
Abstract
Background:
About a decade after the introduction of palliative care teaching for undergraduate nurses and medical students in Uganda, it is unclear to what extent the course impacts students’ understanding, perceptions and orientation to deliver palliative and end-of-life care.
Objectives:
To (1) explore final-year nursing and medical students’ knowledge and perceptions of palliative and end-of-life care, (2) examine students’ orientation and perceived self-efficacy to provide palliative and end-of-life-care.
Design:
A multicentre exploratory qualitative study.
Methods:
A total of 82 undergraduate nursing and medical students were selected from seven medical and nursing schools in Uganda. Data were collected through 10 face-to-face focus group discussions using a pilot-tested interview guide and analysed using inductive thematic analysis.
Results:
Five master themes emerged: (1) Palliative care as a concept with multiple meanings, (2) Misinformation about palliative care, opiates and pain management, (3) Students’ experiences of the course, (4) Dilemmas in knowledge and action, and (5) Palliative and end-of-life care as emotional labour.
Conclusion:
Participants generally had inadequate and varied understanding of, and very few demonstrated low willingness and limited confidence to provide, palliative and end-of-life care. They blamed this mainly on the huge emotional labour of palliative/end-of-life care and inadequate teaching and/or limited clinical exposure.
Plain language summary
Why was the study done?
In Uganda, about 10 years ago, a course on caring for people living with life-limiting illnesses and the dying was introduced into curricula for undergraduate nursing and medical students. To date, there is no documented research about whether the course is positively influencing students’ understanding, attitudes, preparedness, and willingness to care for the dying.
What did the researchers do?
The research team selected 82 undergraduate nursing and medical students in their final year of study from seven medical and nursing schools in Uganda. Study participants were either pursuing a certificate, diploma, degree in nursing and midwifery or a degree in medicine and surgery. Ten group interviews comprising 4-13 students were conducted. Interviews were analysed to identify main topics.
What did the researchers find?
The researchers found that students had inadequate understanding, low preparedness, confidence, and willingness to work with people with life-limiting illnesses. Though they felt the theoretical information was useful and relevant to their training and future job role, they lacked or had very limited opportunities for experiential learning. They find it hard and confusing to translate the theory they learnt in class into practice. Hence, they find caring for the dying, handling challenging conversations and dilemmas in practice very difficult, and so they dislike it.
What do the findings mean?
Findings highlight inadequate training and mentorship and opportunities for experiential learning in real-life clinical and care settings. Training schools should place and rotate students in clinical and care settings for knowledge translation. Students will also need role models who can mentor them, impart the right knowledge, and enhance development of positive attitudes and skillsets required to care for the dying.
Background
The world is faced with a double burden of an ageing population and the increase in chronic non-communicable diseases.1–4 This epidemiological shift has not only increased demand for high-quality palliative and end-of-life care but also poses challenges for health educators and health providers who have both a professional and ethical duty to provide it.3,5–7
One important approach to addressing this need is for medical and nursing students to receive adequate education on palliative and end-of-life care during their training.8,9 The role of education in improving students’ knowledge of, as well as the positive attitudes and confidence to provide palliative and end-of-life care is emphasised by numerous other studies.7,10–18 Anyanwu and Agbedia 19 report how the level of nursing students’ understanding of palliative care has a bearing on the quality of care for future terminally ill patients. Higher levels of knowledge, improved communication, self-confidence, higher levels of concern and personal development have been reported among medical students who had exposure to palliative care training.20–22
Sadly, numerous studies have reported that many nursing and medical students are not confident nor ready to provide appropriate palliative and end-of-life care.23–25 Similar findings have been reported in newly graduated nurses,25–27 as well as in other healthcare professionals.28,29 Yet, it is inevitable that future nurses and doctors will encounter and be called upon to care for people in need of palliative and end-of-life care.6,8,30–33
Insufficient knowledge and inappropriate attitudes are prevalent among nursing and medical students and are widely recognised as major barriers to the provision of high-quality palliative and end-of-life care to patients and their families, including in high-income countries.12,25,34–42 Inadequate education and training among medical and nursing students, resulting in inadequate knowledge of palliative and end-of-life care, are major factors for negative attitudes towards palliative and end-of-life care, inadequate symptom recognition and management, building and maintaining relationships, provision of psychosocial and spiritual care, and communicating with patients and their families.43–52 Inadequate end-of-life content in the curriculum has been cited as one of the main causes of students’ inadequate knowledge and negative attitudes. 53 Zheng et al. 43 suggested that death education should be offered as a core part of undergraduate nursing and medical education curricula.
Close to a decade since the introduction of palliative care teaching into the nursing, allied health and medical training curricula in Uganda, it remains unclear as to what extent, if at all, it is positively influencing undergraduate nursing and medical students’ understanding and perceptions of, or their orientation, confidence and ability to provide palliative and end-of-life. Anecdotal observations in practice point to deficient levels of knowledge, multiple negative perceptions and superstitions about palliative care held by students and qualified healthcare professionals.
Furthermore, almost all the research on the topic is concentrated in high-income countries and may not be generalised to low-and middle-income countries like Uganda due to contextual differences. To note, an as yet unpublished international systematic review 54 that underpinned this study did not reveal any previous research that has recruited certificate level nurses, yet they are the most prevalent of Uganda’s health care workforce. This means that their knowledge and perceptions of and orientation toward palliative care are virtually unknown. This study, in part, addresses this evidence gap.
Aims of the research
To explore final-year nursing and medical students’ knowledge and perceptions of and palliative and end-of-life care.
To examine students’ orientation and perceived self-efficacy to provide palliative and end-of-life-care.
Methods
This study was conducted and reported according to the Consolidated Criteria for Reporting Qualitative studies (COREQ). 55
Design and setting
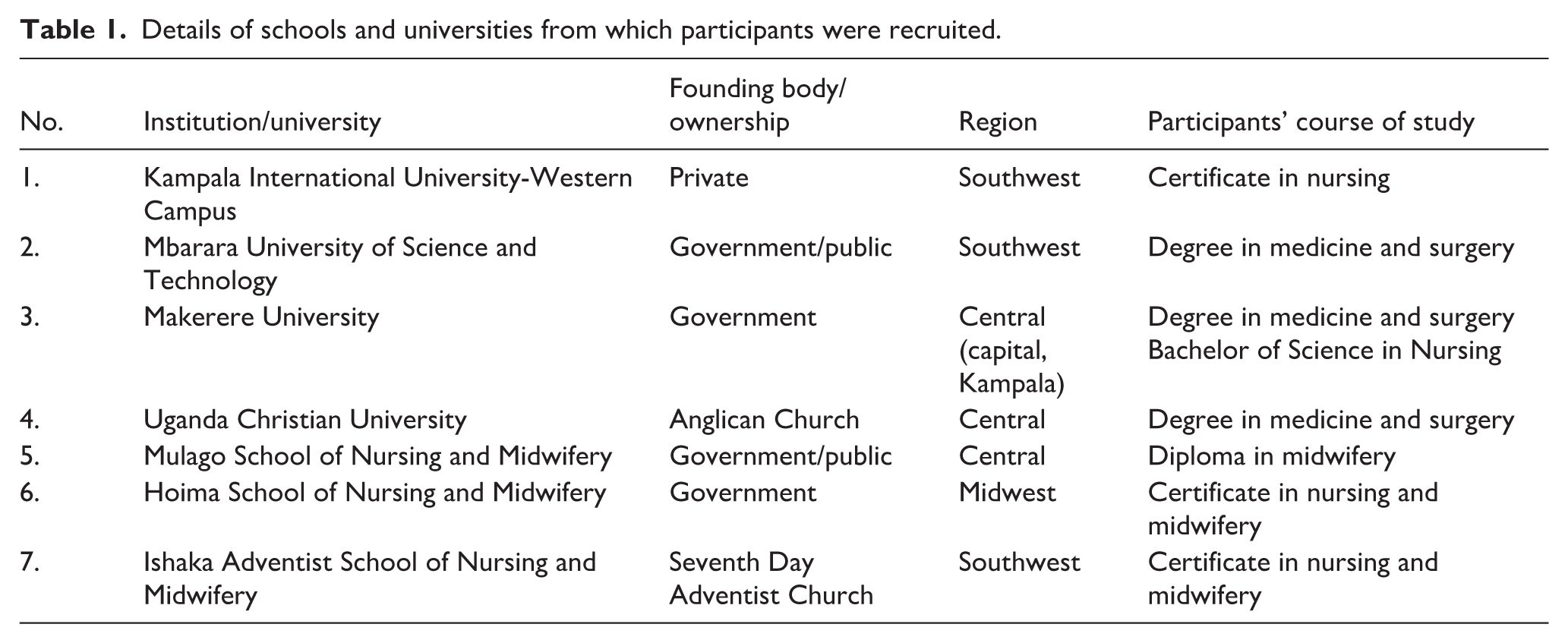
This exploratory qualitative study was part of a large multicentre mixed-methods study into final-year undergraduate (certificate level) medical and nursing students in eight public and private tertiary medical and nursing training institutions in Uganda, participants from seven of which took part in the qualitative element of the study. The details of the participating institutions are shown in Table 1:
Details of schools and universities from which participants were recruited.
Participants
Participants were undergraduate nursing and medical students in the final year of their respective course of study. Degree-level participants were medical students in their final (fifth) year and nursing students in their final (fourth year) semester. Diploma level participants were nursing students in their final semester of a 2-year programme. Diploma nurses and midwives had initially obtained a certificate in nursing and midwifery and been in practise for at least 2 years. Certificate level participants were nurses in their final semester of a pre-registration two-and-a-half-year certificate in nursing and midwifery course.
Sampling and recruitment criteria
Participating institutions were purposively selected in such a way as to have a good representation of the regions in Uganda and the courses of study. Participants were accessed through their respective department heads or deans after securing institutional approval. Convenience sampling was used to recruit participants as the researcher could not easily get the sampling frame to fulfil the criteria for random sampling, given the nature of the settings of the participants. Recruitment of participants was based on a voluntary basis. That’s to say, the sample size was based on those who volunteered to participate.
Eligible participants: (i) were nursing or medical students in the final year of their undergraduate training, (ii) were Ugandans (to increase sample homogeneity and minimize possible skewed variations due to cultural or contextual differences), (iii) granted voluntary consent verbally and by signature, (iv) were able to talk, read and write in English.
A prospective participant was excluded if they: (i) were non-finalists, (ii) were non-Ugandan/international students to minimize confounders related to home country factors such as prior experiential training or exposure to palliative care and (iii) declined to give their consent.
Data collection methods and instruments
To refine the interview guide and ensure its suitability, 56 the guide was piloted on an eligible convenience sample of nine final-year undergraduate (certificate level) nursing students. No major changes were made to the guide, and data from the pilot were used in the final analysis. Data collection took place between November 2022 and February 2023.
Data were generated through audio-recorded face-to-face focus group discussions by the lead author (GN), male gender, using the open-ended topic guide (see Supplemental File). Interviews were conducted in a quiet place selected with the guidance of either a department head or student leader at the participating institution. The constructs in the topic were designed in such a way to elicit and capture rich data 57 that seeks to address the aims of the study ‘knowledge, perceptions, orientation and perceived self-efficacy of undergraduate students to provide palliative and end-of-life care’. Questions included: (1) Probe questions: - to introduce and invite participants to the discussion, for example, I would like to hear your views about palliative care/end-of-life care, how did you find the palliative care training course? How familiar and confident are you in caring for seriously ill patients and their families? . . . (2) Follow-up questions: - to delve deeper into the topic of discussion and the participants’ opinions, for example, please would you share in more detail about (a) what you like/liked about palliative care? (b) what you don’t or didn’t like about palliative care and why? (c) Who do you think can offer palliative care to? (d) What are the benefits of palliative care (if any) . . . (3) Exit questions: - to confirm whether participants said what they needed or had to say, to invite questions from participants, to respond to and clarify their concerns.
The lead author, GN, moderated the discussions with the support of a note taker who captured non-audio recordable and non-verbal observations such as demographics of participants, that is, school, course of study, and participants’ level of agreement or disagreement about some aspects of the research, for example, significant disagreements and agreements among participants. The notes were later integrated into the transcripts and analysed with the rest of the data. Data analysis was conducted simultaneously with data collection. Questions were rotated in such a way that each participant had an opportunity to speak to ensure everyone’s participation and minimise generalised responses. Data collection was suspended at saturation, the most convenient way for sample size estimation in qualitative studies,58–60 when emerging themes became repetitive.
Data analysis
The audio-recorded focus group discussions were transcribed verbatim. Intelligent transcription was then applied to the resulting transcripts, in which step pauses, status, and filler words were removed while touching up grammar for clarity. Lastly, edited transcription was applied, that is, cleaning up the transcripts for readability and further clarity. At this stage, further editing of sentence structure, and reducing and summarizing some of the quotes, while maintaining originality, was done. Inductive thematic analysis – a rigorous, transparent and systematic approach to qualitative data analysis that seeks to ensure rigor, that is, trustworthiness, and credibility – was used to analyse the data 61 Thematic analysis is vital in summarizing and classifying raw data into broad-based categories that exhibit homogeneity in meaning for easier discussion.
A six-stepwise framework adapted from Braun and Clarke 61 guided the analysis: (i) GN immersed and familiarized himself with the data by repeated reading of the transcripts and highlighting participants’ excerpts and themes linked to the research objective. (ii) Took notes of the content areas to which the highlighted phrases and themes referred. (iii) Categorised content areas that were homogenous in intent and meaning into mutually exclusive categories and assigned unique codes to each category. (iv) Re-read and revised the categories, further grouping overlapping categories (those that expressed homogeneity) to formulate new, broad-based meaningful theme categories. (v) Organized linked categories into a hierarchical structure of topics, sections, sub categories and categories and finally (vi) wrote and reported the findings. At this stage, GN then shared the draft report and the transcripts with co-authors PE and EN, who read and re-read the transcripts while objectively comparing and contrasting them against the themes in the draft report. The co-authors shared their comments with GN and amendments, including appropriate movements, re-naming and pooling together quotes that reflected thematic homogeneity were made accordingly. Consensus was reached following discussions about the final master and minor themes included in the report. The number and naming of themes changed from three initial master themes to five master themes in the final analysis.
Rigour and trustworthiness
This study satisfied Lincoln and Guba’s criteria for ensuring rigour and trustworthiness of qualitative research. 62 Member-checking was undertaken by returning transcripts to two focus groups conducted with medical students. Three participants responded and confirmed that the information was a true reflection of what they had shared. Furthermore, the analysis, development and eventual confirmation of master and minor (sub) themes supported with participant narrative quotes was based on consensus reached by the research team with sound experience in qualitative research. These enhance confirmability. Prolonged engagement with participants from different course disciplines, teaching and training (medico cultural) and sociocultural backgrounds ensured sufficient depth and diverse perspectives and exploration of the phenomenon under study, rich data, hence triangulation and credibility of results.
Pilot testing the interview guide with a sample of nine eligible nursing students to ensure its appropriateness and pooling and pairing up together excerpts that reflected homogeneity in meaning from diverse focus groups to come up with master themes adds to the multiple dimensionalities of the themes, as well as credibility and dependability of the results. The description of the research methods and participant contexts, and the process underpinning and permeating the development of themes is very thick and elaborate and is supported with logical schematic frameworks for easy auditability and transferability.
Results
Characteristics of focus groups
Ten focus group discussions comprising 82 participants were conducted. The average time for the interviews was 1 hour and range 37 minutes to 1 hour 18 minutes. See details in Table 2.
Characteristics of the focus groups.

Themes
Analysis of the qualitative data from focus groups generated five master themes. (1) Palliative care as a concept with multiple meanings, (2) Misinformation about palliative care, opiates and pain management, (3) Students’ experiences of the palliative care course/training, (4) Dilemmas in knowledge and action, and (5) Palliative care as emotional labour.
Figure 1 shows the themes development framework, and Figure 2 shows the interaction between emergent themes.
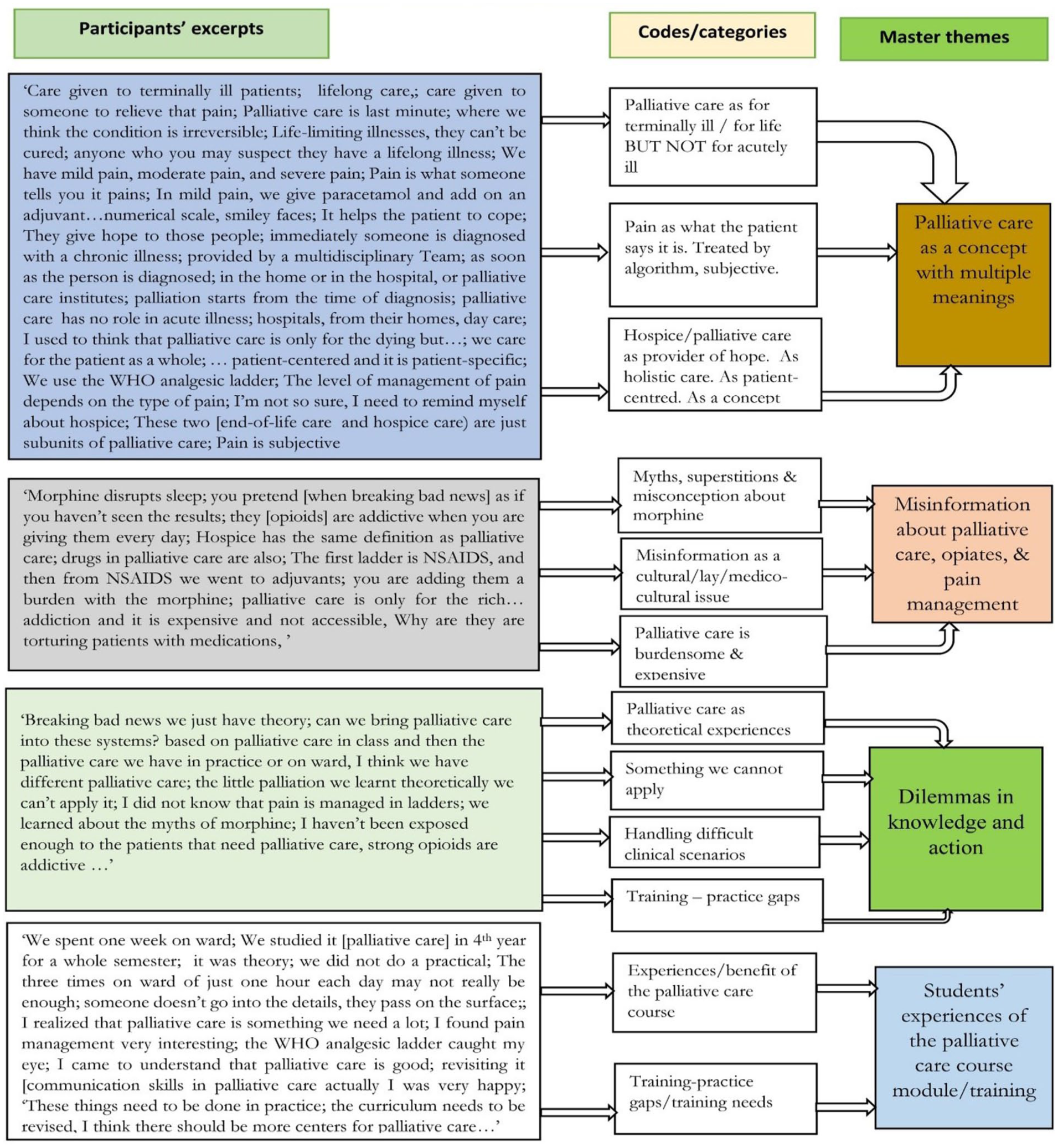
Themes development framework.
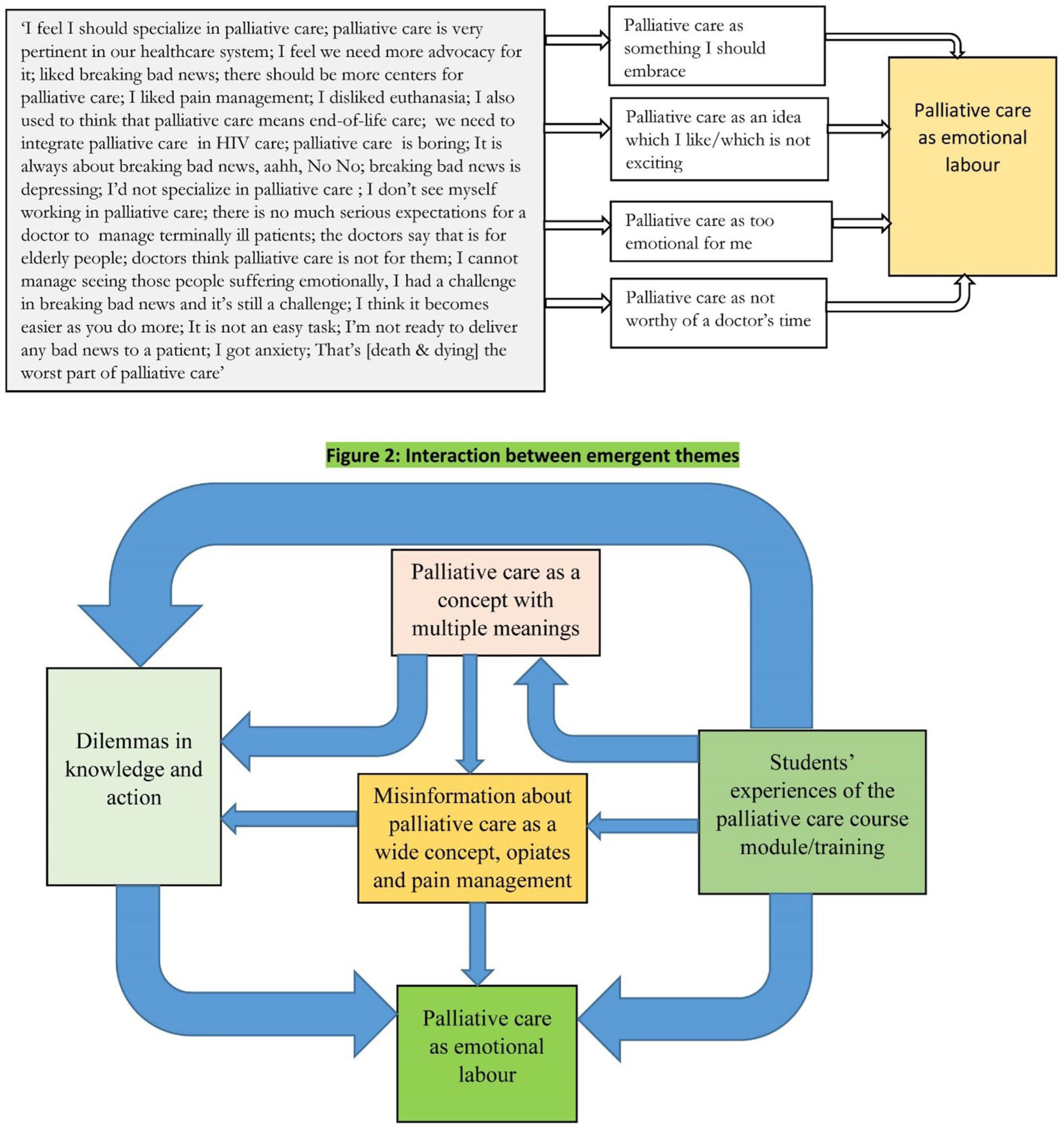
Interaction between emergent themes.
Theme 1: Palliative care as a concept with multiple meanings
Participants defined palliative care in terms of who, where and when it should be provided. Regarding ‘who’, all participants mentioned it is for patients with ‘life-limiting, ‘life-long or long-term’, ‘terminal’ ‘chronic’ or ‘life-threatening illnesses.’ They cited patients with cancer, HIV/AIDS, diabetes, heart problems, stroke and hypertension, TB, etc.: Palliative care is the care given to terminally ill patients with life-threatening conditions like cancer, HIV, hypertension, TB, diabetes, stroke and some serious accidents to relieve their pain. ECN, MP1, FGD 1
They were then probed to elicit their understanding of the terms ‘life-threatening, life-limiting or terminal illnesses’. The majority referred to them as illnesses that are ‘incurable’: A person who has a disease that can’t be cured. ECN, FP7, FGD 3
Sub theme 1: Students’ conceptualization of palliative, end-of-life, and hospice care
Participants demonstrated diverse views and cognition of the reality of the three terminologies. A few reasoned palliative care as a broad concept within which end-of-life and hospice care are sandwiched. Some, for example, those from school B had not heard of or had no prior knowledge about end-of-life care, which suggests some local biases exist in the curriculum: Palliative care starts at the time of diagnosis regardless of whether the illness is going to get cured or is at end-of-life, while for end-of-life care, we have come to a conclusion that this person is not going to survive the illness. MS, MP1, FGD 8 I’m not so sure, I need to remind myself about hospice, but palliative care and hospice care are different. One is a subset of the other. Palliative care is a bigger version, and it is started at the time of diagnosis, at the breaking of the news of the disease. End-of-life care is that care that is given when you notice that you can no longer do anything to bring back this patient. End-of-life care should come in close to the demise of the patient. Before then, palliative care should have been instituted. It will be too late if the patient is dying and we say now, palliative care. . .. MS, MP2, FGD 7
Whilst very few participants described the terms palliative and end-of-life care in terms of duration before death, some hesitated to attach a duration to it, saying that duration is unpredictable. Participants showed varied understanding and views, with many arguing that palliative care has no role in acute illness and others arguing it has: I don’t think I would attach a duration to end-of-life care. End-of-life care in itself would mean preparing someone who knows that they are going to die to come to peace with it. It might be in five months, a year. . .. MS, MP1, FGD 10 Palliative care has no role in acute illness. Some of these acute illnesses may bring certain fears, anxiety in a patient but still I think that should be addressed by the doctor explaining to the patient, addressing all their questions but not starting them on palliation. MS, FP2, FGD 10
Further probing of the participants was done to identify their understanding and views, specifically as to whether palliative care has a role in the management of early-stage cancer that has a likelihood of cure. Very few students reasoned that palliative care has a role in early-stage curable or treatable cancer: I think palliative care is for anyone who you may really suspect they have a lifelong illness. If someone has stage 1 cancer, they can get palliative care as well, because even in stage 1, you still have cancer and it’s still deadly or a life-threatening disease. Giving these patients palliative care could also add to the process of healing [two agree]. BSN, FP2, FGD 5 I don’t think a person who has stage 1 cancer qualifies to get palliative care, because, in stage 1, early-stage cancer, surgery can be done on the patient or the patient can be managed on and the patient becomes okay. It [palliative care) is for patients who are in the last stages of their illness. ECN, FP9, FGD 9
Some narrated that even in early-stage curable cancer, aggressive treatment such as chemotherapy and surgery may result in adverse events that require palliative care. Few, especially medical students, demonstrated a better awareness and understanding of the multidimensional suffering (total pain) associated with cancer, regardless of stage, and reasoned palliative care could improve the quality of life of those patients: Surgeries come with their consequences. A person who has got a road traffic accident and are in pain needs Palliative Care. BSN, MP7, FGD 5 Holistically, what is attached around cancer; anxiety, spiritual concerns. . ., the holistic approach to care would help this patient even if biologically they are more likely to be healed. Even the biomedical aspect, we are not 100% certain that they will be healed, because diseases especially cancer have no fully predictable trend and prognosis. So, I think the patient would need palliative care. MS, MP1, FGD 7
Regarding ‘when’, few participants in each of the groups interviewed responded that palliative care is applicable and starts from the time of diagnosis through the illness continuum: . . .Immediately, as soon as the person is diagnosed. ECN, FP2, FGD 1 It is an approach that improves the quality of life of a patient and their family members, and it is given to terminally ill patients, especially patients with chronic diseases like cancer and it is supposed to start immediately when the patient is diagnosed with cancer, not to start it when the patient is already bedridden. BSN, FP4, FGD 4
Many reasoned that it is only appropriate in advanced stages of the disease; at the end-of-life, and further explained that by the time palliative care is initiated, death is inevitable: Palliative care is for only dying patients. ECN, FP6, FGD 1 Palliative care is care given to people diagnosed with end stage or chronic diseases; and mainly manage pain and other symptoms. MS, FP8, FGD 7
The theme “when other treatments have failed” was common as some narrated that is the time when palliative care should begin. They saw palliative care as a safety net: Palliative care is given to people who have reached advanced stage of cancer or HIV or those who have gone to severe pain and have suffered for a long period of time with a chronic condition . . . Palliative care is given when all other attempts have failed [all agree]. ECN, MP4, FGD 2
Subtheme 2: Palliative care as a holistic, patient-centred concept
Very few demonstrated awareness of key principles of palliative care service provision. Notably, their knowledge of the principles varied widely. Medical students demonstrated a better understanding of ‘total/holistic care’ concept followed by bachelors nursing students, then certificate nursing and final diploma nursing participants: Palliative care does not only treat physical problems but also looks at the patient in totality; the physical, psychological, spiritual, social aspects. BSN, FP1, FGD 4 I liked the fact that the family is always involved. The patient is able to share their feelings and fears, they have someone to listen to them, not being left alone and they become an accidental death and die with dignity. In our usual medical practice, we just focus on the disease, but in palliative care, we focus on the patient and family. BSN, FP2, FGD 4
Only very few certificate-level nursing participants demonstrated an awareness that palliative care extends into the bereavement period: We saw that in palliative care, immediately someone is diagnosed with a chronic illness, palliative care is started, then you go beyond, even when that person rests [dies] you continue to comfort the family members. ECN, FP4, FGD 1 After the terminally patient has passed on, the care continues to their families in order to help them cope with the loss. ECN, MP6, FGD 9
Individualizing care and respect for patients’ autonomy, values and beliefs, for example, use of traditional and complementary medicine, and healthcare workers’ ethical duty to respect patients’ choices and beliefs were mentioned by a few of the medical students who further explained that respect for patient’s autonomy is key in avoiding or solving some clinical dilemmas, for example, patients requests for aggressive/futile and very expensive treatment/medicines, for example, at the end-of-life: Palliative care brings about cooperation in caring for the patient; they [patient’s family] are brought on board so that they know what is taking place. In case of any financial, spiritual, social needs. . .If you involve them [patient’s family], you’re building the confidence within them, to comfort them to relieve anxiety, stress, giving them psychological treatment. ECN, FP8, FGD 3 First of all, patient’s autonomy is key; they have a right to accept or refuse it [medical advice], but before you let them refuse or accept what you are telling them, it is about you to give them all the available information; the benefits, the risks. . .. So that if they say they want to continue even after you’ve told them everything, you let them continue. MS, MP2, FGD 7
Spirituality and spiritual care as well as multidisciplinary team approach aspects were mentioned by very few certificate and bachelor’s degree nursing students as being key concepts of holistic palliative care, who demonstrated limited understanding of the timing for initiation of spiritual care, for example, some narrated that spiritual care is given only at the end-of-life. They then discussed the ‘where’ aspect in palliative care delivery and almost all cited hospice, hospital, homes, etc., as places where palliative care can be provided: If you know that the patient is going to die, that is when you start spiritual care so that the patient will be having that hope of life according to how the scripture tells us. . … ECN, FP3, FGD 3 . . .in hospitals, from their homes, day care; for example, I heard from a patient who was from daycare in Mbarara [Mobile Hospice Mbarara]. ECN, MP5, FGD 2
Subtheme 3: Pain as what the patient says it is – subjective experience, treated by algorithm
Participants discussed the concept of pain in relation to their understanding of what pain is, its assessment, classification and management. All had some basic understanding of what pain is. Medical students demonstrated a better understanding of pain concepts than nursing students. Some referenced their own pain experiences to relate how bad pain is: We defined pain as unpleasant sensory and motor feeling which can be due to tissue damage. . .. BSN, FP3, FGD 4 Pain is what the patient says it hurts. MS, MP6, FGD 7 Pain is pain. I’ve had severe pain, intolerable pain. It was not a good experience. MS, MP6, FGD 10
They then discussed physical pain assessment, covering aspects of history taking, use of pain measurements like visual analogue scales, numerical rating scales, smiley faces, jerrycan, etc., and pain classification citing nociceptive and neuropathic pain. However, very few participants were willing and able to correctly demonstrate how to apply some of these measurements. To almost all, pain measurement was a concept but not a practice reality. Nursing students, especially if they were certificate level, demonstrated possession of the least theoretical knowledge of pain assessment: We have tools which we use, e.g. facial expression, finger scoring [demonstrates correctly how to rate pain on the fingers]. We can use jerrycan tools. . .. ECN, FP3, FGD 3 We use a rating scale of 1-10 where a patient tells you how he relates his pain out of 10; may be 10 for severe and 1,2,3,4 for mild pain. We also use the PQRST where we see the precipitating factors or what relieves it, the quality, radiation, then severity. . … BSN, FP1, FGD 4
Some of the nursing and medical students across all levels demonstrated an awareness of ‘total pain’ and emphasized the need to undertake a holistic assessment of the patient: Their pain is not only physical, it is also emotional and psychological. These people’s life is tending towards the end; they no longer perform their daily activities as they are supposed to. That kind of emotional pain can even be much worse than the physical pain. MS, MP1, FGD 10
Students’ accounts of pain management
Most discussed pain management, and referenced pain assessment, including the need to classify, diagnose and grade its severity, prior to management using the World Health Organization (WHO) three-step analgesic ladder. None referenced the WHO two-step ladder for children. Their understanding of pain management was varied, with some having good basic knowledge while others had inadequate knowledge. Notably, medical students had better knowledge of pain management than their nursing colleagues: The level of management of pain depends on the type of pain. Acute pain we manage it with first step of the analgesic ladder; NSAIDS-Diclofenac, ibuprofen. . . If the pain is moderate, that’s when we manage using weak opioids like tramadol. Sometimes, the cancer patients experience much pain that can’t be ‘cured’ with step 1 and step 2 analgesics, that’s when we look at the last step of the ladder; strong opioids and we start managing using drugs like pethidine, ‘codeine’ depending on the assessment. ECN, MP1, FGD 3 You assess the patient, grade the severity of the pain, and then you manage. E.g. moderate pain our first line we dive into weak opioids; we usually use tramadol, codeine, even pethidine. For severe pain, we give some morphine or fentanyl. MS, MP12, FGD 7
One medical student narrated about breakthrough pain and its indications, citing the need to re-assess the patient and revise treatment. Many of the participants, especially nursing students, disclosed that they lack the basic skills of pain assessment and management: They taught us something about that pain which comes in. . ., the pain has been controlled but there’s that pain which comes through. . . If someone is getting breakthrough pain that can be a signal to me that my titration [of analgesics) needs to be revised. MS, MP5, FGD 10 As per now, if they call me there is this patient who is dying in pain, come and advise, sincerely, I can’t. ECN, FP8, FGD 2
Theme 2: Misinformation about palliative care, opiates and pain management, death and dying
There was an amalgam of misinformation of varying degrees emerging and permeating different elements of palliative care, including participants’ understanding of what palliative care is and who it benefits, handling challenging clinical scenarios, opiates and pain management, death and dying etc. Notably, participants had varied misunderstanding of hospice care, with some mentioning that it is a building while others described it as a ‘philosophy of care’: Hospice is not a place; it is a philosophy of care. . … Dip-N, FP6, FGD 6 Terminally ill, I think it is not the right word we would use. I may say it [palliative care] is the care given to people who are faced with life-threatening illnesses but they are not very ill, but they have the condition that is worrying their life. . .. palliative care is given when there is no hope of life. Dip-N, FP4, FGD 6 We were told by some of our seniors that hospice is just another system in the US, where hospice is like their end-of-life care, and that it does not apply to our setting; for us we do palliative care as a whole, and palliative care is this care from the diagnosis. . . MS, MP2, FGD 7
Almost all the students had superstitions and misconceptions about opiates, particularly fear of addiction and tolerance, and that they had witnessed or heard similar fears voiced by their seniors. Almost all mentioned the fear of morphine solution causing addiction and respiratory depression, and hastened death: They [opioids] are addictive when you are giving them every day, every time. If you give once, it is fine. ECN, MP4, FGD 2 I would not like to make morphine as a long-term treatment for a patient who is in pain, Okay, tramadol yeah. BSN, MP7, FGD 5 There are scenarios where cancer patients or people in a lot of pain are getting increasing doses of morphine or other opioids and at a certain point you find that these doses are actually not good for them. Doses keep increasing until in one way or the other they end a patient’s life. MS, MP5, FGD 10
Very few, especially medical students, stated that they would give morphine if there were a clinical justification. Many of their views, however, were punctuated with elements of misinformation and poor understanding of pain assessment and opiate use: I think it [morphine] is not addictive as long as you give them in the right quantity and also conditions. ECN, MP7, FGD 2 . . . if I see the patient, especially cancer patient is in severe pain and the other analgesics are not working for him, I would advise the doctor to prescribe it. . . I think the addiction comes in as a drug abuse. Sometimes the patients simply increase the dose by themselves. So, when instructions are followed clearly, addiction rarely comes. BSN, FP2, FGD 4 One thing I would be worried about is not addiction, but tolerance; the patient will require large and larger doses to control the same pain. So, I would not really advise to give it for a long time. At end-of-life, the comfort of the patient overrides many things including the addiction. MS, FP3, FGD 7 I would let them be on morphine as long as it is clinically necessary; as long as they have the pain, and the treatment causes no side effects. We always weigh risks and benefits. If the patient is at risk of addiction but the immediate concern right now is their pain. . . and there is no such thing as bad as pain. Pain is very bad. MS, MP1, FGD 10
Some, more especially nursing students, reasoned that morphine (with all its side effects) and other long-term drugs when given to seriously ill patients in palliative care are even more burdensome, and this distresses them (students): You are dealing with a patient and the end of it all is death. Why are they torturing patients with medications? They take medicines from day one up to the day they die, knowing that even when they take those tablets nothing will change, they’ll die. That’s the only thing I hate about it [pallitiave care]. Why do they inflict that suffering on patients?. ECN, FG2, FGD 3
There emerged elements of ‘misinformation’ about the cost of palliative care, with students reporting that it is expensive. It can also be argued that to some extent, their narrations reflect the reality of what’s happening and what they observe in practice, as reports of patients being charged money (often excessive amounts) for morphine solution (which is cost-free) are increasing: The drugs in palliative care are also expensive, e.g. the strong opioids to manage pain are expensive e.g. morphine and pethidine. I witnessed a patient who was buying a bottle of morphine at shs [Ugandan shillings] 25,000. Now, my worry is, these patients from poor families, will they receive the services, will they afford? Palliative care services are only for the rich families. ECN, MP5, FGD 2
Very few, particularly medical students and registered nurses upgrading their qualification, demonstrated possession of good basic knowledge of and positive attitudes towards morphine use, and cited that their understanding, view and perception improved following the course. They cited clinical scenarios where optimal control of patients’ pain had failed until they switched to morphine, even when their seniors were initially hesitant or opposed to it: If you give it at right time, right dosage, if morphine is given in its right doses and right time and for the right diagnosis, you follow the prescription, you follow the rules of giving morphine, it cannot cause addiction. Dip-N, FP3, FGD 6 We learned about myths about morphine. I know that when morphine, if well titrated, it is not going to cause addiction. MS, MP3, FGD 8
Medical students were specifically asked about a morphine prescription, its components and who is legally allowed to make it (according to Ugandan law). They mentioned they only learnt the morphine prescription theoretically. None mentioned having had an opportunity to practice or even look at an already-made morphine prescription: Morphine prescription, I remember that we actually had a calculation in palliative care, but I don’t remember, we need to go back and read it. MS, FP5, FGD 8
A female participant added: I have seen morphine being used in other settings, especially in theatre during surgery. On the palliative side, I haven’t really interfaced with its administration and how it all goes. MS, FP2, FGD 10
Theme 3: Students’ experiences of the palliative care course/training
Subtheme 1: Lecture room experiences
They critiqued different elements of the palliative care course unit, including course design, duration, content, and its impact on their understanding and view of palliative care. Their critique and experiences emerged in three themes: theoretical experiences, field/clinical experiences, including the benefits and challenges (dilemmas) they encounter in translating the theory into practice, and finally their training needs. Some narrated how they feel that even the theory they received was thin and inadequate, and the training did not prepare them adequately to provide palliative care. Very few stated otherwise: We studied it [palliative care course] for a whole semester, and we did one exam, it was theory. We did not do a practical. . . ‘When they are teaching us, someone passes on the surface bit, they will not go into the details about how you are going to handle this patient’s condition. ECN, FP3, FGD 3 I was disappointed that we did not get a chance to get the clinical exposure. MS, FP2, FGD 8
Sub theme 2: Hands-on/field/clinical experiences
They then discussed their experiences in the clinical setting, particularly their level of interaction with palliative care patients, and with qualified colleagues, seniors. Notably, all the participants in the study reported limited-to-no exposure and interactions with patients with life-threatening or life-limiting illnesses, including those whose schools are within or near cancer treatment centers or hospices. They reported this created a dilemma in how to translate what they learnt in theory into practice: I have managed cancer patients at the village level’ [Only one has interacted with terminally ill patients]. ECN, MP7, FGD 2 We learnt palliative care once a week for one semester and we had a few days on the cancer, oncology ward to be taught what we learnt in the lectures. Every group went about three times. That time was good. Actually, we studied a lot, but we didn’t get time to practice all of it. The three times on ward of just one hour each day may not really be enough. MS, MP1, FGD 10
Sub theme 3: Benefits from the palliative care course module
All the participants mentioned they experienced some gains from the course, mainly improved knowledge of the reality of the need for palliative care. Very few shared about the very limited situations where they had to apply the theory they learnt: Before the course, I thought that these people die in a lot of pain, always miserable, they are neglected, but when I was in the class of palliative care, I saw that there’s some hope for them, quality of life, they don’t die so miserably in that hard pain which is so unbearable pain. . .. ECN, FP6, FGD 9 During that time in class, I realised that palliative care is something we need a lot. But when I was practicing in the holiday, there is this lady who had oesophageal cancer, I think it was in stage 4, and whenever we would do ward rounds, we would move from one patient to another and whenever we would reach her bed, people would say, ah, that one is on palliation, there is nothing to do. We would skip her. Then I was wondering, based on what we studied in class, what is palliative care? Then I asked, now for this patient we also need to give morphine? Then the doctor asked me, has she told you that she’s in pain? I don’t know if she was really assessed, whether at that time surgery wasn’t necessary? Then also, she looked a bit disturbed by being skipped on every ward round. She was on ward for six months. I was really disturbed. . .Coz, based on the palliative care we studied in class and then the palliative care we have in practice or on ward, I think we have different palliative care. MS, MP 4, FGD 10
Most participants referenced pain as one of the topics they understood and liked most. Particularly, they mentioned that from the course, they became aware of the subjective nature of pain and pain being inadequately or poorly managed in clinical settings: I liked pain management, I appreciated that most, we were in surgery rotation and there was this child who had fallen down the stairs and everyone cared about the cerebral. . . pathophysiology, what’s going to happen next, and then the surgeon was like, but have you managed the patient’s pain? Why are we caring about this thing when she’s in pain? At least now, we have appreciated that pain is very subjective. . .. MS, MP1, FGD 8
Participants, especially medical students, further quoted that the course addressed other crucial, exciting topics they never knew before, for example, handling bad news and how to deliver it, managing other symptoms, and knowledge of which they found relevant and applicable in all fields of medicine: I don’t remember disliking any particular topic. I think palliative care generally as course is a good one. The ones I liked most; we learnt about breaking bad news and the four stages of grief. I enjoyed learning about that psychology. MS, FP6, FGD 8 We studied some of the symptoms that people with conditions that affect various systems present with and how we can manage those symptoms. That was a good thing coz some of these life-limiting illnesses and the symptoms they bring are based on the systems they are affecting. It equipped us with some good knowledge on how to handle these symptoms e.g. in cardiovascular. . .. Then also, we learnt about pain management; the pain ladder. That was something good. I enjoyed it. Yes, we had done communication in communication skills but revisiting it in palliative care was nice, actually I was very happy coz palliation is all about communication, that is how you can be able to understand someone’s pain. . ., social, faith. MS, MP1, FGD 10
Subtheme 4: Students’ training needs
Students discussed their training needs and what they feel needs to be done to improve palliative care education. They critiqued the nature of instruction or delivery of the palliative care course, which they said is merely theoretical. Further, they mentioned that many facilities lack palliative care and requested that it would be good if they were rotated through settings, centers or wards that deal with patients with palliative care needs so that they are able to apply the theoretical knowledge they have learnt: Can we bring palliative care into these systems? I think the curriculum needs to be revised, because, like he [his colleague] has said, we were on that ward for three days, once in a week for three weeks. And in those three days, I don’t know about others, but for us we were just standing in a certain corner. We didn’t see patients, talk to them or what, we were just there for courtesy. The course looked more like a formality than giving us chance to do something. MS, MP3, FGD 10 The little palliation that we have learnt theoretically we can’t actually apply it because, when we meet those patients with life-threatening conditions on ward, from the way the doctors treat them, they say that one we are discharging through hospice. MS, MP1, FGD 10
Theme 4: Dilemmas in knowledge and action
Sub theme 1: Influences on practice: Paternalistic cultures-seniors’ views and behaviours, prohibitive laws
Participants gave multiple examples of when seniors of their own profession or another impact the ways in which care is offered and delivered. There is no challenge to this because it is not their place to do so. Things are done not on an evidence-base but rather because “they”, the seniors or doctors, do or say so. In this respect, there is a norm that palliative care is not for doctors, that pain relief is dangerous and addictive, and as a result, we believe we can do nothing, so therefore we do nothing. The influence on the students was such that in some cases it coloured their view of palliative care entirely, while others recognised the tension and sought to cognitise it or to blame the seniors: Morphine, they [doctors/seniors] say that it is for elderly people not children, that it is addictive. They don’t give it and they always tell us not to give it because they are fearing those patients to get addicted. That these strong opioids are given to the dying patients, those at end-of-life. BSN, FP5, FGD 2 Palliative care is still foreign. I experienced it in my last placement, we had two patients; the doctor recommended they were supposed to be on palliative care, but nurses were not even bothered. They could read the files but do nothing. The nurses who are supposed to help the patients get that special care are not caring; they neglect palliative care. ECN, MP1, FGD 3 There is still a bias towards palliative care. Knowing that palliative care is for hospice and people who have specialized in that part, not for doctors themselves to have the skills to provide the service to patients. We want to cure diseases and move on with life. BSN, MP5, FGD 10
Power imbalance, mostly nurses feel they are not given the opportunity to practice palliative care, in particular, making decisions was a striking theme. They (nurses) questioned and decried the unfairness in the law and professional codes of conduct, as these give decision-making powers to the doctors only: The negative side I saw, strong opioids are used which are not recommended to be prescribed by a nurse. Yet, when the doctor prescribes, the nurse gives and any negative outcomes that arise it is the nurse to be attacked first. ECN, FP2, FGD 1 Most of the laws do not allow health workers at our level to give drugs commonly used in palliative care. You assess, you do everything, but you will not be in a position to give the drug which is not prescribed by the doctor. ECN, FP3, FGD 2
Theme 5: Emotional labour of Palliative care / something other people do
Sub theme 1: Palliative care as how the students feel about and perceive it
Many participants did not think palliative care is for them, because the emotional impact is too great. This fear of the emotional effort has an effect on the ways in which they view palliative care, pain management and end-of-life care. Most notably, they referenced that they are not ready and/or not willing to take a career in palliative care and witness and manage the multiple overwhelming emotions from patients. Their perception of and orientation towards palliative and end-of-life seemed to be influenced by multiple factors, summarised in Figure 3.
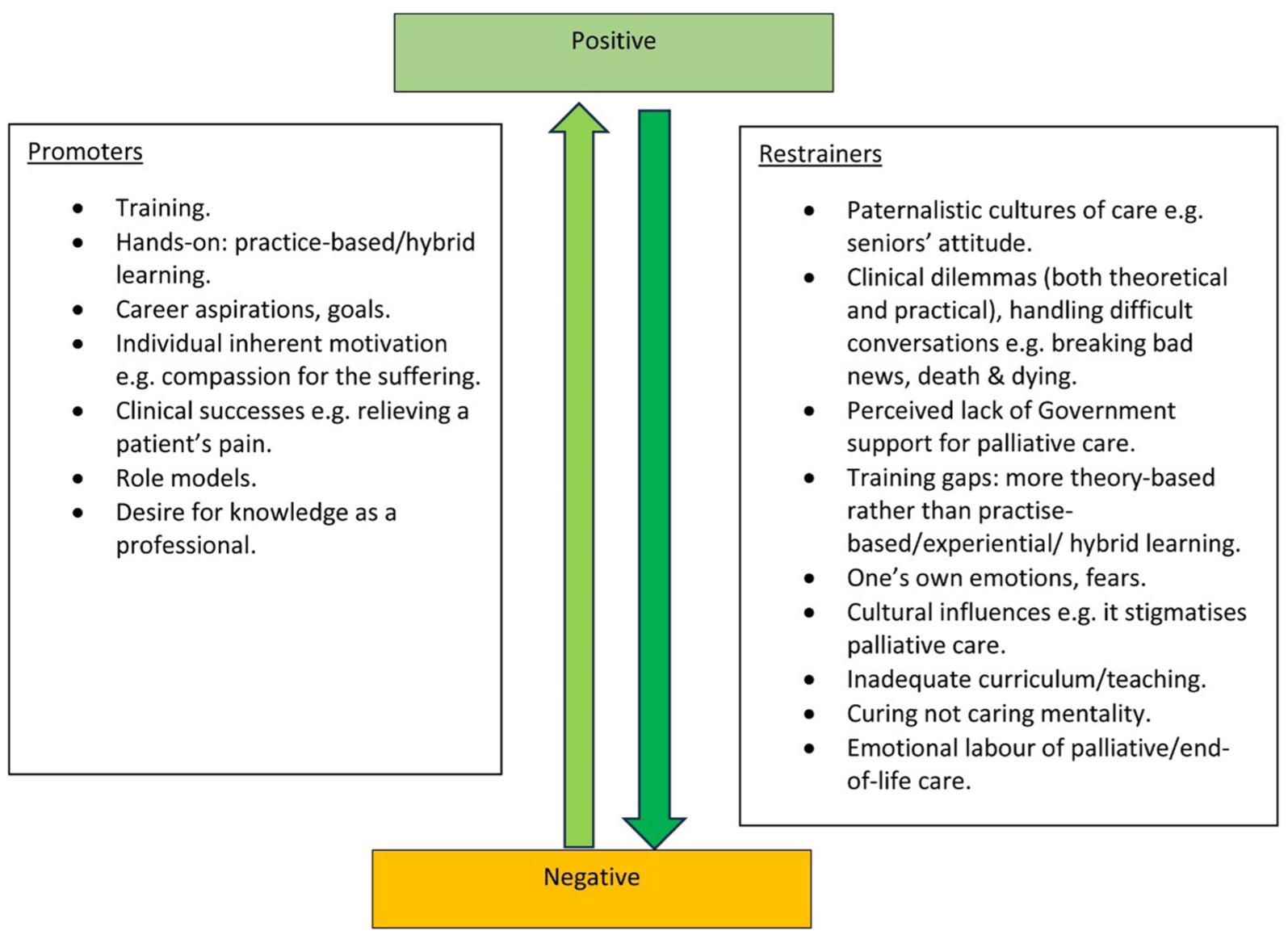
Promoters and restrainers diagram.
There was a recurrent theme of a gross lack of preparedness and unwillingness to provide palliative care that affected the majority of the participants. Medical students showed more negative attitudes and less willingness; however, nursing students demonstrated lower perceived self-efficacy to provide palliative care than medical students: Unfortunately, I cannot manage seeing those people suffering, emotionally I cannot manage it. . . ‘I see it as a difficult specialty. So, me to join that specialty, no, I cannot. ECN, FP2, FGD 1 That thing [palliative care] is irritating. One time I dealt with one lady [patient with diabetic wound], I hated it [palliative care] in my life. I was almost leaving this nursing course. The thing is bad. It [patient’s wound] was kinda fuming. There are conditions in palliative care that are such bad to handle. You can even reach a time when you dislike them [patients]. ECN, MP2, FGD 3 I find that medicine itself, being a primary physician is already emotionally draining and I think calliative care even requires more than emotional commitment. MS, FP5, FGD 8 I don’t find it [working with dying patients] easy, but am confident because I am someone who can look at a condition and a person and I feel what someone is going through. BSN, FP2, FGD 5
Very few participants narrated how the course shaped their view and understanding of palliative care and its importance, especially relief of suffering and promotion of comfort. As a result, they are now more willing to deliver it, with some mentioning that they would be willing to make a career in palliative care in the future: I feel I should specialise in palliative care. Those patients are like us. Even at one point, no one knows, I can also be a victim at one point. I don’t see any reason why I can’t help those people. They are like me.. . .. ECN, FP 2, FGD 1 My view of palliative care is that it is very pertinent in our healthcare system. It’s not been well absorbed, imbibed throughout our country but one thing I learnt from doctor [. . .] who was teaching us, it improves at least the quality of life and it also promotes the dignity of the patient towards their end-of-life. MS, MP3, FGD 8 I liked palliative coz, before, I thought palliative care is all about someone going to die. We had a neighbour; he had liver cancer. Hospice started caring for him and people kept saying he is going to die but he lived longer. I am so passionate about medicine and I love to meet people with terminal illness. So, when I saw palliative care, I don’t think I disliked any topic. Yes, breaking bad news is there, but I’ll see when I get to practice. MS, MP1, FGD 10
There was a striking theme where students’ dislike and fear of building a career in palliative care was perpetuated by the perceived lack of the government’s recognition and support for palliative care. Again, this was punctuated with some elements of misinformation and perhaps inadequate teaching: I heard that palliative care has just been brought into the system. But we don’t see like the government people concentrating and supporting it, e.g. like a day to celebrate it. You may find they don’t even budget for it. . . It worries me, coz if at all the government is not supporting it, is not promoting it, now what about us nurses? Because, for us we depend on the government. ECN, MP1, FGD 2
They then suggested remedies for some of the gaps they see in the health care system. Particularly, they referenced gaps in pain assessment and management by health workers and the need for all health workers to have knowledge of pain management: Palliative care is important and I am glad that we learnt about it, and I feel it should be included in curriculum for health workers. . .. No patient should be left to live in pain. MS, MP3, FGD 8 I wish that palliative care would be put into every single chronic illness, DM, HIV, that whole good system that HIV has. . .. MS, MP1, FGD 8
Sub theme 2: Students’ perceptions and attitudes towards death and dying
In addition to delivering bad news, discussing death and dying was the second most common challenge and topic disliked by most participants. They referenced how, based on cultural connotations, discussions about death are taboo, how they’re not comfortable and ready to discuss death and dying with patients, and how caring for the dying causes them psychological and emotional disturbances: It is emotionally discouraging because even when you care for these patients you already know that they are going to die. . .. It becomes emotionally disturbing, and you feel discouraged. ECN, MP1, FGD 1 You have people with you, but within you, death is near, you know that any time soon, you are actually going down the grave, and you don’t know where you’re going. . . ‘I got anxiety studying about death and dying and as a young girl, I don’t know, sometimes I find death abnormal. ECN, FP1, FGD 9
However, few showed a positive attitude towards death and dying, with only two mentioning how they like end-of-life discussions. They had an understanding and cognition of the reality of death and finality of life and the need for health workers to accept this reality and provide better end-of-life care for patients and their caregivers: . . .end-of -life, all of us understand that we believe that health workers we care but God heals. It’s our responsibility to explain to the patient so that he or she can understand that for every care we will give, there is a possibility of death. We can prepare the patient until he dies; find out the plans of the patient and see how you can help the patient and also the family. ECN, FP2, FGD 1 I would not like to be a palliative care specialist. He [the lecturer] talked about his work, how you really you put in a lot and it does not stop at the point of death, you go into the bereavement stage and beyond to see that the family is coping and they’re comfortable and can now move forward, and putting in all that for very many patients, I don’t think I can be able to do that. MS, FP6, FGD 8
Sub theme 3: Palliative care as a specialty/profession that is not profitable, not worthy of medical effort
Some mentioned that they’re not ready to work with patients with life-limiting and life-threatening illnesses because the main purpose they came to nursing or medical school is to treat and cure people and make money. Interestingly, on the other hand, they, especially medical students, recognised that they will inevitably be faced with situations that will require them to provide some form of palliative care in practice and appreciated those who have taken a career in palliative care. We are training to offer a service that can cure people from their illnesses. But for the case of palliative care, we are sure that the disease is going to progress until the person’s life ends. When you treat and the person is not improving, you feel discouraged and as if you have failed. It is better when you treat someone who came critically ill, after two days you see them laughing, you feel motivated. But today you treat this person, within two, three days the person dies. You treat another person, one month, three months, the person dies. Mentally, as a health worker, you get disturbed. BSN, MP5, FGD 1 I don’t see myself going into palliative care. Most of us came into medical school to help people, to relieve patients of their suffering. Making money is there, but we also want to see that patients are improving. But in Palliative Care, you are dealing with people who are really not going to improve. . .. MS, MP11, FGD 7 I don’t see myself working in palliative care. I don’t think I am called to do that, and I don’t think I’ll be strong enough to do that, but the ones that do it, the ones who are called like you, thank you very much coz it’s necessary. MS, FP 6, FGD 8
Discussion
The main aim of this study was to examine final-year undergraduate nursing and medical students’ knowledge and perceptions of and orientation and perceived self-efficacy towards palliative and end-of-life care. The study found that participants had a diversity of views and theoretical understanding of palliative care and who it may benefit, but a lack of uniformity in understanding. There was some rationalisation of the processes where the majority demarcated palliative and end-of-life care in terms of time duration. There was an awareness of when palliative care is appropriate, with the majority stating that it starts from diagnosis to death, even if they do not always and clearly know what it means or who it is for. Notably, much of their understanding was related to hearsay and theory from the classroom.
In our study, nursing students showed somewhat better, but limited, willingness to work with patients with palliative needs than their medical colleagues, contrary to the findings reported by Dobrowolska et al. 38 , who found nursing students demonstrated significantly lower interest in receiving training in palliative care. This low interest in working in palliative care and death avoidance among nursing students/interns has also been reported in other studies.25,39
There are some broad themes emerging from the focus groups which reflect an interaction between knowledge, skills and attitudes of the students to the elements of palliative and end-of life care. There was a striking recurring theme of egocentrism among the participants; they see the issues as being about them and how they feel and not about the patient or the patient’s family. To them, holistic and person-centered care are concepts that they like but which don't quite make it into practice. Palliative care is something others do, and others believe in, but it’s not for them (students). The disconnect between the theoretical notions of person-centeredness and what they actually see being done in practice confuses them. This leads students to couch things in relation to the impact on them rather than on the patient, for example, ‘how will the patient respond to me?’. That the students talk about person-centered care, but that it stops mattering when we cannot objectively meet needs, is a striking theme in this study. Some discussions revealed a somewhat widespread dislike of the patient being the person in charge, in essence denying person-centred care, for example, ‘palliative care is not like the other side of clinical sciences where you explain something and the patient is able to pick. . .’ This may relate to role models, training, and cultures of care or just fear of providing palliative care.
There was a gross lack of preparedness to talk about death and dying, and a failure to see the patient as someone who deserves the truth, for example, some participants narrated that palliative care is a profession where one ‘must tell lies’ as they narrated clinical encounters that involve ‘difficult’ or challenging communication such as breaking bad news, death and dying with patients and it is unsurprising that these were most highly disliked by almost all the participants in this study.
All the participants in this study narrated limitations ranging from partial to a complete lack of opportunity for hands-on learning. Lack of basic knowledge, low self-confidence, limited nursing skills, fear and unpreparedness and unwillingness to handle patients with terminal disease are phenomena that have been reported in numerous studies conducted with undergraduate nursing23,40,50,52,63–66 and medical students and graduates.21,45,67–71 Inadequate curricula and training in palliative and end-of-life care, including limited exposure to dying patients is a global crisis that is reported in numerous studies conducted with nursing and medical students.15,21,41,42,46,48,50,70,72,73 Yet, evidence shows end-of-life care courses improve students’ knowledge of, and positive attitudes towards, care for the dying13,16–18,48 and, in turn, their confidence. 45
Very few participants who had some form of exposure to experiential learning demonstrated better positive (but inadequate) attitudes and knowledge of palliative care concepts, such as person-centeredness, than their colleagues who did not. This is consistent with the findings of a study by Centeno et al. 74 who found that a palliative care course exposed second to sixth year Spanish medical students to the concepts and principles of palliative care, including improved awareness of palliative care, holism, patient-centredness, positive attitudinal and behavioural change, self-awareness, as well as helping dispel myths and misconceptions about it.
Evidence from observational and evaluation studies supports that clinical exposure and opportunities for interactions with terminally ill patients consolidate students’ knowledge, skills and confidence, including reducing death avoidance and increasing self-efficacy to provide palliative and end-of-life care.7,11,14–16,75–78 Hökkä et al. 50 corroborated that clinical placements help students to consolidate learning experience, while Pastrana et al. 15 found that bringing students directly from the hospital to patients’ homes for exposure reinforced learning. A recent study from the United Kingdom found nursing students recognised end-of-life care for children and young people as a sad but important part of the job, and one which can have a lasting impact, but which requires improved education and support. 52 Centeno et al. 74 in their mixed design evaluation found that medical students’ understanding of and attitudes toward palliative care improved, and misconceptions were dispelled, resulting in a re-conceptualization of relationships with patients and families, as well as their role as future physicians following a palliative care course. These studies, however, were set in high-income countries; hence; their transferability to low-income contexts should be treated with caution.
Students’ understanding of palliative care was punctuated with multiple elements of misinformation, and this was a central theme that permeates almost all the other emergent master themes. Numerous other studies report how misinformation and inadequate understanding of palliative care is prevalent among nursing and medical students.24,35,40,70,79–82
Misinformation about palliative care appears to be a wider sociocultural/lay issue but also a medico-cultural issue which affects all of the student. This affects attitudes and behaviours stigmatising palliative care and contributing to students’ inability to translate theory into practice. In our study, many participants cited that they don’t, or rarely, see their seniors providing palliative care to patients who they (students) feel need it. They narrated that doctors/seniors who are key decision makers in clinical settings are sometimes not available or are unwilling to orient them or listen to others’ views. They (seniors) dislike and stigmatize palliative care and this spills over to the students.
In this study, students showed a variety, from almost none to a basic level, of understanding about pain management. For the majority, pain is a nebulous physiological concept, just another symptom to treat, a concept rather than someone else's reality, and a mono-dimensional occurrence which they fail to see as a qualitative experience. To them, pain tools are a concept but not a practise reality, not a lived experience – they have some theory but at best very little idea as to how to apply them in practice.
There is a disconnect between the skills they possess and the desire to manage pain. Strikingly, only very few have ever assessed and graded pain but the majority are happy to treat it. Limited training regarding pain and knowledge deficits in the use of analgesics and failure to use pain assessment tools is reported in other studies.42,68,83,84 The need for adequate training in palliative care and pain management at undergraduate and subsequent levels is urgent.85,86
There is a lot of misinformation and poor understanding of opiates, and perpetuation of myths, with almost all participants stating that opiates are limited to adults, long-term opiates are addictive and hasten death, and that they cause respiratory depression, etc. The lack of education and knowledge as a perpetuator of myths and misconceptions about opiates among students and healthcare professionals is a phenomenon widely reported in studies elsewhere.40,87–94 The literature cites a paucity of expertise to teach palliative care as one of the contributors to inadequate training.95,96 There is much literature that contends that for novice nurses and medical doctors to be able to acquire adequate knowledge and skillsets, and the positive attitudes towards palliative care, their training must be adequate.7–18
The mythology students hear and learnt about end-of-life care, opioids, etc., is a recurrent theme and is perpetuated rather than dismissed as they become more educated. This also feeds into dilemmas and, potentially for some, moral distress – that is, they know what the right thing to do is, but are unable to do it. Our findings corroborate earlier research that has reported students’ attitudes towards death have a role in influencing their attitudes towards caring for the dying.19,97 Mastroianni et al. 98 reported that students’ attitudes and perceptions towards palliative care, death and dying are psychological and behaviours learned as part of their social and cultural experiences. Surprisingly, none of the participants in the study were aware of key palliative care developments in Uganda, for example, the availability of a division for palliative care services at the Ministry of Health, nor the existence of the Palliative Care Association of Uganda and the African Palliative Care Association, let alone the existence of an amended statute allowing specially trained nurses and clinical officers to prescribe morphine for the management of moderate to severe pain (since 2004). It is probable that teaching does not emphasise these crucial developments, yet these could potentially change students’ overall view of palliative care.
There was a common theme of admiration for people who do palliative care ‘but it is theirs’, ‘for someone else but not for me’. For the majority, more so if they were medical students, palliative care is not worthy of effort – it is regarded as not rewarding, and it doesn’t equate with their needs and preferences as health professionals. The ‘treat to cure and make money mentality,’ where failure to cure is seen as a failure, is a common finding in this study. Markedly, the need to cure and make money for most overrides the need to care. This is in opposition to palliative care, which is burdensome, slow, time-consuming, and full of emotionally draining.
That medical students are more interested in curing rather than caring is also reported in a study of Turkish medical students 38 and one of nursing students in the US. 99 This issue appears to be closely linked to the misinformation and the lack of, or inadequate, experiential exposure and mentorship, which amplifies the disconnect between palliative care theoretical training. Students own fears are projected onto the interactions with patients, the prescription, the care, the being with, the family care, the emotional labour associated with palliative and end-of-life care. For example, for some participants, their fear and unwillingness to venture into palliative care is related to a perceived lack of government support and recognition of palliative care evidenced by the limited visibility of palliative care in the health care system and public service structure; making them more vulnerable to unemployment should they work in palliative care, and affirming their notion palliative care is not that important.
Interestingly, from another lens, they see palliation as a safety net – something to turn to when everything there is has failed, but which also underlines how they equate palliative care with end-of-life care and failure. Ignorance is reported in other studies as a predictor leading healthcare professionals and general public to equate palliative care to end-of-life care.100,101
Strengths and limitations of the study
The study has notable strengths. First, the study was part of a larger parallel mixed-methods design using focus groups to gain a deeper exploration of the topic. Results reported here confirm and triangulate with results from the quantitative element of the study. 102 Furthermore, the results represent the rich and diverse views of participants from different disciplines, teaching and training, and sociocultural backgrounds. Second, the multicentre study design recruiting participants from eight schools and different courses adds to the generalisability of study findings, certainly within Uganda. Third, the study has unearthed the views of diploma and certificate-level nurses who have not been studied elsewhere. Fourth, this is the first study on the topic in Uganda. Hence, findings are novel; the study identified and discussed crucial insights into the nature, and to some extent, the quality of palliative care education, training gaps and needs and recommendations for improvement as voiced by the student participants.
Conversely, the study had a few limitations that are worth mentioning. First, the overarching influences of culture on the students’ overall learning experience, attitudes towards palliative and end-of-life care, handling challenging (‘difficult’) conversations, particularly breaking bad news, etc., are quite striking in this study. The methodology and aims of the study may not be able to account for these emerging influences. Future research should examine these further using more robust and appropriate methodologies, such as grounded theory and ethnography, to better understand how culture and its tenets influence students’ learning, knowledge, attitudes, perceptions and orientation towards palliative care and death and dying. Second, we were not able to obtain information on what palliative care content is covered in the curricula of the schools or universities, hence, potential limitations in accounting for its impacts on the observations made in this study.
Conclusion
The study found that participants generally had inadequate knowledge and were influenced by varied misinformation, resulting in grossly negative attitudes and limited confidence and willingness to provide palliative and end-of-life care. These observations underline deficiencies in training, and perhaps curricula. There is a particular need to integrate and strengthen practical, pedagogical and experiential training with theoretical teaching to foster skills development but also to allow for translation of knowledge into practise. These could be incorporated as an examinable component that is graded alongside theoretical assessments, for example, using objective structured clinical examinations (OSCEs).
There is likely an urgent need to review the palliative care curriculum to establish its adequacy in meeting the training needs of the learners. The review should look at critical aspects such as content, scope, and delivery of the course. It is likely, based on the study findings, that there exist knowledge gaps among those teaching the palliative care course modules that should be addressed.
It is imperative that students be rotated through appropriate clinical settings such as hospices, cancer centres and wards that care for patients with palliative and end-of-life care needs. This will give them exposure to patients and experience learning in a real-life setting, thereby helping them close the theory-practice gap.
The lack of mentorship and role modelling from teachers and seniors in clinical settings is a common theme and a barrier to the acquisition of knowledge, positive attitudes and skills among all the participants. There is an urgent need for teaching institutions/universities to strengthen mentorship for students while on clinical attachments so that they optimize their learning benefits from these field encounters.
In particular, there is a need to address prohibitive paternalistic cultures of care, mainly perpetuated by senior health professionals not willing to provide and discuss palliative and end-of-life care, whilst shunning handling challenging conversations and delegating them to students. Challenging conversations, death and dying are common and inevitable scenarios in clinical settings; therefore, training must empower future doctors and nurses to handle these tasks and not to shun them.
The amalgam of misinformation around opiates, particularly opioid phobia and pain management in general, is a common finding among all of the participants, and this fear of opioid use is closely perpetuated by inadequate theoretical training and the negative attitudes of seniors in the clinical setting. Training needs to pay special attention to these to dispel misconceptions, superstitions and stereotyping that surround and limits rational opiate use.
Failure to take these necessary steps means that future nurses and doctors will continue to leave training institutions with just some theoretical palliative care knowledge and a gross lack of understanding as to how to apply it in clinical practice.
Further, participants' discussions of morphine solution being ‘commercialised’ in some instances in health and clinical settings despite being a free medicine funded by the government of Uganda, need not be underestimated. Robust systemic mechanisms that can identify and take necessary disciplinary action against any violations or cases of opioid misuse need to be instituted. Such mechanisms could include sensitisation and putting in place safe ways in which patients or caregivers can report such cases.
Supplemental Material
sj-docx-1-pcr-10.1177_26323524261426016 – Supplemental material for Final-year undergraduate nursing and medical students’ knowledge, perception, orientation and perceived self-efficacy to provide palliative and end-of-life care: Qualitative findings from a parallel mixed-methods study
Supplemental material, sj-docx-1-pcr-10.1177_26323524261426016 for Final-year undergraduate nursing and medical students’ knowledge, perception, orientation and perceived self-efficacy to provide palliative and end-of-life care: Qualitative findings from a parallel mixed-methods study by Germanus Natuhwera, Peter Ellis and Eve Namisango in Palliative Care and Social Practice
Footnotes
Acknowledgements
We would like to acknowledge the preprint available on the Research Square Pre-Print server ![]() . The authors thank the following individuals who supported data collection for this research. Mr. Kintu Herbert, Mulago School of Nursing and Midwifery, Kampala, Uganda. Dr. Rogers Abaho (Rest in peace), Kampala International University and Medical Officer, Bushenyi District Local Government, Bushenyi, Uganda. Dr. Victor Niwamanyire, Makerere University College of Health Sciences, Kampala, Uganda. Dr. Kibet Emmanuel, Mbarara University of Science and Technology, Mbarara, Uganda. Dr. Robert Alinda, Uganda Christian University and Mulago National Referral Hospital, Kampala, Uganda. Ms. Mercy Akoragye, Student Midwife, Mayanja Training Institute, Mbarara, Uganda.
. The authors thank the following individuals who supported data collection for this research. Mr. Kintu Herbert, Mulago School of Nursing and Midwifery, Kampala, Uganda. Dr. Rogers Abaho (Rest in peace), Kampala International University and Medical Officer, Bushenyi District Local Government, Bushenyi, Uganda. Dr. Victor Niwamanyire, Makerere University College of Health Sciences, Kampala, Uganda. Dr. Kibet Emmanuel, Mbarara University of Science and Technology, Mbarara, Uganda. Dr. Robert Alinda, Uganda Christian University and Mulago National Referral Hospital, Kampala, Uganda. Ms. Mercy Akoragye, Student Midwife, Mayanja Training Institute, Mbarara, Uganda.
Ethical considerations
The research was approved Hospice Africa Uganda Research Ethics Committee on 20th/9/2022 (reference HAU-2022-03-A). Administrative was obtained from Makerere University School of Medicine Research Ethics Committee on 28th October 2022, and from the respective administrative authority in each of the participating institutions/universities. Written informed consent was obtained from each participant. All data collected and presented in the results in this study were anonymised to ensure the confidentiality of participants.
Author contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets generated and/or analysed in this study are not publicly available due to the sensitive nature of the data. Only transcripts but not audios are available from the corresponding author on reasonable request: gnatuhwera@hospice-africa.org or ngermans16@gmail.com.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.