
Abstract
Objectives:
Effective pain management remains a significant challenge for patients with cancer, where disparities in care and treatment are evident. Patients from minority ethnic populations are often inadequately assessed and undertreated for pain. Patient-centred educational interventions have proven effective in enabling patients to communicate their pain to clinicians. However, the factors that make cancer pain education interventions relevant and acceptable for patients from minority ethnic populations are not well understood. This study aims to systematically identify, appraise, and synthesise evidence on educational resources for the assessment and management of cancer-related pain, and to evaluate their relevance for patients from minority ethnic populations.
Method:
A mixed-methods systematic review was conducted (PROSPERO: CRD42024498184), with searches in MEDLINE, EMBASE, PsychINFO, and CINAHL from inception to June 2025. Studies focusing on patient-centred educational interventions for the assessment and management of cancer-related pain were eligible for inclusion. The search was not limited to minority ethnic populations, as broader cancer pain education literature may offer valuable, applicable insights. Quality appraisal was performed with “QualSyst.”
Results:
A total of 3560 studies were identified, of which 62 (5 qualitative, 56 quantitative, 1 mixed-method) met the eligibility criteria. Only six studies specifically focused on minority ethnic populations, all of which were based in the United States and involved Hispanic, African-American, Indian-American, and Asian-American populations. Key components of educational interventions were identified, and an initial logic model was developed to guide the creation of future educational resources for cancer pain management.
Conclusion:
Evidence directly addressing cancer pain management in minority ethnic populations remains limited. Nonetheless, the review does identify promising intervention components and structural considerations for culturally responsive patient-centred care. Current evidence highlights the importance of developing tailored educational interventions aimed at improving knowledge, correcting misconceptions, enhancing communication, and promoting self-monitoring to empower patients to manage cancer pain effectively and seek help when needed.
Plain language summary
This study systematically reviews educational interventions for cancer pain management in minority ethnic patients, highlighting the need to improve knowledge, address misconceptions, enhance communication, and promote self-monitoring. The study presents an initial logic model to guide the development of future educational resources tailored to minority ethnic populations.
Keywords
Introduction
Cancer is the second leading cause of death worldwide, with approximately 20 million new cases reported in 2022 and a rising prevalence. 1 Pain affects many patients with cancer, increasing to 70% of patients at the advanced stage of the disease.2,3 Pain can be highly distressing and debilitating for those who experience it 4 with some considering it a sign of impending death.5,6 The Lancet Commission on Pain Relief and Palliative Care states that pain relief is a human right. 7 Cancer pain management requires a holistic approach, which considers both pharmacological and non-pharmacological approaches. Medication, including the use of opioids, is effective in controlling pain for around 90% of patients with advanced cancer,8,9 leading to clinically significant improvements in quality of life. 10
Despite the importance of pain management in advanced cancer, many patients continue to receive inadequate treatment. 11 For example, inequities in prescribing opioids to manage cancer pain exist and have specifically been noted among patients from minority ethnic backgrounds in addition to other intersectional factors, for example, sex, age, and socioeconomic status.12 –15 Most recently, disparities in the receipt of opioids were observed among patients from African-American and Hispanic populations in the United States. 16 A systematic review of 18 studies, primarily conducted at sites in the United States, found ethnic disparities in the receipt of opioids for cancer pain, even after controlling for factors such as age, health insurance, gender, and pain intensity. 17 Other studies within the review reported that patients from minority ethnic populations encountered unmet needs in terms of cancer pain management and worried about side effects, tolerance, and addiction related to analgesics.18 –21
The underlying causes for these disparities remain opaque, potentially involving patient, professional, organisational, and system-centred factors. 22 For example, ethnic differences in preferences for opioids might influence outcomes. Some individuals’ religious or cultural beliefs may influence their response to illness and symptoms. 23 Fears of dependency and side effects,24,25 along with the potential underreporting of pain due to unconscious negative stereotyping of minority ethnic patients by physicians, may also contribute.26 –28 Language barriers may further influence the communication of pain history. 29 A qualitative study of a sampling of safety-net clinics in the United States identified a reluctance among some clinicians to prescribe opioids to patients from minority ethnic populations with chronic, non-cancer pain due to perceived risks of misuse and addiction. 30 A recent study conducted in England, which analysed data from over 232,000 individuals in a 9-year cohort, identified that when compared to the White reference population, the odds of receiving a prescription for opioids were lower for minority ethnic patients near the end of life. 31 Shared understanding between patients and healthcare professionals regarding opioid safety, efficacy, and dependence, as well as open, effective communication, has been identified as a key factor in the successful assessment and management of cancer-related pain.32,33 Strengthening knowledge exchange and fostering meaningful dialogue about pain can enhance collaborative decision-making and improve outcomes. 34
To address this issue, patient-centred cancer pain education interventions have been developed to facilitate better cancer pain assessment and management.33,35 To date, two systematic reviews have examined cancer-related pain education interventions in the general population. Adam et al. 36 reported on 34 randomised controlled trials (RCTs) and identified that education interventions (for patients or healthcare professionals) have a small but significant effect on knowledge and attitudes and contribute to a reduction in pain intensity in patients with cancer. 36 Oldenmenger et al. 37 reviewed 26 RCTs and identified cancer pain education interventions that led to improvements in patients’ knowledge about cancer-related pain. After accounting for the heterogeneity across the studies, only 19% of patients in this meta-analysis reported a reduction in pain intensity. 37 These findings suggest that education interventions may benefit a subgroup of patients with specific characteristics, for example, poor health literacy. However, other key patient-centred characteristics, for example, patient ethnicity and culture, were not examined.
Important questions remain about the relevance of existing patient-centred cancer pain education resources for individuals from minority ethnic populations. Developing effective interventions for these groups requires a detailed understanding of the components, contexts, mechanisms, and causal pathways that lead to desired patient-centred outcomes. A systematic analysis of these elements can support the development of a logic model to inform the design of future educational resources. This model should be grounded in evidence from existing interventions developed for the general population, whilst also incorporating features that reflect the unique needs, preferences, and cultural contexts of minority ethnic communities. Although general cancer pain education resources may provide useful insights, their applicability to minority ethnic populations warrants critical examination. In addition, the cultural strengths and practices related to cancer pain management within these communities should be acknowledged and systematically investigated. 38 Therefore, this study aims to: (i) systematically identify, appraise, and synthesise existing evidence on patient-centred components, processes, and causal pathways underpinning cancer pain education interventions to inform the development of a logic model; and (ii) evaluate the relevance and applicability of these interventions to patients from minority ethnic backgrounds.
Methods
The research paradigm underpinning this mixed-method systematic review is rooted in pragmatism, which prioritises the research question over specific methods or paradigms.39,40 Given the complexity of the research question, this review combines quantitative and qualitative studies to provide a comprehensive understanding of the components and mechanisms of action of cancer pain education interventions.
This systematic review was performed based on the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines 41 (PROSPERO registration CRD42024498184). We reviewed all types of original studies, including randomised clinical trials, qualitative, quantitative, and mixed-method studies.
Search strategy and eligibility criteria
The SPIDER framework was used to develop the search strategy, as shown in Table 1. The following electronic databases were searched: MEDLINE, EMBASE, AMED, PsycINFO, CINAHL, and CENTRAL (Cochrane) from the databases’ inception to June 2025. In addition, key journals were hand-searched (2019–2025) to ensure that no recent studies were missed in the relevant literature: Journal of Pain and Symptom Management, Palliative Medicine, Psycho-Oncology, Journal of Palliative Medicine, BMJ Supportive and Palliative Care, and Journal of Clinical Oncology. No study was excluded based on the country or language. In our search strategy, we did not restrict study selection to those conducted exclusively in minority ethnic populations. This is because insights from the broader literature on patient-centred cancer pain education may also have relevance to minority ethnic groups.
A summary of the search strategy using the SPIDER framework.

Information source: The search items used for MEDLINE/Ovid, PsycInfo/Ovid, Embase/Ovid, and CINAHL/Ebsco are shown in Supplemental Material 1.
Data management and extraction
References were imported into Covidence (Veritas Health Innovation, Melbourne, Australia) (an online platform to streamline the systematic review process) to remove duplicates and manage data. A data extraction form was piloted and then used to include general review information, study methods, outcome measures, results/findings, and quotations. Data extraction was conducted by one reviewer (T.D.), with 20% of the extracted data from the included articles verified by a second reviewer (D.W.) within the Covidence management platform. Any discrepancies were discussed with J.K. and J.H. to reach a consensus. The PRISMA flowchart was used to depict the study selection process (Figure 1).

Flowchart of the study selection.
Quality appraisal
The Standard Quality Assessment Criteria for Evaluating Primary Research Papers (QualSyst) was used to assess the quality of both qualitative and quantitative studies. 42 As this review incorporated qualitative, quantitative, and mixed-methods primary studies, we used the QualSyst tool to ensure a consistent and comparable appraisal across diverse study designs. The QualSyst provides two complementary checklists, one for quantitative studies (comprising 14 questions) and one for qualitative studies (comprising 10 questions), allowing a parallel assessment of methodological soundness, transparency, and reporting quality without privileging one methodological tradition over another. This tool has been widely adopted in systematic reviews integrating heterogeneous evidence. 43 It enabled us to evaluate internal validity, transparency of data collection, and analytical rigour whilst maintaining parity across methodological types. Each question was scored as 2 = yes, 1 = partial, or 0 = no. When a question did not apply to a particular study type (N/A), the criterion was excluded from the summary score calculation. Summary scores were therefore calculated by summing the total score across relevant items and dividing by the possible maximum score.
If the QualSyst score is 0.80 or higher, it is interpreted as strong quality; 0.60–0.79 as good quality; 0.50–0.59 as adequate quality; and 0.50 or lower as poor quality. T.D. assessed the quality of all the studies, and D.W. verified 20% of the studies independently, where discrepancies were discussed with J.K. and J.H. to reach a consensus.
Synthesis methods
We employed a data-based convergent design in which both quantitative and qualitative data from all included articles were analysed using a unified synthesis method after data transformation (e.g. converting quantitative data into themes) as described by Hong et al.43,44 The results were then used for a narrative synthesis of the concepts. 45 For ethnically focused studies, the results were critically examined to identify the distinctive features of the interventions for patients from minority ethnic populations. Logic models are increasingly recommended in systematic reviews addressing complex questions about the hypothesised pathways and mediators that link intervention components to outcomes. For all studies included in this review, the findings were used to construct a logic model according to the guidelines by Rohwer et al. 46 and Kneale et al. 47 In brief, a process-oriented framework was adopted. Educational interventions from the included studies were first critically examined to identify patient-centred components and intended outcomes. Then, potential pathways (mediators) linking these components to the outcomes were extracted. An initial logic model was subsequently developed through an iterative process to visually map these relationships and illustrate the underlying mechanisms of change.
Results
A total of 3560 studies were identified, of which 62 studies are included in this review. Figure 1 presents the PRISMA flow chart. No other studies were identified by hand searching (cross-referencing or journal content pages).
Study characteristics
Supplemental Material 2 presents the characteristics of selected studies that were included and assessed. The dates of publication range from 1987 to 2025 and include 57 quantitative studies, 4 qualitative, and 1 mixed-method study. Most studies were conducted in the United States (n = 23), followed by China (n = 7), the Netherlands (n = 5), Norway (n = 3), and Taiwan (n = 3). Six studies specifically focused on cancer-related pain among patients from minority ethnic populations, and patient ethnicity was reported in 8 of the remaining 56 studies, all of which were conducted in the United States.
Quality appraisal results
Supplemental Materials 3A and 3B present the quality of all included studies based on QualSyst tools. The quality of the articles was appraised as “strong” (n = 38), “good” (n = 18), and “adequate” (n = 5). No articles were excluded due to poor quality.
Qualitative studies
Patients’ experiences of educational interventions were investigated in five qualitative studies.48 –52 The summary of these studies is located in Supplemental Material 4. No qualitative studies focused on patients from minority ethnic populations. A common theme in the qualitative studies focused on patients’ attitudes and knowledge about analgesics, particularly opioids and the risk of addiction. For example, a patient with cancer reported: “. . . I would never have risked taking more [morphine], because I thought that I would then be completely gaga. One never talked about that. And then, you’re just constrained. Because it is said that morphine is addictive.” 48 Patients’ knowledge about opioids and their willingness to use or avoid them were influenced by personal philosophies, negative personal or peer experiences, and difficulties in understanding complex information or distinguishing between chronic and breakthrough pain.51,52 For example, “[Patient with cancer:] . . . but I’m sort of old school. I was brought up not to take any medications until you’re right in the midst of it.” 51 Additionally, many patients struggled to apply complex medical information to their daily lives. Their assumptions significantly impacted their help-seeking behaviours, with some feeling ashamed to ask for stronger medication and others feeling guilty for not being strong enough. For example, “[Patient with cancer:] . . . But I feel a bit, like sinful in some way, I mean when I sort of beg for it, then maybe he or she is thinking ‘Oh, that’s the way it is’, like I’m awfully eager to get myself some drugs.” 51 Some patients believed that pain was a normal part of cancer or its treatment. For example, a patient said, “You don’t know if the pain is part of the cancer treatment or not. You also feel very insecure in terms of the pain.” 50 One of the qualitative studies indicated that concerns about the effects of medication on themselves as well as their families also contributed to patients’ fears. 48
Qualitative studies also reported how education interventions/resources positively affected patients with cancer pain. For example, “As one who was living in constant pain, I was not one to call the doctor. If I had this resource available, maybe things would have changed for me a lot faster than they did . . ..” 49 In another example, “[I feel] very well, because I learned a lot from Mrs S [Nurse]. And that makes me feel more secure.” 48 In terms of study quality, three of these studies were appraised as being “good” and two as being “adequate” using the QualSyst assessment tool (Supplemental Material 3B). However, all studies lacked evidence of reflexivity. Only one study made use of a theoretical framework to guide the research process. 48
Quantitative studies
Various educational interventions have been reported for managing cancer-related pain, focusing on patient and caregiver education about pain management strategies and addressing concerns. These interventions aim to improve treatment use and overcome communication issues and misconceptions. Notably, three interventions—PRO-SELF,48,51 –59 TEC (Tailored Education and Coaching),60,61 and PEP (Pain Education Programme)62 –67—were more frequently employed in different countries and applied in multiple languages.48,55 –58 Distinguishing features of PRO-SELF, TEC, and PEP interventions are their emphasis on patient empowerment through education and self-management,48,51 –59 enabling patients and caregivers to actively participate in managing the disease and its symptoms. This approach helps patients take a more active role in their pain management and fosters confidence in their ability to do so. In addition, these interventions provide personalised education and support by tailoring information and coaching strategies to meet each patient’s specific needs, preferences, and circumstances, thereby enhancing pain management.62 –67 Their adaptability to various care settings, including hospitals and home environments, ensures accessibility and applicability to a broad range of patients and caregivers.
Components of educational interventions for the management of cancer pain
Table 2 outlines the components of educational interventions relevant to cancer pain management in all studies included in this systematic review. Sixteen intervention components, categorised under seven themes, were identified. A key aspect of the assessment in several studies was evaluating and understanding individuals’ knowledge about their cancer pain and analgesics to manage it.33,68 –70 In addition, assessing self-efficacy formed an integral part of certain educational interventions, including the PRO-SELF, TICAA, and TEC.52,59,60,66,71
Components of education intervention for cancer pain management.
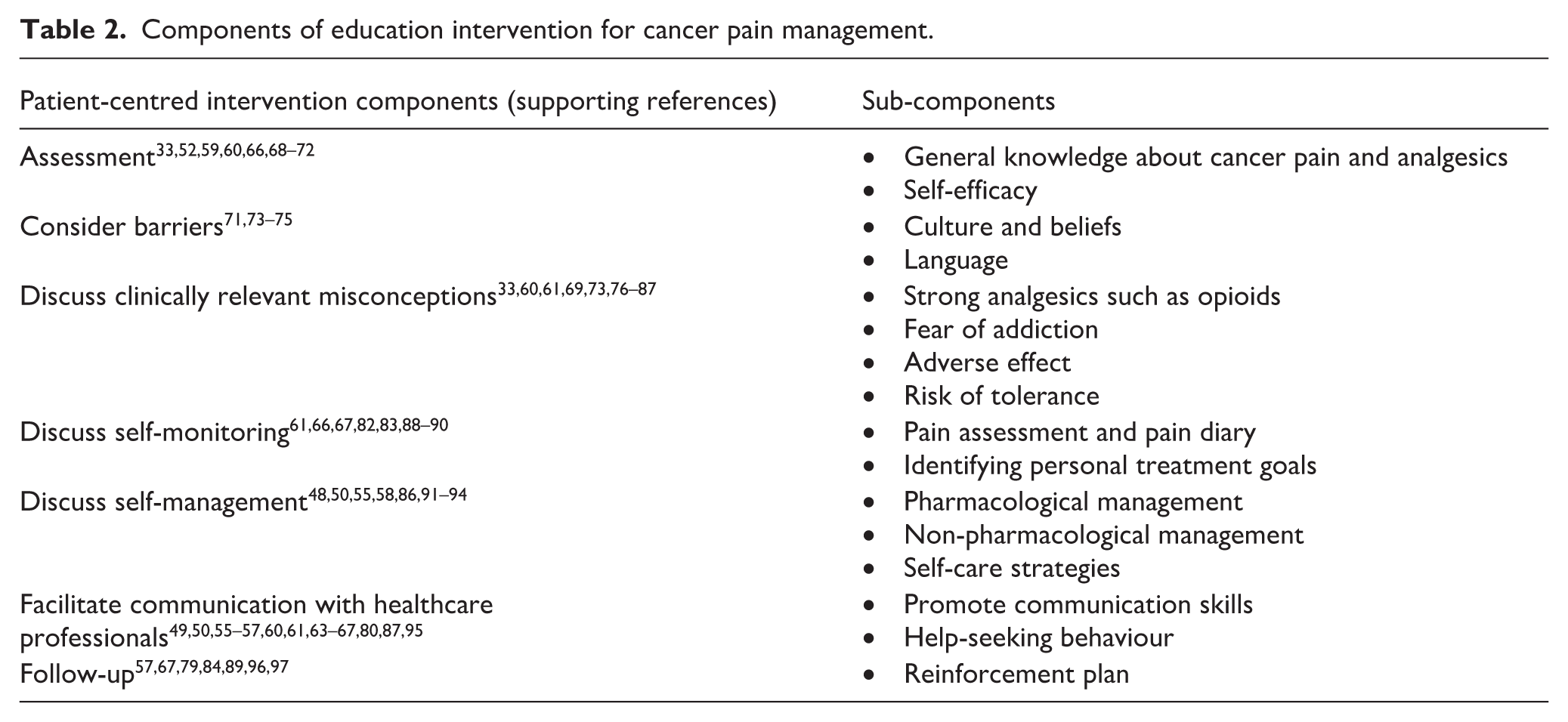
Addressing potential barriers to pain control was emphasised in three studies, particularly those that focused on patients from minority ethnic populations, where factors including language, beliefs, and cultural practices were considered.71,73,74 Discussions around misconceptions about cancer pain management were frequently reported in the literature, as detailed in Table 2.33,60,61,69,73,76 –87 Specifically, misconceptions about opioid use, a well-recognised barrier to effective pain management, were frequently reported and included various dimensions, for example, fear of addiction, tolerance, and adverse effects as shown in Table 2.
To build on patients’ existing assets, 12 studies used educational interventions that incorporated self-monitoring tools (e.g. pain diaries)66,67,83,88–89 and self-management strategies, including both pharmacological and non-pharmacological approaches.48,50,55,58,86,91,92 Another fundamental component of these interventions was the facilitation of effective communication with healthcare professionals, particularly for patients when their self-management strategies proved insufficient.49,50,55 –57,60,61,63 –67,80,87,95 Furthermore, several studies highlighted the importance of follow-up to reinforce the learning process, as shown in Table 3.57,67,79,84,89,96,97 A summary of barriers and facilitators identified across studies is presented in Supplemental Material 5.
The summary of studies focused on patients from minority ethnic populations included in the systematic review.

RCT: randomised controlled trial; USA: United States; TICAA: Technology-Based Information and Coaching/Support Programme for Asian-Americans; ACS: American Cancer Society; ICC: I Can Cope.
The ethnicity not determined.
The mediators and mechanisms of action of the educational interventions
Mediators
To explore how educational interventions alleviate cancer-related pain and associated symptoms, a number of studies investigated potential mediators of this effect. For instance, Im et al. utilised Bandura’s theory of behavioural change to explain the intermediate mediator underlying symptom reduction following educational interventions. 71 In their study, patients’ attitudes, self-efficacy, and perceived barriers were examined as mediators. The results revealed that these mediators collectively accounted for significant reductions in symptoms over 3 months. Furthermore, each mediator demonstrated statistically independent effects on accompanying symptoms, suggesting that attitudes, self-efficacy, perceived barriers, and social influences likely play a mechanistic role in the efficacy of educational interventions. Likewise, Lin et al. considered reduced barriers and improved adherence to analgesics as mediators of educational interventions in cancer pain control. 84 The results of the RCT demonstrated that patients in the intervention group had significantly lower barrier scores and better adherence with a scheduled analgesic regimen compared to patients in the control group. These findings are aligned with the lower levels of worst pain intensity reported by the intervention group.
Other studies support the notion that educational interventions improve adherence to analgesics.54,99 –101 For example, Miaskowski et al. utilised the PRO-SELF programme and reported that reductions in pain intensity scores following education might be mediated by changes in the type and amount of analgesics used [e.g. opioids vs Non-Steroidal Anti-Inflammatory Drug (NSAIDs)]. 54 Similarly, Aparna et al. implemented a standardised educational intervention for cancer pain management, demonstrating a statistically significant improvement in analgesic knowledge and compliance in the intervention group. Additionally, a significant positive correlation was observed between knowledge and compliance scores, suggesting that improved knowledge contributes to better adherence. 100 Another possible mediator for increased adherence to analgesics following an educational intervention was explored by Chou and Lin, who demonstrated that patient satisfaction with pain management regimens is a significant factor influencing medication adherence. 101 Another potential mediator for cancer-related pain control following education intervention is reported to be improved management of breakthrough pain through increased use of short-acting analgesics. 33
In general, reduced barriers to pain control have been considered intermediate mediators of educational interventions in various studies and clinical settings.71,73,74,80,81 Most of these studies have used the Barrier Questionnaire, which assesses patients’ concerns about physical effects, fatalism, harmful effects, and ineffective communication—factors that can be improved through educational interventions.60,65,76,80,81,84,97,99,102,103 Increased self-efficacy has also been reported after education intervention for cancer pain control (e.g. TEC, PRO-SELF, ANtiPain).48,59 –61,85,92
Mechanism of action
Mechanisms of action refer to the overarching processes through which an intervention operates to achieve desired outcomes. 104 These processes can be illustrated using a logic model. In this review, no previous reports outlining a logic model for cancer pain management education interventions were identified in the included studies. In addition, no studies have formally investigated the mechanisms of action for education interventions targeting cancer pain management. However, it is possible to propose an initial process-oriented logic model based on the framework by Rohwer et al. 46 which is presented in Figure 2. This figure outlines the processes and pathways linking the identified patient-centred components of educational interventions to their outcomes. The initial model illustrates the transferable logic underlying cancer pain education interventions reported in the included studies, whilst also incorporating distinctive patient-centred features specifically relevant to patients from minority ethnic backgrounds.

The logic model representing different domains of educational interventions for the management of cancer-related pain.
Furthermore, the mechanisms of action for implementation strategies, such as acceptability and fidelity, 104 in education interventions for cancer pain management were also absent in the included studies.
Description of the studies focused on patients from minority ethnic backgrounds
The summary of the six studies focused on patients from minority ethnic populations is presented in Table 3. All were conducted in the United States and included Hispanic, 73 African-American,68,98 Indian-American, 74 and Asian-Americans. 71 One study compared patients from minority ethnic backgrounds with their White counterparts but did not specify the details of the ethnic groups included.(Kalauokalani, Franks and Oliver, 2007) Table 3 also describes the purpose, patient-centred components, and distinctive features of these studies.
Purpose of education interventions for patients from minority ethnic backgrounds
Although the purposes of these studies were diverse, they shared common patient-centred themes, including (i) tailored education, (ii) misconceptions, and (iii) communication as outlined below:
Tailored education: Martin et al., 98 Im et al., 71 and Hodge et al. 73 designed studies to assess the effect of a culturally tailored education intervention for cancer patients from minority ethnic populations. When developing a tailored educational programme for low-income, predominantly African-American patients with cancer, Martin et al. initially conducted a descriptive cross-sectional study with 25 cancer patients to identify educational topics from the American Cancer Society’s “I Can Cope” curriculum. 68 After asking patients how they prioritise information and stress-management needs, cancer survivors expressed a preference for topics directly related to their illness and treatment, including understanding cancer and managing pain. These findings were subsequently used by the same investigators in an RCT to evaluate the effect of a tailored education intervention on the information needs of a population of predominantly African-American patients. 98 Im et al., focused on Asian-American patients with breast cancer, examining a culturally tailored technology-based programme compared with information from the American Cancer Society website. 71 To culturally tailor the components, the modules were available in five Asian languages and included culture-specific content, with interventionists familiar with the patients’ cultures, such as a Chinese registered nurse for Chinese participants. Hodge et al. tailored an education programme for Indian-Americans, incorporating materials that were aligned with American-Indian values, symbols, and themes of health, healing practices, and spirituality. 74 American-Indian survivors also contributed to the storytelling phase of the education material.
Misconceptions: Correction of clinically relevant misconceptions about cancer-related pain treatment was a central theme in interventions devised by Anderson et al. 73 and Kalauokalani et al. 82 In Anderson et al.’s study, misconceptions about pain treatment and the importance of reporting pain and inquiring about pain relief were addressed. However, details of the themes of these misconceptions were not reported. 73 Kalauokalani et al. emphasised the importance of identifying patients’ clinically relevant misconceptions about cancer pain management, highlighting common misunderstandings such as concerns about addiction, beliefs that pain medications are ineffective, fears of being labelled a “bad” patient, worries that pain treatment may distract from cancer care, confusion about how to take analgesics, and the assumption that analgesic side effects are uncontrollable and worse than the pain. 82
Communication with healthcare professionals: Education interventions reported by two out of six minority ethnicity-focused studies emphasised improving communication with healthcare professionals and overcoming communication barriers.74,82 To enhance patients-physician communication, Kalauokalani et al. included a rehearsal of an individually scripted patient-physician dialogue about pain control in their intervention. 82 This process helped patients: (1) identify treatment goals (e.g. “I want to sleep through the night without pain”); (2) formulate questions to achieve those goals (e.g. “What pain medication lasts through the night?”); and (3) practice asking questions, discussing pain with doctors, and negotiating a pain management plan. Hodge et al., aimed to explore the cancer experience and barriers to the management of pain, depression, fatigue, and loss of function among American-Indians residing in the Southwestern United States. 74 Key strategies in this intervention included targeted rapport building and reducing communication barriers among caregivers and “Western” healthcare providers.
Mode of delivery of education interventions in minority ethnicity-focused studies
Educational interventions targeting cancer patients from minority ethnic populations incorporated a variety of delivery methods. Whilst Kalauokalani et al. 82 and Martin et al. 98 utilised only an in-person education session, other studies incorporated a combination of approaches that included videos, booklets, handouts, and in-person sessions. 73 Im et al. developed a technology-based online module for Asian-American patients, supplemented by group and one-on-one coaching sessions. 71
Distinctive features of the interventions for patients from minority ethnic populations
Aspects of interventions focused on patients from minority ethnic populations that differentiate them from other general education interventions for cancer-related pain included:
(a) Involving representatives from the same ethnicity as the patients in the development of education resources: This was one of the distinctive features of education interventions developed by Martin et al., 98 Im et al., 71 and Hodge et al. 74 in collaboration with representatives from African-American, Asian-American, and Indian-American communities, respectively.
(b) Consideration of language: Anderson et al. made use of bilingual research nurses and bilingual materials. 73 Im et al. created the modules in five different languages (English, Mandarin Chinese (traditional and simplified), Korean, and Japanese). 71
(c) Consideration of culture: In Hodge et al. study, culturally sensitive materials were aligned with American-Indian values, symbols, healing practices, and spirituality. 74 In the Im et al. trial, culturally specific contents (e.g. herbal medicine and acupuncture) were included in the education materials. In addition, intervention developers were familiar with the patients’ culture (e.g. Chinese registered nurses for Chinese participants). 71
Effectiveness of education interventions in minority ethnicity-focused studies
Due to the heterogeneity of outcome measures and components of the educational interventions, a quantitative meta-analysis was not feasible. However, the included studies demonstrated varied results, ranging from no statistically significant effect on cancer-related pain compared to controls73,98 to significant improvements in pain and knowledge about pain management71,74 as shown in Table 3.
More specifically, Anderson et al. identified that a 20-min educational programme reduced the worst pain ratings from baseline to the first follow-up among African-American patients. 73 However, the brief nature of this intervention highlights the need for extended patient education in future studies. Kalauokalani et al. examined the effects of educational interventions among minority ethnic patients compared to their White counterparts, identifying that the interventions significantly reduced pain in both groups and helped diminish racial/ethnic disparities in pain control. 82 A limitation of this study was that all participants were English-speaking adults, preventing an assessment of language barriers.
In the trial by Im et al., significant reductions in pain and symptoms were observed over time in both the intervention group (who received culturally tailored education) and the control group (who received generic education from the American Cancer Society website). 71 However, the intervention group experienced greater reductions in physical symptom distress scores compared to the control group. Additionally, improvements in attitudes, self-efficacy, barriers, and social influence collectively accounted for significant decreases in symptoms. Unlike Kalauokalani et al., 82 this study primarily included non-English-speaking patients (82.6%) living in the United States, emphasising the role of tailored education in the presence of language barriers.
Following a tailored educational programme for Indian-American patients, Hodge et al. 74 demonstrated statistically significant improvements in knowledge about managing symptoms, including pain, depression, fatigue, and loss of function. However, pain intensity and cancer-related symptoms were not measured in this study. Therefore, the intervention’s effect on symptom control remains unknown.
Overall, the purposes and distinctive features of interventions focused on patients from minority ethnic populations demonstrate promising results in cancer pain control. These studies provide evidence that improving knowledge, correcting misconceptions, enhancing patient-physician communication, and promoting self-monitoring—when done with consideration for language and culture—can have a positive effect on pain outcomes. However, this evidence derives from studies conducted in the United States, and therefore, an evidence gap remains regarding the components and distinctive features of educational interventions suitable for patients from minority ethnic populations in other countries.
Description of studies that did not focus on ethnicity
Of the 62 studies reviewed, eight focused on cancer pain education and included patient ethnicity in their findings, summarised in Supplemental Material 6. Whilst 48 studies did not report participants’ ethnicity, they still offer valuable insights into the components, processes, and mechanisms of educational interventions for cancer pain management, applicable to all patients, including those from minority ethnic populations. These studies were categorised as either qualitative, exploring patients’ and caregivers’ experiences, or quantitative, evaluating the effectiveness of the interventions.
Discussion
This mixed-method systematic review of 62 studies represents the first comprehensive attempt to identify and synthesise evidence on educational approaches for cancer pain management and to assess their relevance to patients from minority ethnic populations. The review includes both studies specifically targeting patients from minority ethnic backgrounds and more general educational interventions, the latter of which offer valuable transferable patient-centred insights that may inform culturally appropriate approaches for these populations.
We identified the components of the educational interventions and studied potential direct and intermediate effects that led, in some studies, to effective cancer pain control and symptom improvement. Current evidence suggests that the development of educational interventions focuses on knowledge improvement, correction of misconceptions, communication, and self-monitoring to empower patients. Our findings support the importance of tailored education in cancer-related pain management for both the general population and minority ethnic communities. This aligns with Mead and Bower’s 105 comprehensive framework of patient-centred care, which was applied by Luckett et al. 106 to cancer pain self-management, highlighting the importance of promoting self-assessment and individualised pain management to empower each patient and their family within the context of their priorities, preferences, and daily lives. 106 The key features of the interventions tailored for patients from minority ethnic populations included the provision of educational materials in multiple languages, the incorporation of culturally safe and sensitive content, and reducing communication barriers with healthcare professionals.
The logic model of educational interventions for the management of cancer-related pain
The components of the educational interventions, patients’ experiences, along with the direct and intermediate effects leading to pain control, are summarised in a process-oriented logic model guided by Rohwer et al. 46 As shown in Figure 2, the logic model comprises seven intervention components and a number of direct and intermediate effects that portray the underlying processes associated with the intended outcomes. In summary, assessing patients’ general knowledge about cancer pain and analgesics is a common component in most studies included in this systematic review. This requires particular attention to misconceptions and common barriers to cancer pain management. 14 In addition, cultural factors are considered by incorporating materials that reflect patients’ beliefs and practices. 74 This is particularly important for patients from minority ethnic populations in multicultural societies, as reflected in six minority ethnic-focused studies.68,71,73,74,98 The findings of this review suggest that reference to cultural values, symbols, and spirituality can be successfully incorporated into educational interventions.71,74 This can be achieved by adopting co-creative approaches that respect patients’ values and avoid imposing dominant cultural perceptions. Common barriers and facilitators identified across studies (Supplemental Material 5) highlight the importance of addressing communication challenges, cultural beliefs, and patient self-efficacy when developing educational interventions.
Facilitating patients in communicating with their healthcare team, as well as follow-up and reinforcement of learning, are other critical components of patient education for cancer pain management.57,67,79,84,89,96,97 Self-monitoring, facilitated by tools including pain diaries, enables patients to identify their issues and set personal treatment goals.66,67,83,88,89
This systematic review identified evidence of the processes that link the above components to cancer pain control. A key mediator identified by this review represents empowering patients to take an active role in their treatment, enhancing their confidence throughout the process.48,51 –59 This may be achieved by addressing barriers to pain control, improving self-efficacy, and fostering positive attitudes towards treatment options. The current evidence suggests that these factors are associated with improved adherence to prescribed analgesics and greater patient satisfaction with their treatment.54,99 –101 Another important aspect of effective educational interventions is promoting communication, enabling patients to confidently request assistance when needed. Overall, this approach encourages greater patient involvement in their care, leading to improved pain and symptom management, as well as enhanced quality of life (Figure 2).
Generalizability of the existing education interventions in minority ethnic populations
Given that only a small number of studies were identified in this review specifically focused on patients from minority ethnic populations, and of these, all were conducted in the United States, we question to what extent they may be relevant to patients from minority ethnic populations in other geographical settings in the absence of necessary acceptability and feasibility testing. This is because educational interventions were bespoke, largely tailored to the needs of patients from a specific ethnic group. However, these studies still provide important distinctive features that may usefully guide the development of future educational interventions for patients from minority ethnic populations in other settings. For example, involving representatives from the same ethnicity as the patients in the development of educational resources is suggested.71,74,98 This “emic” as opposed to “etic” approach may facilitate a more effective cultural modification of existing interventions (e.g. PEP and PRO-SELF) by addressing culturally sensitive issues that healthcare professionals might otherwise not be aware of. Since overcoming communication barriers is key to the effectiveness of interventions, minority ethnic-focused studies, as suggested by Kalauokalani et al., incorporate rehearsing scripted patient-physician dialogues about pain control, identifying treatment goals, and formulating questions to achieve those goals. 82
Addressing communication barriers also involves considering the language and the ability to deliver education in a way that is accessible to patients and their caregivers from different minority ethnic populations. Whilst some educational interventions for cancer pain, PEP and PRO-SELF have been translated into different languages57,58,64 they have not been specifically studied among patients from minority ethnic populations. Given the comprehensive nature of these interventions, it seems reasonable to suggest that these resources could be tailored to minority ethnic groups by incorporating the distinctive features mentioned above. However, this will require further research to explore the specific needs of patients from minority ethnic populations, involving patients, caregivers, and healthcare professionals.
Whilst our review focused specifically on cancer pain interventions that explicitly aimed to be culturally tailored, we acknowledge that broader patient education or pain management interventions may contain elements relevant to minoritised ethnic groups, even if not labelled as such. These interventions may offer useful insights into transferable mechanisms of action or engagement strategies.
Strengths and limitations of this review
The strength of this mixed-methods systematic review lies in encompassing all studies utilising educational interventions for cancer-related pain management. It involved appraising 62 primary studies, including 8154 patients, 666 of whom participated in studies focused on those from minority ethnic backgrounds. It also involved the inclusion of both quantitative and qualitative studies on patient-centred educational interventions for cancer-related pain management. This approach provided deeper insights into the identification of components and mediators of cancer pain education interventions (Table 3 and Figure 2).
However, this study also has limitations that limit the inferences that can be made from the findings. First, whilst the focus of this review was on cancer pain education interventions and their relevance to patients from minority ethnic backgrounds, we are cognizant of the relative dearth of interventions, largely US-based, that focused on minority ethnic backgrounds. This does not reflect the impact of increased globalisation in many more countries, where patients increasingly reflect identities, backgrounds, and heritages different from those caring for them. This limitation speaks to the absence, wilful or inadvertent, of minority ethnic populations in intervention development and evaluation.107,108
We did not conduct a meta-analysis due to the heterogeneity of populations, outcomes, and interventions. Instead, our review employed a data-based convergent design and a narrative synthesis rather than quantitative pooling. To assess the quality of each study, the QualSyst tool was applied; this aligns with guidance for mixed-methods systematic reviews and has been widely adopted in reviews integrating heterogeneous evidence. The tool enabled us to evaluate internal validity, transparency of data collection, and analytical rigour whilst maintaining parity across methodological types. 42 Consequently, multiple risk-of-bias frameworks (e.g. Cochrane for quantitative studies and GRADE-CERQual for qualitative evidence synthesis) were not used, as each framework has differing assumptions about study design, and their use would have introduced inconsistency and reduced feasibility without improving interpretive validity. Whilst the focus of this review was on cancer pain education interventions and their relevance to patients from minority ethnic backgrounds, the number of studies specifically addressing these populations was limited, and all were conducted in the United States. This limited pool of studies does not reflect the impact of increased globalisation in many more countries, where patients increasingly reflect identities, backgrounds, and heritages different from those caring for them. Moreover, the terminology used to describe ethnic groups varied across regions. For instance, in the United States, “Asian” often refers to people of East and Southeast Asian origin, whereas in the United Kingdom, it typically refers to individuals of South Asian descent, including those from India, Pakistan, Bangladesh, and Sri Lanka. 109 Within the context of this systematic review, since all ethnically focused studies were conducted in the United States, the term “Asian” refers to individuals of East and Southeast Asian origin. A similar inconsistency exists in the terminology used to describe Indigenous populations within the American continent. In the study conducted in the United States, the term “Indian-American” was used, 74 whereas other countries may use terms such as “Indigenous peoples” or “First Nations peoples.” We chose to retain the original terminology to remain faithful to the source material. However, this inconsistency highlights the complexity of comparing and generalising findings across studies. Thus, the harmonisation of terminology in research on minority ethnic and Indigenous communities warrants further collaborative efforts among researchers that include patient and public involvement to ensure studies are authentically grounded in the lived realities of patients.110,111
Another limitation of the review is its exclusive focus on patient-centred education, with insufficient consideration of the contributions of other stakeholders in the education process. Among the studies included, there are only two that addressed education for informal carers, involving a total of 238 caregiver participants.48,77 Informal carers play a crucial role in supporting and communicating with patients, particularly in minority ethnic communities, where language and cultural barriers pose additional challenges in caring for individuals with cancer.48,52 Similarly, the role of healthcare professionals, their perspectives, knowledge, and training, was not comprehensively explored in this systematic review. It is reasonable to suggest that educators (healthcare professionals) should have access to appropriate educational resources covering the key components, common misconceptions, barriers to educational interventions, as well as cultural competency and cultural safety.112,113 This important aspect was largely overlooked in the included studies. Only one report in the included studies examined the experiences of physical therapists in the context of cancer pain management. 50 This limitation of the systematic review highlights the need for an alternative search strategy to better address educational training for healthcare professionals in future research.
In this systematic review, only primary research studies were included. However, educational intervention resources are not limited to published literature in peer-reviewed journals. Local, national, and international clinical guidelines, audits, and online surveys may also provide information relevant to cancer-related pain education. For example, Luckett et al. utilised a national online survey of current practice, a desktop review of online patient pain diaries, and other related resources to develop a cancer pain self-management resource addressing patient, provider, and health system barriers. 22 Their findings align with the components identified in the present systematic review by encouraging self-monitoring, building patients’ sense of control, and supporting communication with healthcare professionals. 22
Whilst several included studies 114 suggest that cultural and socioeconomic contexts shape patients’ understanding and communication of pain, yet these were seldom analysed through an intersectional lens, this systematic review did not specifically explore the impact of intersectional factors on cancer pain education interventions. 115 Whilst these factors are known to influence pain assessment and management (e.g. social determinants of health), 114 they were not addressed in the majority of studies included in this review and thus warrant further investigation. Future research should explicitly examine how social determinants, such as income, education, and migration status, interact with ethnicity to influence engagement with cancer pain education. 111
Additionally, this review highlights a significant gap in the literature concerning cancer pain management in minority ethnic populations from a strengths or assets-based perspective.38,116 This approach acknowledges that individuals from minority and often marginalised communities may nonetheless possess valuable human capital and community assets that they draw upon during health crises that may include experiencing cancer pain. 23 Further research is needed to examine this complex and highly nuanced area in greater depth, with particular attention to the role of cultural healing practices, the influence of community-based social support networks, 117 religious beliefs, and the presence of faith, 118 the need to educate healthcare providers about the strengths embedded within these communities. 112
Implications for clinical practice
Consequent to globalisation, healthcare systems are more frequently required to provide care to individuals from minority ethnic backgrounds who may hold differing health beliefs, symptom attributions, and preferred solutions than their clinicians. This is occurring in contexts where professional cultural safety and cultural literacy have often been insufficiently prioritised, and where patients may not always feel respected, valued, or protected from cultural harm. 119 A lack of attention to power dynamics and institutional biases can inadvertently lead to misunderstandings and create barriers in interactions between patients and clinicians from different cultural backgrounds. 120 Promoting cultural safety through collaboration and engagement with minority ethnic communities fosters trust and may help dispel misconceptions.119,121 –123
Clinicians should be aware that addressing culturally patterned or shaped misconceptions can enhance adherence to analgesic regimens.54,99 –101 Ultimately, improved communication between clinicians and patients empowers individuals to seek help when routine pharmacological and non-pharmacological therapies are ineffective.
This review identified key components of effective educational interventions for cancer pain management that can support clinicians in delivering more responsive care to patients from minority ethnic communities, as shown in Table 3. The interventions emphasised the importance of patient-centred assessment by healthcare teams, which facilitates the planning of personalised education tailored to individual needs. Such approaches include avoiding overly complex explanations, offering clear treatment options, and addressing cultural and language barriers through the development of culturally sensitive and translated educational materials.
Implications for research
This systematic review highlights significant gaps in knowledge regarding interventions for cancer-related pain for patients from minority ethnic populations. Future studies are required in multicultural societies, particularly outside the United States, where the knowledge gap is currently evident. Second, studies focused on patients from minority ethnic populations have predominantly been quantitative emphasising the development and effectiveness of interventions. Robust qualitative studies are also essential for exploring the perspectives and lived experiences of patients from minority ethnic populations regarding cancer pain management. Future investigations should address this, incorporating input from all stakeholders, including informal caregivers and healthcare professionals. Future primary research on cancer pain education that explicitly employs Indigenous research methodologies should be explored to ensure data sovereignty and cultural relevance.
The logic model presented in this review serves as an initial framework that requires further refinement, particularly through the incorporation of lived experiences. Specifically, it provides a provisional framework that future qualitative studies should use to explore the lived experiences of family caregivers to ensure the “Facilitation with Healthcare Professionals” component is fully culturally inclusive. To achieve this, research should prioritise effective educational interventions assessed within minority ethnic populations. Utilising established cancer PEPs, such as PRO-SELF and PEP, across different languages and cultural contexts may enhance their relevance and applicability for these patients from these populations. For instance, the German and Norwegian versions of PRO-SELF48,55,56 and the Taiwanese version of PEP 64 have already been used successfully; this list can be expanded to encompass additional languages. Whilst these translations are primarily directed towards patients from the majority population rather than specifically addressing those from minority ethnic groups, future efforts should focus on translating and delivering these interventions in a broader range of languages beyond those currently available.
Conclusion
Pain is a common symptom in patients with cancer, but with effective management, it can significantly improve their quality of life. Despite this, evidence reveals ethnic disparities in the assessment and management of cancer pain.18,21,124 –127 This systematic review identified the key patient-centred intervention components and mechanisms of educational interventions for cancer pain management relevant to patients from minority ethnic groups. Drawing on both qualitative and quantitative studies, the findings highlight the importance of tailoring educational interventions to address the needs of patients from minority ethnic backgrounds to optimise cancer-related pain management within minority ethnic communities. Current evidence indicates that educational interventions should focus on improving knowledge, correcting misconceptions, enhancing communication, and promoting self-monitoring to empower patients. Culturally focused interventions stand out for their inclusion of educational materials in multiple languages, 128 incorporation of culturally sensitive content, and efforts to reduce communication barriers with healthcare providers.
These goals can be achieved by involving community representatives from the same ethnic backgrounds as the patients in the development of educational resources and by assessing patients’ specific needs. 108 However, further research is necessary to determine the most effective strategies for creating these interventions and reducing existing disparities in pain management within minority ethnic populations. The logic model developed in this review requires further refinement through rigorous qualitative research, incorporating input from multiple stakeholders, patients, their unpaid carers, and clinicians.
Supplemental Material
sj-docx-1-pcr-10.1177_26323524261421936 – Supplemental material for Patient-centred educational interventions for assessing and managing cancer-related pain relevant to minority ethnic populations: A mixed-methods systematic review
Supplemental material, sj-docx-1-pcr-10.1177_26323524261421936 for Patient-centred educational interventions for assessing and managing cancer-related pain relevant to minority ethnic populations: A mixed-methods systematic review by Tara Dehpour, Donna Wakefield, Tim Luckett, Jamilla Hussain and Jonathan Koffman in Palliative Care and Social Practice
Supplemental Material
sj-docx-3-pcr-10.1177_26323524261421936 – Supplemental material for Patient-centred educational interventions for assessing and managing cancer-related pain relevant to minority ethnic populations: A mixed-methods systematic review
Supplemental material, sj-docx-3-pcr-10.1177_26323524261421936 for Patient-centred educational interventions for assessing and managing cancer-related pain relevant to minority ethnic populations: A mixed-methods systematic review by Tara Dehpour, Donna Wakefield, Tim Luckett, Jamilla Hussain and Jonathan Koffman in Palliative Care and Social Practice
Supplemental Material
sj-docx-4-pcr-10.1177_26323524261421936 – Supplemental material for Patient-centred educational interventions for assessing and managing cancer-related pain relevant to minority ethnic populations: A mixed-methods systematic review
Supplemental material, sj-docx-4-pcr-10.1177_26323524261421936 for Patient-centred educational interventions for assessing and managing cancer-related pain relevant to minority ethnic populations: A mixed-methods systematic review by Tara Dehpour, Donna Wakefield, Tim Luckett, Jamilla Hussain and Jonathan Koffman in Palliative Care and Social Practice
Supplemental Material
sj-docx-5-pcr-10.1177_26323524261421936 – Supplemental material for Patient-centred educational interventions for assessing and managing cancer-related pain relevant to minority ethnic populations: A mixed-methods systematic review
Supplemental material, sj-docx-5-pcr-10.1177_26323524261421936 for Patient-centred educational interventions for assessing and managing cancer-related pain relevant to minority ethnic populations: A mixed-methods systematic review by Tara Dehpour, Donna Wakefield, Tim Luckett, Jamilla Hussain and Jonathan Koffman in Palliative Care and Social Practice
Supplemental Material
sj-docx-6-pcr-10.1177_26323524261421936 – Supplemental material for Patient-centred educational interventions for assessing and managing cancer-related pain relevant to minority ethnic populations: A mixed-methods systematic review
Supplemental material, sj-docx-6-pcr-10.1177_26323524261421936 for Patient-centred educational interventions for assessing and managing cancer-related pain relevant to minority ethnic populations: A mixed-methods systematic review by Tara Dehpour, Donna Wakefield, Tim Luckett, Jamilla Hussain and Jonathan Koffman in Palliative Care and Social Practice
Supplemental Material
sj-xlsx-2-pcr-10.1177_26323524261421936 – Supplemental material for Patient-centred educational interventions for assessing and managing cancer-related pain relevant to minority ethnic populations: A mixed-methods systematic review
Supplemental material, sj-xlsx-2-pcr-10.1177_26323524261421936 for Patient-centred educational interventions for assessing and managing cancer-related pain relevant to minority ethnic populations: A mixed-methods systematic review by Tara Dehpour, Donna Wakefield, Tim Luckett, Jamilla Hussain and Jonathan Koffman in Palliative Care and Social Practice
Footnotes
Acknowledgements
This study is supported in part by the National Institute for Health and Care Research Applied Research Collaboration for Yorkshire and Humber [NIHR200166]. The views expressed are those of the author(s), and not necessarily those of the NHS, the NIHR, or the Department of Health and Social Care.
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This publication is independent research funded by the National Institute for Health and Care Research, Yorkshire and Humber Applied Research Collaborations, NIHR200166.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Any other information in this review is available from the corresponding author upon request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.