at Clínica de Occidente S.A., a hospital located in the city of Cali, Colombia. The primary outcome of this study was to compare the association between early and late admission to PC program. The cut-off interval of 3 months for defining early and late admission was based on the study by Hui et al., 19 which demonstrated similar results when using cut-off points of 1 or 2 months.
The impact on aggressiveness in EOL management was assessed by the relationship between indicators of aggressive care at the EOL. To measure this, we utilized a composite indicator called ‘adjusted EOL aggressiveness (mean SD)’, which was adapted from the study by Earle et al. 20 This composite indicator consists of five criteria: use of chemotherapy within the last 30 days prior to death, hospitalization for more than 14 days during the last month of life, multiple visit (>2) to the emergency department (ED) within the last 30 days of life, and hospitalization and/or admission to the intensive care unit (ICU). We excluded a sixth variable from the original composite, which was in-hospital death, as the program database at the clinic did not have data on patients who died at home. The composite score ranges from 0 to 5, higher scores indicating a higher level of aggressiveness in the EOL management.
Within the study design, approximately 30 variables were evaluated, which were extracted from the patients’ medical records. These variables encompassed most of the data presented in Tables 1–5. The inclusion of these variables allowed for a comprehensive assessment of various factors related to the patients’ medical history and EOL care.
Sociodemographic data of patients receiving treatment at Clínica de Occidente S.A. between 2017 and 2019.

PC, palliative care.
Clinical data of patients receiving PC treatments at Clínica de Occidente S.A. between 2017 and 2019 compared by groups.

PC, palliative care.
Aggressive treatment at the EOL in patients evaluated for early PC at Clínica de Occidente.
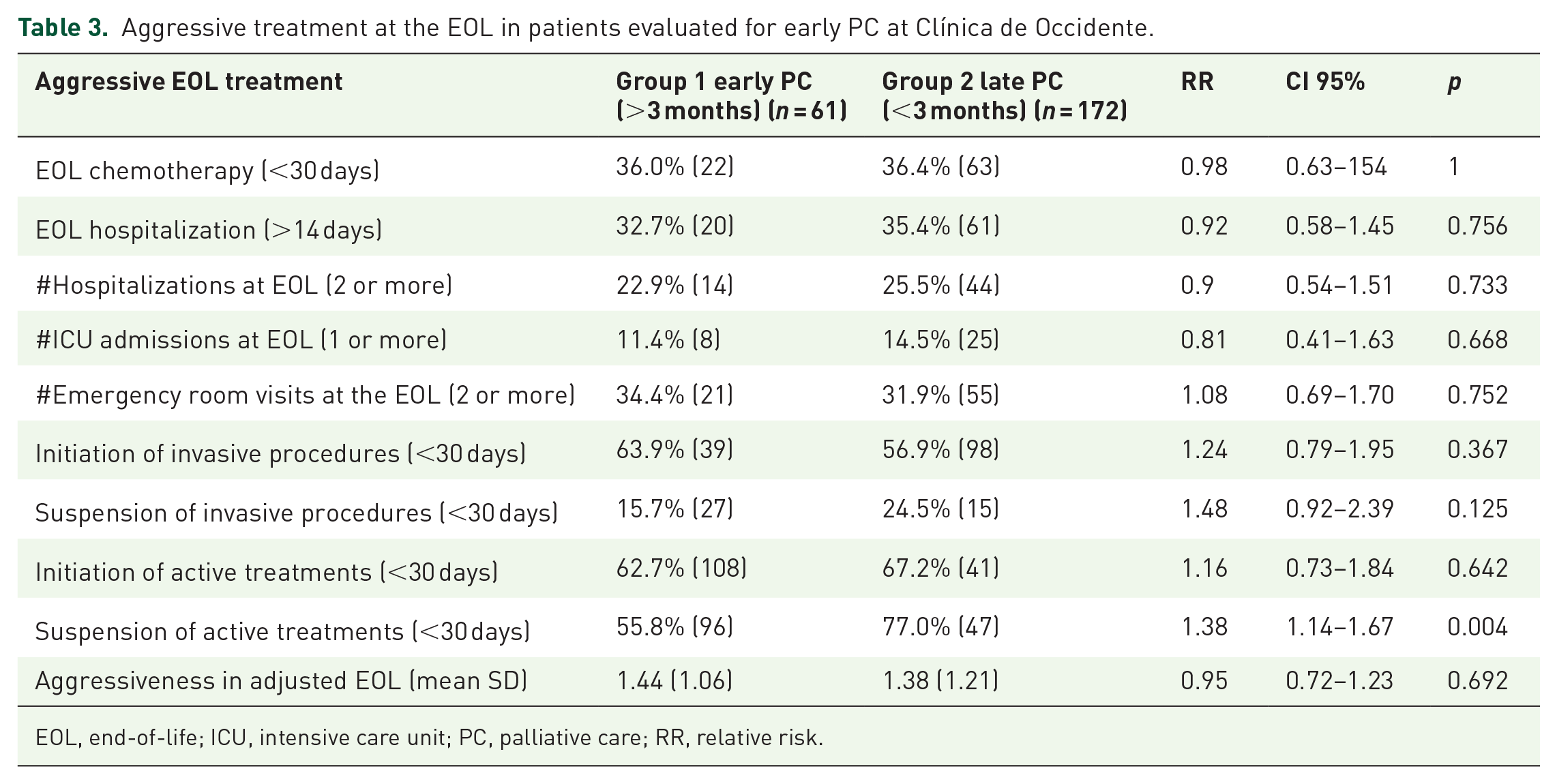
EOL, end-of-life; ICU, intensive care unit; PC, palliative care; RR, relative risk.
Aggressive EOL treatment in patients at Clínica de Occidente assessed by PC adjusted for aggressiveness in EOL.

Significant at 0.10 and CI 90%.
Significant at 0.05 and CI 95%.
EOL, end-of-life; PC, palliative care; RR, relative risk.
Shared decision-making/advanced directive.

PC, palliative care.
The principal investigators reviewed the patient’s medical records using their electronic records. To confirm reliability and validity another physician researcher checked the congruence between the data.
Population and sample
Our study focused on a cohort of 391 patients from the database of the PC program at Clínica Occidente S.A. These patients had been diagnosed with terminal oncologic disease and had passed away between 1 January 2017 and 31 December 2019. To be included in the study, patients had to meet certain criteria: they had to be over 18 years of age, have died from cancer or cancer-related causes during the study period, and have been evaluated by the PC program. We excluded patients who lacked documentation regarding the time, place, or circumstances of death, as well as those whose death resulted from a non-cancer pathology. Additionally, patients who had received medical care from an external institution within the last 6 months of their life or had received first-time medical care less than 1 month before the EOL (including emergency care, hospitalization, and outpatient care) were also excluded from the study.
Of the initial cohort of 391 patients, 25 did not meet inclusion criteria and an additional 133 patients had one or more exclusion criteria. Therefore, a total of 233 patients were included for this study (Figure 1).

Flow chart—sample selection.
Statistical analysis
A descriptive statistical analysis was conducted on the study population, including sociodemographic data, basic clinical data, physical examination data, functional and prognostic assessment data, aggressiveness markers data, and EOL data, as presented in the tables. For qualitative variables, absolute and relative frequencies were calculated, whereas measures of central tendency and dispersion were calculated for quantitative variables. Bivariate analysis was performed to assess associations between the categorical exposure variable (Early and Late PC) and the various outcomes, such as chemotherapy in the last 30 days of life, hospitalization for more than 14 days, number of ICU admissions in the last 30 days of life, number of hospital admissions in the last 30 days of life, number of emergency room admissions in the last 30 days of life, initiation and suspension of invasive treatments and procedures, and aggressiveness in EOL care. To control possible confounders and evaluate the impact of each variable in early admission to the PC program, a multivariate analysis was conducted using logistic regression. The variables with p values ⩽ 0.20 in the bivariate analysis were incorporated into the model. The model was built using the Backward strategy and assessed through likelihood ratio and Akaike’s information criterion. The most parsimonious model was selected.
Results
The demographic data of the study population (n = 233) revealed that 62% (n = 146) were female and the majority (70.8%) resided in the city of Cali. The age range was from 24 to 95 years, with an average age of 65.3 years. Among the patients, 32.6% were single at the time of their last PC assessment. Regarding occupation, 68% of women were engaged in household care and 15% were retired. In contrast 43.6% of men were retired. Approximately 42.4% of the patients reported having an extended family.
In terms of the time period, the year with the highest number of PC patients was 2018, accounting for 49.7% of the cases followed by 2019. The most frequent oncological pathology observed in the study population was related to the gastrointestinal system in both sexes (29.1%). Among women, breast cancer was the second most common (14.5%), whereas among men, genitourinary ranked second (9.4%) (See Table 1).
Regarding the clinical data, 34% of the patients were referred to the PC program by general practitioners. However, among the analyzed groups, patients who were admitted early to the program were referred by oncology in 50.8% of cases, whereas in the late admission group, they were referred by general practitioner and internal medicine in 37.7% and 33.7%, respectively. There were no differences in the frequencies of cancer anatomical sites between the analyzed groups, with gastrointestinal, breast, and genitourinary cancer being the most common.
Upon admission to PC program, 32% of the patients were receiving chemotherapy with curative intent, which was comparable in both groups. About 18% were receiving chemotherapy and/or radiotherapy with palliative intent, 16% had undergone surgery with curative and/or palliative intent, and 15% were not receiving any oncological treatment. In terms of opioids use, 79.4% of the patients entering the PC program had prior experience with opioids, and 45% were currently receiving morphine as part of their management. When comparing the two groups, 90% of patients in the early PC admission group had access to opioid management, whereas 75.6% of patients in the late admission group had access to this type of medication.
The most frequent symptoms reported upon admission to PC program were pain (72.9%), dyspnea (38.6%), and delirium (15.4%). There were no differences in the prevalence of these symptoms between the two comparison groups. In terms of functionality assessment, 54% of the patients had a Karnofsky score between 10% and 40%, which was similar in both groups. However, in the late admission group, 50.5% of patients had an ECOG score between 3 and 4, whereas in the early admission, the majority had an ECOG between 0 and 2 (42.6%).
According to the Barthel scale, 49.3% of the patients were classified as being in a state of total dependence. This predominated more in the late admission group versus the early admission group (see Table 2).
No significant differences were found based on early PC admission in the component indicators of the primary endpoint. This includes the use of chemotherapy in the last 30 days of life (36.4% versus 36%; RR: 0.98, CI 95%: 0.63–1.54, p: 1), hospitalization for more than 14 days at the EOL (35.4% versus 32.7%; RR: 0.92, CI 95%: 0.58–1.45, p: 0.75), having two or more hospitalizations at the EOL (25.5% versus 22.9%; RR: 0.9, CI 95%: 0.54–1.51, p: 0.73), having two or more emergency admissions at the EOL (31.9% versus 34.4%; RR: 1.08, CI 95%: 0.69–1.70, p: 0.75), and having any ICU admission at the EOL (14.5% versus 11.4%; RR: 0.81, CI 95%: 0.41–1.63, p: 0.66) (see Table 3).
In the analysis of secondary variables, a statistical significance finding was observed. The early PC admission group showed a decrease in the EOL aggressiveness when active treatments were suspended (77% versus 55.8%; RR: 1.38, CI 95%: 1.14–1.67, p: 0.004). However, no significant differences were found between the groups regarding the suspension or initiation of invasive procedures or active treatments (p: 0.125, 0.367, and 0.642, respectively) (see Table 3).
The study assessed the aggressive EOL treatment of patients based on the relationship between the time of admission to the PC program and the level of aggressive care received. A composite indicator, the adjusted EOL aggressive care score (adjusted EOL), was used to measure the level of aggressiveness in EOL care. Higher scores indicate more aggressive treatment. In the adjusted multivariate analysis, a difference was observed in favor of late admission to PC care for aggressive EOL treatment. The adjusted EOL score was 79.6% for late admission compared to 70.4% for early admission, with a relative risk (RR) of 1.98 (CI 90%: 1.08–3.59). Although the p-value (0.061) did not reach conventional statistical significance (p < 0.05), it is worth noting that we used a slightly relaxed significance threshold of p < 0.10 based on the methodology employed in this study. This suggests a potential trend toward more aggressive EOL care in the late admission group (see Table 4).
Additionally, in both groups analyzed, there was a lack of shared decisions and advance directives, with a similar absence in both groups (88.3% versus 86.8%). Among patients admitted late, 8.1% had advance directives, compared to 6.5% of patients admitted early. The limitation of therapeutic effort was primarily the responsibility of the patient’s family in the majority of cases in both groups (81.9% versus 78.6%) (see Table 5).
Discussion
This retrospective cohort study aimed to investigate the association between early admission to PC and less aggressive EOL care. The main findings of this study support the hypothesis that early admission to PC is linked to better EOL outcomes in oncology patients. One important finding of our study was the significant difference observed in the main variable, adjusted EOL aggressive care score (adjusted EOL), when adjusting the levels of significance by multivariate regression. This indicates that early admission to PC may have a substantial impact on reducing the aggressiveness of EOL care. which aligns with previous research studies.5,14,17
The median time between admission to the PC program and death was 26 days (mean, 72 days) reflecting the current status of PC access in our clinic. These findings underscore the importance of prompt referrals to ensure patients have adequate time to benefit from PC services.
Our multivariate logistic regression analysis revealed a significant association between the timing of admission to the PC program and the presence of aggressive treatments in the last month of life. Specifically, the initiation of invasive procedures within 30 days of admission was associated with a 3.12 times higher risk of receiving aggressive EOL care (CI 95%: 1.56–6.36, p: 0.001). These results highlight the critical role of early PC initiation, as delay in referral may lead to more aggressive treatments near the EOL. This correlates with previous studies, such as the study conducted by Hui et al., 19 which demonstrated that early PC (more than 3 months before death) is significantly linked to improved EOL outcomes. 19
Moreover, our study demonstrated that early referral to PC facilitated the suspension of active treatments at the EOL, indicating a measure of nonaggressiveness. This outcome can be attributed to overcoming dysthanasic processes including the cessation of futile treatments that do not have a short-term impact on EOL management. These findings align with previous studies, that have shown an association between early PC referrals and the utilization of PC programs, resulting in less aggressive EOL care. 18
An important finding was the limited referral to the PC program, particularly in the late admission group, by specialties such as oncology. This reflects the insufficient access to PC at this stage of life, 8 highlighting the fact that most patients enter the PC program due to complications of their oncologic conditions and/or during prolonged hospitalizations, which reduces the opportunity for timely interventions to limit EOL aggressiveness. Despite the continued efforts of international and Latin American associations to enhance access to PC services and eliminate barriers, this reality persists within the current healthcare system. Therefore, it is crucial to maintain a focused approach and explore further options to improve and provide additional tools to achieve this objective in future research, 21 this includes raising awareness and conducting training programs to underscore the significance of PC.
Additionally, our study revealed a lack of advance directive planning for patients at these stages, which hinders healthcare professionals from making decisions regarding the initiation and/or suspension of active or invasive procedures at the EOL. Consequently, the responsibility of decision-making falls on the patients’ relatives through limitation of the therapeutic effort or do-not-resuscitate orders to alleviate suffering. This phenomenon is not limited to Latin America, as evidenced by a study in Norway that demonstrate a prevalence of treatments in the last weeks of life that prolong life but create unnecessary aggressiveness. 22
Our findings correlate with several studies, 22 which have shown that patients who received PC consultation experienced better quality EOL care compared to hospitalized patients or those who did not received prior outpatient PC consultation. This included reduced hospitalizations and costs, increased hospice services, and higher ratings for care and communication by informed family members. Advance directives played a vital role in reducing unwanted treatments and aligning end. 23
This study has several limitations that should be acknowledged. First, it is important to note that this was a retrospective study conducted using medical records from a single institution, which may not fully represent the diversity and characteristics of the entire city or country. The reliance on a single institution introduces the possibility of selection bias and limits the generalizability of the findings. Additionally, the quality of the data could be affected by incomplete information in multiple medical records, potentially compromising the accuracy and reliability of the results. Another limitation is the unequal distribution of patients between the early admission group and late admission group, with lower proportion of patients in the early admission group. However, it is important to note that the sample size was deemed adequate for the specific analysis conducted in this study. Furthermore, it should be acknowledged that information on patients who did not die in the hospital was not available for analysis. This introduces a limitation in the assessing the ‘non-aggressiveness’ variable and its impact on ‘adjusted EOL’ variable. Future studies should aim to include a more comprehensive representation of patients across different care settings to provide a more holistic understanding of EOL care. Lastly, this study did not take into account additional palliative factors such as spiritual or post-mortem family factors, which could influence EOL care decisions and outcomes. Considering these factors in future research would provide a more comprehensive assessment of the impact of PC on EOL experiences.
Conclusion
Our findings highlight an important issue regarding the timing of PC referral in patients nearing the EOL. It is concerning that more than half of the patients in our study were evaluated by the PC program late, within 3 months before death. This late evaluation reflects a higher degree of aggressiveness in the treatment provided at the EOL. On the other hand, our findings suggest that early referral to the PC program, more than 3 months before death, is associated with higher likelihood of suspending futile active treatments, leading to reduced aggressiveness of treatment at the EOL. While our results indicate a trend toward a decrease in use of chemotherapy, hospitalization, ER visits, and ICU admissions at the EOL with early referral to PC, these associations did not achieve statistical significance.
In conclusion, our study suggests that early referral to PC may play a crucial role in reducing the aggressiveness of treatment at the EOL. Further research is warranted to confirm these findings and explore strategies to ensure timely and appropriate access to PC services for patients with advance illnesses.
Footnotes
Acknowledgements
The authors would like to acknowledge to the Pain and Palliative Medicine Program of Clínica de Occidente for their support in providing access to medical records of the study patients and to the Family Medicine Specialization program and the Department of Family Medicine of the Universidad del Valle for their assistance in preparing this manuscript.