
Abstract
Objective
To evaluate the final-year medical students’ perception of their competencies related to palliative care.
Materials and Methods
Two consecutive anonymous surveys at 6 and 12 months among 6th-year medical students at the Faculty of Medicine, Prince of Songkla University.
Results
One hundred and ten (66%) and 103 (62%) students completed the questionnaires at 6 and 12 months, respectively. With the criteria that at least 80% of them should be confident to manage the cases independently or under supervision, they perceived themselves to be good at holistic care and communication skills, but lacking in common symptoms management and ethical aspects. The common promoting factors and barriers for their learning experiences were reported.
Conclusion
This study identified many aspects necessary to improve the students’ learning experience in our compulsory longitudinal integrated palliative care curriculum.
Introduction
Palliative medicine education is an essential process that fills the gap between terminal patients’ needs and physicians’ competencies. Although the World Medical Association has declared that “Medical school curricula should include the teaching of palliative medical care” since 2006, 1 this process seemed to be inadequate in many medical schools even in developed countries. Recent surveys have described it as 'poor without compulsory courses', 2 'too little and too early', 3 'much remains to be done' 4 or 'need for an individual leader or champion. 5
Thailand is a developing country in South East Asia with palliative care services that have been categorized as 'localized provision’ by the International Observatory on End of Life Care in 2008. 6 Both service and education related to this health care system are still at their beginning stages.
Palliative care core curriculum, Prince of Songkla University in 2010. *

Included only the curriculum organized by palliative care education development committee.
Materials and Methods
Two consecutive cross-sectional surveys were conducted. All of the students were asked to voluntarily and anonymously answer the questionnaires at the 6-month (midyear) and 12-month (final) rotations in September 2009 and February 2010, respectively. These survey periods were chosen because our students are required to work in our medical school's Songklanagarind Hospital for 6 months and in one of the affiliated provincial hospitals for another 6 months in the final 6th year.
The questionnaires consisted of 4 sections according to our palliative care curriculum main objectives:
Ability to assess and provide holistic interdisciplinary palliative care for the patient and family. Ability to assess and provide treatment and care for common symptoms in terminally-ill patients. Ability to communicate end-of-life issues with patient and family. Ability to explain legal and ethical aspects related to end-of-life care.
In the first 3 sections, the students had to categorize their competencies according to the 4 following levels.
Having the knowledge. Having observed other staff. Able to perform by themselves under staff supervision. Able to perform by themselves independently.
In the last section dealing with legal and ethical aspects, the students had to categorize their competencies according to the 2 following levels.
Having the knowledge. Able to explain it to others.
In each section there were also open-ended questions for the students to describe their actual experiences, promoting factors and barriers in learning any of the competencies. The questions were
Please describe your experiences that indicate your development according to this learning objective and competency level. What are the promoting factors for your development? What are the barriers for your development?
The percentage of students in each category was calculated for both the 6-month and final surveys. The proportional difference between both surveys was analyzed with Pearson's chi-squared test using the STATA program. The investigators also manually performed content analysis of the students’ response to the open-ended questions.
The study protocol was approved by the faculty's ethics committee.
Results
One hundred and ten (66%) and 103 (62%) from a total of 166 final-year medical students anonymously responded the questionnaires at the 6-month and 12-month rotations, respectively.
Holistic Interdisciplinary Palliative Care
Most of the students, 87% and 94% from the 6-month and 12-month surveys, respectively, perceived that they could provide holistic care for the patients and families independently or under supervision (Fig. 1). One of the students reflected the experience (translated and paraphrased),
Students’ perception of their competencies in holistic care, symptom management and communication skills. “I had a patient with nasopharyngeal carcinoma with brain and lung metastases. I initially talked with the patient and family about the treatment plan, which was palliative care, and tried my best to take care of them by providing pain control and nutritional support, and talking with them about their feelings and what they wanted to do. I continuously took care of this case until the patient died. The patient and family were involved in the whole process of decision making; they accepted the treatment plan, cooperated with us and appreciated our work.”
Promoting factors
The common promoting factors for the students’ learning experiences were the opportunity to manage the cases by themselves (24%), opportunity to contact real patients (19%) and their attitude of wanting to help the patients (13%). These are some of their reflections,
“The staff allowed me to take full responsibility and manage the case by myself.”
“Taking care of a real patient did motivate me to search for more knowledge.” “I wanted to support the patient's family mentally.”
Barriers
The common barriers for the students’ learning experience were lack of knowledge or experience (18%), time constraints (18%) and heavy workload (17%). These are some of their reflections,
“I have no prior experience of doing this.” “It is time consuming to manage a case according to the palliative care concept, but actually we did not have enough time.”
Symptom Management
From the 6-month survey, the percentages of students who perceived that they could manage the common symptoms independently or under supervision were 92% for nausea and vomiting, 85% for pain, 77% for respiratory symptoms, 75% for anorexia, 74% for mood and sleep problems, and 69% for bowel care. The percentages increased to 92%, 87%, 79%, 80%, 75% and 77% in the 12-month survey for each symptom respectively (Fig. 1). One of the students reported,
“I could manage the patients’ side effects from pain killers such as constipation and vomiting.”
Promoting factors
The common promoting factors for the students’ learning experience were the opportunity to manage the cases by themselves (22%), their attitude of wanting to help the patients (22%) and the opportunity of contact with real patients (19%). These are some of their reflections,
“I had a lot of opportunity to learn when I was on duty alone.” “I felt empathy while taking care of real patients with suffering, which made me eager to help them.”
Barriers
The common barriers for the students’ learning experience were lack of knowledge or experience (89%), time constraints (22%), heavy workload (22%) and lack of staff to teach or supervise (22%). These are some of their comments,
“I didn't know the drugs action or how to manage terminal patients.” “There was no staff available to supervise my work.”
Communication Skills
Referring to the 6-month survey, the percentages of students who perceived that they could communicate with patients and families independently or under supervision about the goal of care was 85%, family perspective 85%, prognosis and truth-telling 78% and withholding/withdrawing treatment 77%. The percentages increased to 97%, 94%, 95% and 91% in the 12-month survey for each topic respectively. The percentage differences between the 2 surveys were statistically significant for the goal of care and truth-telling issues (Fig. 1). One of the students reflected the experience,
“I had a palliative care patient with acute myeloid leukemia. The patient himself was hopeful of surviving for a longer period of time than his very actual poor clinical condition warranted for. When we diagnosed his incurable condition, we talked with the patient and his family several times, gradually informing them about the prognosis. Finally, the family agreed with the 'do not resuscitate’ plan and the patient passed away peacefully.”
Promoting factors
The common promoting factors for the students’ learning experience were the opportunity to manage the cases by themselves (13%), the opportunity to practice frequently (13%) and senior staffs’ support and supervision (11%). These are some of their reflections,
“I had the opportunity to talk with the patient frequently.” “The senior staff supervised me when I communicated with the patient.”
Barriers
The common barriers for the students’ learning experience were lacking of teaching and supervision by senior staff (28%), lacking of knowledge or experience (16%) and heavy workload (12%). These are some of their reflections,
“I had no one to advice me how to communicate with the patient.” “I was not confident to break bad news to the patient and family, afraid to make them sad.”
Legal and Ethical Issues
The 6-month survey revealed that the percentage of students who perceived that they could explain matter related to patient autonomy was 87%, informed consent 81%, confidentiality 75%, substitute decision making 72%, resource allocation 68%, advance directives 60% and euthanasia 54% The percentages resulted 84%, 75%, 77%, 70%, 60%, 67% and 54% in the 12-month survey for each topic respectively (Fig. 2). One of the students reflected the experience,
Students’ perception of their competencies in legal and ethical aspects. “I informed the patient about his prognosis and care plans while he was still conscious and respected his decision.”
Discussion
The result of this study reflected the experiences from the Faculty of Medicine, Prince of Songkla University's compulsory palliative care curriculum for undergraduate medical students, which has been in place since 2001. During the surveying period in 2009–2010, the total mandatory hours were 30 (Table 1). In accordance with the criteria that at least 80% of the students should have the confidence to manage the cases independently or under supervision, some aspects were found needing further improvement, especially that related to symptom management, which included mood and sleep problems, bowel care, respiratory symptoms and anorexia. Less than 80% of the students also perceived that they could explain all the contents of legal and ethical aspects except autonomy. The students perceived themselves to be good in holistic care and communication skills. This study also demonstrated that their communication skill perceptions were improved with more clinical experience during the final year.
One of the strategies to improve palliative care education is to develop a formal curriculum. Although the 'placebo’ effect on medical students’ knowledge, skills and attitudes of a curriculum without compulsory palliative care course has been demonstrated by Ostgathe et al, the authors concluded that the final results were still poor. 2 Fraser has also demonstrated that students in medical schools with formal curriculum feel more prepared to take care of end-of-life patients than from those without it. 7 Palliative care education in our medical school before 2001 could be described as opportunistic. After 2001, we developed our curriculum following the principles proposed by Billings and Block in their 1997 status report. 8 These included longitudinal integration along the span of medical education tailored to students’ developmental stage, direct experience with terminally-ill patients and their families especially in the clinical years, with a focus on humanistic attitudes, communication skills, interdisciplinary teamwork and the opportunity to have self-reflection.
In this study, the most common factor that promoted the students’ learning experience in all aspects was the opportunity to manage the cases by themselves. To have 'clinical exposure’ to the patients has long been emphasized;7–10 this could be facilitated during the clinical years when real patient contact and frequent practice opportunities are available. Their attitude of wanting to help the patient could also be catalyzed by the contact with terminally-ill patients.
Topic details of palliative care ward rounds in 4 major rotations at Songklanagarind Hospital for the 6th-year medical students, Prince of Songkla University in 2010. *
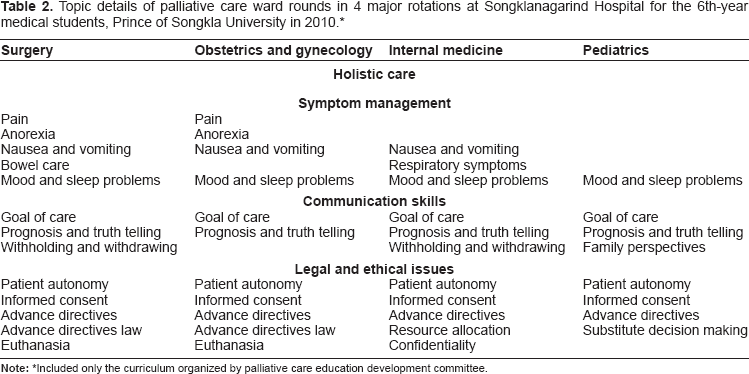
Included only the curriculum organized by palliative care education development committee.
Supervision and support from senior staff and physicians is also an important factor. In this study, the students mentioned that it could promote communication skills development. They also reflected that without it, they might have problems in learning how to manage the symptoms and communicate with the patients properly. The scenario that the staff or resident 'left him alone to do so’ to have a DNR discussion with the patient was described by the medical student in Wear's study. 11 Sullivan's national survey has also reported that the faculties and residents in USA felt unprepared to teach palliative care. 12 To overcome this barrier, the faculty and palliative medicine role models development are recommended.9,15–17
There were some limitations in this study. The voluntary response rate of about two-thirds of the students may lead to selection bias. The questionnaires did not include 'do not know or no experience at all’ choice for the students. This study also demonstrated only the students’ perception not the actual competencies in palliative medicine. All of these would result in a shift towards overestimation of actual competencies. The findings from the open-ended questions did show that many of them lacked knowledge and experience. The quantitative approach of this study also had limitation in perception issue, the national qualitative research based on our findings are currently studied including in-depth interview of more stakeholders such as the faculties, the students and the patients.
From this study, we could identify many aspects that may help to improve the students’ learning experience, including more clinical exposure, systemic integration of common symptom management and ethical issues into the major rotations, faculty development and a formal evaluation process.
Conclusion
These 2 cross-sectional surveys evaluated the longitudinal integrated palliative care curriculum at Prince of Songkla University's medical school as part of its continuous development process. Based on the criteria that at least 80% of the students should have the confidence to manage the cases independently or under supervision, our medical students perceived themselves to be good at holistic care and communication skills, but lacking in common symptoms management and ethical aspects. The common promoting factors for their learning experience were the opportunity to contact the patient and manage the cases by themselves during the clinical years, their attitude of wanting to help the patient, the opportunity to practice frequently and the senior staff's support and supervision. The common barriers included lack of knowledge or experience, time constraints, workload and lack of senior staff or physician supervision and support.
Author Contributions
Conceived and designed the experiments: SS, TS. Analysed the data: SS, TS. Wrote the first draft of the manuscript: TS. Contributed to the writing of the manuscript: SS, TS. Agree with manuscript results and conclusions: SS, TS. Jointly developed the structure and arguments for the paper: SS, TS. Made critical revisions and approved final version: SS, TS. All authors reviewed and approved of the final manuscript.
Disclosures and Ethics
As a requirement of publication author(s) have provided to the publisher signed confirmation of compliance with legal and ethical obligations including but not limited to the following: authorship and contributorship, conflicts of interest, privacy and confidentiality and (where applicable) protection of human and animal research subjects. The authors have read and confirmed their agreement with the ICMJE authorship and conflict of interest criteria. The authors have also confirmed that this article is unique and not under consideration or published in any other publication, and that they have permission from rights holders to reproduce any copyrighted material. Any disclosures are made in this section. The external blind peer reviewers report no conflicts of interest.