
Abstract
Background
Telerehabilitation (TR), a branch of telemedicine, provides remote therapeutic rehabilitation through telecommunication. Driven by technological advances and benefits like remote monitoring and patient education, it has grown since 1998. The Coronavirus Disease 2019 (COVID-19) pandemic highlighted its importance in maintaining healthcare access.
Research question
What is the efficacy of TR compared to in-person rehabilitation? Are the assessment tools effective? Is TR well-accepted, and are costs reduced?
Methods
A bibliographic search on Medline, Cochrane and Google Scholar focused on systematic reviews (SRs) from 2014 to Mai 2024, comparing TR or home-based rehabilitation with in person treatments for various conditions. Independent reviewers conducted initial screenings, resolving disagreements by a third reviewer. Joanna Briggs Institute Critical Appraisal Checklist was used to evaluate the quality of review. The data was synthesised narratively.
Results
The search identified 665 SRs. After selection, 228 SR were included. TR models include synchronous (real-time video interactions), asynchronous (independent sessions through digital platforms) and mixed methods. Regardless of the medical fields, the conclusions of the SRs consistently point to the equivalence of TR compared to in-person rehabilitation. Remote evaluations via digital tools were reliable and valid for various assessments. TR is cost effectiveness and well accepted.
Conclusions
TR is a viable alternative or complement to traditional rehabilitation, offering enhanced accessibility, reduced costs and improved results. Barriers include technical issues, training and concerns about lack of physical contact. Mixed methods could address these challenges.
Background
Telerehabilitation (TR), as defined in the Mesh (Medical Subject Headings) directory, encompasses the remote delivery of therapeutic rehabilitation through telecommunication technologies.
1
This specialised branch of telemedicine has emerged relatively recently, with its inaugural scientific discourse traced back to 1998.
2
The advent of the 21st century witnessed a surge in TR programs, attributed to heightened awareness of its potential benefits and concurrent advancements in technology, fostering the establishment of dependable rehabilitation services. These services extend to encompass remote monitoring of rehabilitation progress, adjustment of rehabilitation protocols from a distance, as well as education and training initiatives targeted at families and healthcare professionals.3–5 By 2008, scholarly literature attributed the capability of TR to:
Facilitate healthcare services in remote or underserved regions.
6
Broaden rehabilitation horizons through computer-assisted systems.
7
Enhance quality of life.
8
Mitigate medical expenses by accommodating a larger number of patients within a given timeframe.9,10 Reduce travel requirements.
9
The subsequent decade witnessed an exponential expansion of telemedicine applications, propelled by advancements in computer technologies, widespread deployment of high-speed networks and the refinement of telemedicine apparatus. Contemporary telecommunication modalities encompass video conferencing, email correspondence and text messaging, alongside the capacity for remote manipulation of robots, robotic appendages. These technological strides have profoundly reshaped human interactions.
10
Concurrent demographic shifts and augmented public health budgets have catalysed the emergence of novel rehabilitation paradigms.
11
Lastly, the Coronavirus Disease 2019 (COVID-19) pandemic in 2020 has placed a stronger emphasis on telemedicine and TR in healthcare worldwide. 12 Throughout the pandemic, this modality has demonstrated its capacity to facilitate access to healthcare services and improve care continuity, irrespective of geographic location, with substantial potential in terms of time and resource savings.11,13–15
In the healthcare pathway of a patient requiring the intervention of a rehabilitator, alongside medical and curative care, the patient is managed in a post-acute care facility or in a private practice for the following purposes (Ministry of Health, France):
To regain the best possible physical, cognitive and psychological function. The goal is to fully restore the impaired function or optimise its capacity. This is rehabilitation. To support the patient if limitations in their abilities prove to be irreversible. The aim is to enable the patient to adapt as best as possible to these limitations and find ways to overcome them. This is re-adaptation. To go beyond medical care and ensure real autonomy for the patient – in their family and professional life – allowing them to regain the living conditions they had before their hospital stay. This is reintegration.
Each of these stages is configured as an iterative process, involving a series of loops that combine assessments, clinical decisions and interventions. These processes actively involve patients, healthcare professionals and caregivers. In this context, TR emerges as an emerging solution, deploying tools tailored to each of these rehabilitation stages and each of the actors involved. Barack and Klein categorised them into six categories: Internet-based educational interventions, self-help therapeutic interventions on the Internet, therapeutic interventions on the Internet with face-to-face components, online counselling, therapeutic software operated on the Internet and other online activities.
16
Each category of Internet-based intervention is described based on four major elements: (a) content (e.g. educational or behaviour modification), (b) multimedia (e.g. text, images and videos), (c) online interactive activities (e.g. online quizzes, assignments) and (d) guidance and feedback (e.g. automatic reminders, professional feedback).
Despite this observation, clinicians face several questions in their decision-making process regarding the implementation of these devices. What are the expected effects compared to face-to-face treatments What are the most relevant forms of TR? What are the clinimetric values of evaluation tools?
The answers to these questions could be crucial in the planning of services and the development of rehabilitation centres. The results of this study could provide insights into determining the role of TR in conjunction with inpatient services, either as an alternative to in-person care or as a means to extend and follow up on rehabilitation efforts.
The objective of this review of systematic review (SR) is to provide an overview of TR, including the types of TR and associated technical requirements, expected effects, the clinical value of assessment tools and the role of family caregivers in these remote interventions. To address the question of development areas in rehabilitation centres, we processed the responses as follows:
What models are used in TR? How is the patient's evaluation performed? What is the acceptance of TR and what are the determining factors? What is the efficacy of TR? What is the cost-efficiency ratio of these systems?
Method
Search strategy
A bibliographic search was conducted on Medline, Cochrane and Google Scholar, initially using the keyword ‘telerehabilitation’. Given the abundant literature, we have chosen to focus solely on SRs.
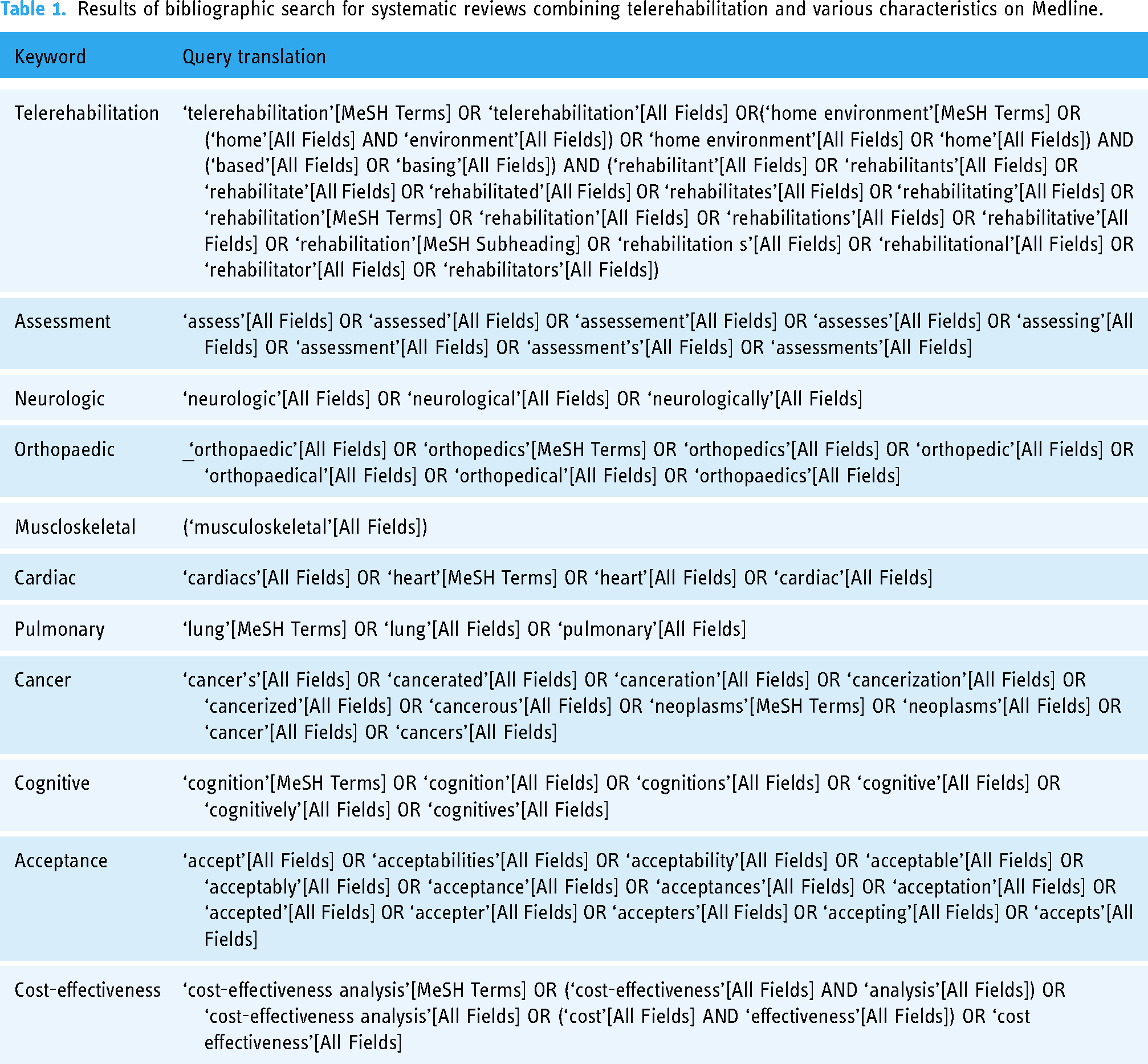
The SR filter was applied (Table 1). The search criteria range from 2009 to Mai 2024.
Results of bibliographic search for systematic reviews combining telerehabilitation and various characteristics on Medline.
Inclusion and exclusion criteria
All SRs were included to evaluate the benefits obtained with the physiotherapy treatment administered. Outcomes varied depending on the diseases and the studied population. Participants in the studies could be adolescents (under 18 years of age), adults (over 18 years of age) and senior citizens (over 65 years of age). All types of interventions were considered. Intervention treatment was defined as physiotherapy administered remotely through the use of web technology with the aid of a smartphone, videoconferencing, application or other similar tools. Standard physiotherapy was understood as the face-to-face administration of physiotherapy treatment with physical contact between the physical therapist and the patient. All SRs were included, regardless of whether they used the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) methodology or not.
Data extraction
Two independent reviewers (PP, BF) carried out the initial screening of titles and abstracts (to exclude papers that were definitely ineligible), followed by a detailed full-text screening of the remaining papers (to exclude papers not meeting all inclusion criteria, with reasons for exclusion recorded). Any disagreements between the reviewers were resolved with the help of a third reviewer.
Summarizing and collating the data
The general, methodological and results/outcomes of the included studies were analysed using narrative synthesis to summarise and explain the findings.
Articles have been evaluated using the Joanna Briggs Institute (JBI) Critical Appraisal Checklist for SRs 17 and research synthesis. A particular emphasis was placed on the bias analysis tools used in the reviews.
Results
Selection of articles
The literature on TR is extensive, producing no fewer than 8890 responses on Medline without filters as of 30 July 2024, including 665 SRs. Based on title and abstract, the following were excluded: non-SRs, SRs related to paediatric rehabilitation and studies that did not focus on either TR or home-based rehabilitation. In total, 232 full-text articles were analysed and five duplicates were detected.
In the end, 228 articles were included in the study (Figure 1). Each review was then categorised into one of the following categories: neurology, orthopaedics, respiratory, cardiac, cognitive, cancer, elderly, cost-effectiveness, acceptance and determining factors, assessment and global. After duplicates were identified (five articles), a total of 228 articles, encompassing 3418 clinical studies, were analysed. The list of articles is compiled into 11 tables by category in Appendix 1. All bibliographic references are in Appendix 2.
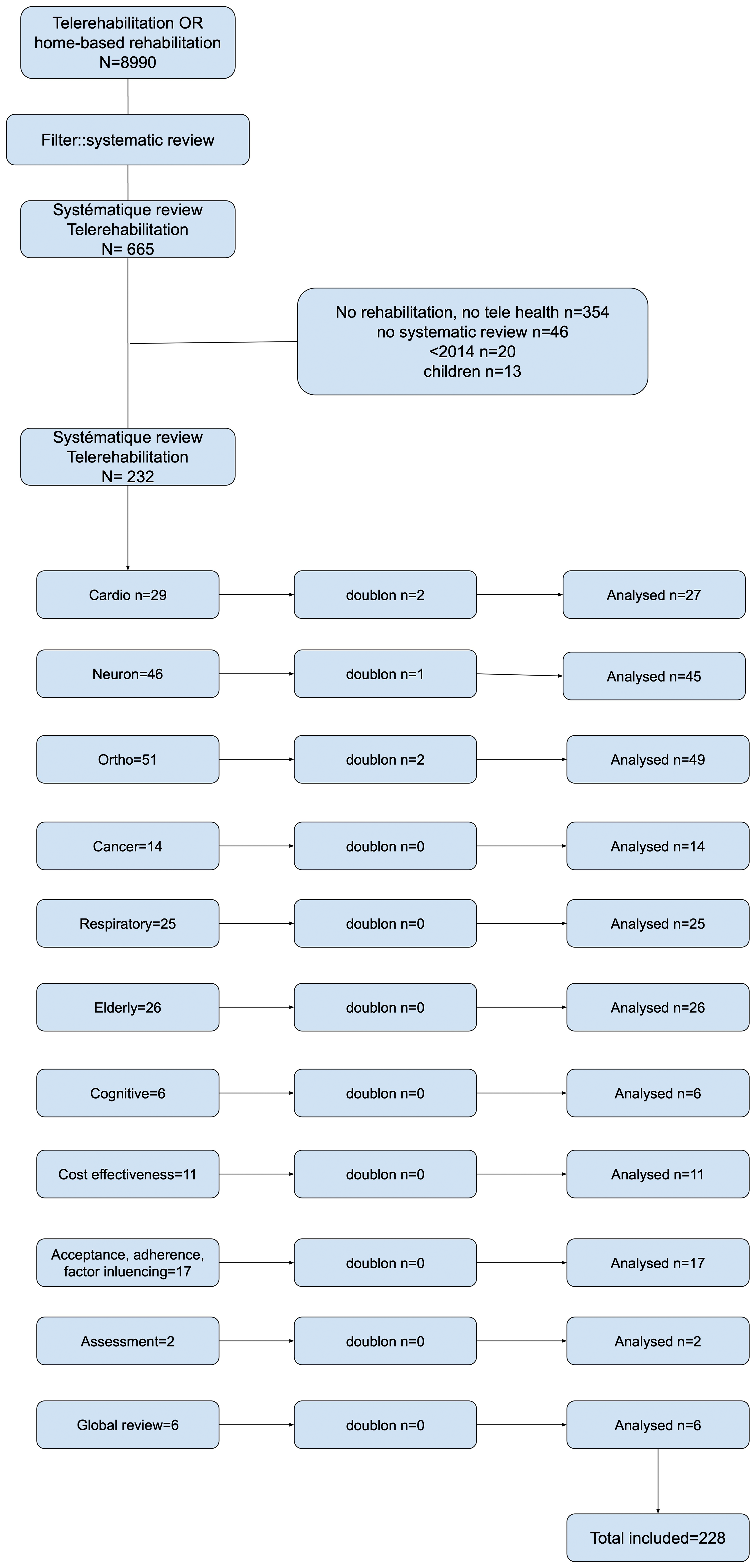
Reporting items for systematic reviews flow diagram of the study selection process.
Overall, a large majority of the studies exhibit adequate methodological quality a well-justified selection of clinical studies. The subject of TR has been addressed in all areas of rehabilitation, and the number of SR has increased significantly in the last 3 years. The results are presented in the order of the questions asked, (a) models used in TR, (b) patient evaluation, (c) acceptance and determining factors, (d) efficacy and (e) cost efficiency.
To inform the discussion and address the various research questions, an exploration of the clinical studies selected in the SRs was conducted to retrieve source data and details of the interventions.
Evaluation of study quality
The bias analysis tools used in the various reviews were identified. They are reported in the tables of Appendix 1.
Ninety-six SRs used Cochrane's Risk of Bias tool, 38 used the Physiotherapy Evidence Database (PEDro) scale, one study combined both tools, four used the Tool for Study quality assessment and reporting in Exercise (TESTEX), four used the JBI Critical Appraisal Checklist, four used the Grading of Recommendation, Evaluation, Development and Evaluation, three did not comply with recommendations, and 44 studies did not present specific bias analysis tools. The remaining reviews used tools more specific to their subject, such as the Consolidated Health Economic Evaluation Reporting Standards 2022 checklist for cost-related studies, the COnsensus-based Standards for the selection of health Measurement INstruments (COSMIN) checklist or the Quality Measurement Checklist for reviews focussing on evaluation.
Intervention models
Various TR models have been implemented globally. 18
Synchronous and asynchronous modes
The internet has the potential to become an effective instrument for large-scale healthcare interventions to promote self-management and chronic disease prevention. 19 Synchronous interventions involve patients being individually or collectively accompanied by therapists in real-time through video conferferencing, 20 as opposed to asynchronous interventions, which consist of digital-format sessions performed independently by the patient. 21 The development of innovative technologies has enabled the integration of important features to facilitate and optimise asynchronous care delivery. 22 Initially, simple implantation of exercise program platforms configured by rehabilitation professionals was made available to patients (e.g. Axomove©, kinexer6©). Subsequently, motion tracking systems were integrated to provide real-time biofeedback during exercise, incorporating various technologies such as wearable sensors with inertial measurement units, sensors embedded in smartphones and camera-based sensors. 23 These technologies guide patients during sessions, allowing remote close monitoring of patient progress, providing individualised support and enhancing accountability. 24 Furthermore, digitizing movements with corresponding data storage on web platforms can assist therapists in monitoring patients and adjusting interventions based on data. In some recent systems, artificial intelligence can analyse real-time feedback and adapt exercise difficulty (e.g. neuradom© system).
On the other hand, recent research on human–machine interfaces has improved the accessibility of virtual reality, 25 which can be used synchronously or asynchronously. However, remote devices remain non-immersive.26–28 Although Head Mounted Display systems offer a much more engaging and sensory impactful immersive experience, 28 with superior effects, 29 patient safety, cost and connectivity issues hinder their remote use. Platforms such as XRHealth clinics (https://www.xr.health/) offer remote rehabilitation programs characterised by semi-autonomy, supervised by health professionals.
Mixed modes (TR and in-person)
The combination of face-to-face and online or computer-based platforms is increasingly utilised in healthcare. 30 As a strategy, the combination of these approaches is known as ‘mixed rehabilitation’ or ‘blended learning’. 31 Mixed therapy, combining the use of an interactive resistance training program on a tablet with face-to-face therapy sessions, is feasible and safe, with high participant acceptance. 32 Another study shows that satisfaction, system ease of use and treatment adherence were high in patients treated for depression, with clinically effective outcomes. 33 In chronic disease self-management programs that combine face-to-face and online/computer-based educational interventions to improve knowledge and induce behaviour changes leading to effective self-management practices, it is shown that the most effective and well-received treatment plans rely on subjective and objective assessments of patient needs and the use of age-appropriate tools. 34 For example, Morsa et al. suggest that young adults with chronic diseases may be receptive to educational strategies involving role-playing. 35 In general, the results of mixed methods depend on healthcare professionals’ adaptation to digital tools and their non-traditional role. When the focus was explicitly on training healthcare providers to administer mixed interventions, improvements in patient outcomes were observed. 36 Therefore, it is important to enable healthcare professionals to acquire specific knowledge in the virtual environment. 38 Furthermore, the TR environment continues to evolve. Therefore, it is important to incorporate new evidence and advancements in the ethical, administrative, clinical and technical aspects of TR. 37
Assessment model
Two SRs have identified assessment tools suitable for use in TR.38,39 In neurology, 22 tools exhibit sufficient psychometric properties and are considered appropriate for use. However, in the musculoskeletal field, special orthopaedic tests, posture analyses and neurodynamic tests present challenges for remote implementation. More specifically, there are several modalities for patient evaluation: the use of a third-party caregiver capable of replicating tests, the use of traditional tests modified for self-administration, 40 the use of connected devices or the collection of declarative information on web platforms. In all cases, before conducting the tests, clinicians must consider whether the chosen tests have good quality clinical measurement properties and if they are validated for an online environment. 40
Assessment by remote caregiver
In the orthopaedic field, typical assessments include evaluating joint range of motion, assessing gait and manual dexterity, testing motor control, strength and endurance, analysing postures and determining functional capacities.
For joint range of motion measurements, studies show good reliability and validity of data when measurements are taken by a professional accompanying the patient and remotely directed. 41 Regarding the evaluation of lumbar postures, the results appear conflicting concerning the validity and reliability of data. 42 Similarly, placing a virtual goniometer on the screen demonstrates good reliability and validity compared to actual measurements. 43 For strength, endurance and motor control, the results have demonstrated good validity in endurance (Cronbach's alpha = 0.8) and excellent validity in motor control (Cronbach's alpha = 0.97) between remote and face-to-face assessment methods. Intrarater and interrater reliability of endurance and motor control assessment based on remote evaluation was excellent (intraclass correlation coefficient > 0.90). 44 In terms of functional capacity measurements, three studies reported functional outcome measurements based on remote assessment.41,43,44 Concurrent validity between remote and face-to-face assessments showed substantial to good agreement for the Timed Up and Go test (Krippendorff's alpha = 0.86), the Tinetti test (Krippendorff's alpha = 0.79) and the Berg test (Krippendorff's alpha = 0.76) for patients undergoing total knee arthroplasty. Similarly, excellent reliability was reported for the Oswestry Disability Index (Cronbach's alpha = 0.99), the 12-item Short Form Health Survey (Cronbach's alpha = 0.97) and the Tampa Scale for Kinesiophobia (Cronbach's alpha = 0.97) in patients with low back pain. 37
According to Brito, 38 there are two TR tools that have strong evidence in the field of neurological impairments. Among these, eight tools are highly recommended due to their high quality of clinical measurement. These tools are particularly beneficial for individuals who have experienced a stroke, spinal cord injury or Alzheimer's disease.
Self-administered assessment
In a study conducted by Russel in 2010, 44 a face-to-face physical examination was performed which included various assessments such as postural evaluation, gait analysis, functional task analysis, observation and palpation of the painful area, range of motion tests, muscle strength testing, nervous system evaluation and orthopaedic tests for ligaments, joints and tendons. Patients were guided by a remote therapist to self-assess and perform specific tests. For instance, patients were asked to report pain intensity and location while performing certain movements under the guidance of the remote therapist. Computer tools were utilised by the remote therapists for measurements and patients were shown instructional videos. The results of the physical examination indicated high levels of agreement in validity and reliability studies.
Russel, 45 in another study focusing on motor impairments of the ankle, showed similar agreement of 93.3% for pathoanatomical diagnosis. Clinical observations were highly concordant (k = 0.92) for categorical data and significant (93.3% agreement; chi-square = 234.4; p < .001) for binary data. A high level of inter- and intrareference reliability was found for TR assessments. These data on self-administration of tests are corroborated in the study by Lade. 46
The Rehab@Home framework is a TR system designed for stroke patients undergoing home-based rehabilitation. Developed by Jagos in 2015, 47 the framework includes wireless instrumented insoles, a third-generation tablet, a server and a graphical web interface for medical professionals. Assessment tests are conducted on the tablet to automatically analyse rehabilitation progress. Both the Rehab@Home system and virtual urban environment were positively received by patients and physicians for their successful outcomes.
Assessment with connected digital tools and objects
Online exercise platforms are designed to receive patient reports, making remote monitoring easier. The collected information can include scores, questionnaires to be completed or free-form reflections. 48 Connections are made either on dedicated websites or through dedicated applications. 49 All platforms also record the timing of connections, their number and duration. The placement of sensors, as mentioned earlier, allows for quantifying movement and provides feedback on exercise execution. More recently, Lidar (light detection and ranging) technology or depth-sensing cameras provide the same type of information but eliminate the need for sensor placement and offer increased user-friendliness. 50 As Lidar systems become increasingly prevalent in consumer hardware, it is likely that sensors will gradually be replaced by these new devices. Remote virtual reality systems are also capable of providing standard measurements such as goniometry of specific joints. 51
Acceptability of TR devices
Fifteen SRs were included in our review (Appendix 1 and 2). Overall, the results show good acceptability of telerehabilitation devices52,53 that greater self-efficacy, self-motivation, social support, intentions and previous adherence to physical therapies predict higher adherence. 54
In their study, Chen (2020) 55 demonstrates that poststroke participants mostly reported positive experiences with the TR system. They found the system easy to use due to the engaging experience and the convenience of home-based sessions. Participants emphasised the importance of technical assistance and the home environment. Additionally, family support aided them in continuing their rehabilitation. In Subedi (2020)'s literature review, 56 cardiac TR interventions were well-received by the majority of participants (80%), with 90% finding them relevant. Similarly, an individualised TR intervention that integrates exergaming and clinical video teleconference is acceptable for patients with multiple sclerosis and can serve as a viable alternative to traditional rehabilitation methods. 57 Paediatric TR is also feasible in clinical settings, and services are acceptable to patients’ families. 58
Roy (2023)'s study 20 shows that patient expectations regarding TR vary depending on the condition (effects, absence of travel, self-rehabilitation) and that devices should aim to align tools with these expectations to promote treatment adherence. The study also indicates high overall satisfaction.
Regarding patient-therapist interactions, concerns about impersonal care with telehealth have been reported in prior qualitative research. 59 However, studies demonstrate that the provider-patient relationship was not affected by videoconferencing 60 and that the comfort of being at home could facilitate a more relaxed and personal encounter. 61 Elliott et al. 62 reported that communication, particularly establishing rapport and developing patient-centred relationships, was frequently mentioned by highly satisfied telemedicine patients. 63
Nonetheless, there are barriers to the adoption of TR, particularly among healthcare professionals. 63 In a survey, Fernandes et al. (2022) 64 found that 55% of physical therapists (717 respondents) disagreed with the idea that TR is as effective as in-person programs, compared to 39% of the general population (1107 respondents). The cited barriers relate to technical connection issues, lack of training, 65 the feeling of being unable to perform all assessments and treatment techniques, or the absence of physical contact as a foundation of the therapeutic relationship. 66 There are also concerns about liability in case of adverse events. 63 Mixed models can overcome these obstacles by utilizing each modality for its advantages, such as physical contact, touch, direct communication for in-person sessions, 67 self-assessment, ecological environment assessment and automatic feedback through connected objects for remote sessions.
Overall, acceptability remains high regardless of the specific conditions, but attention should be paid to key determinants. Factors that facilitate acceptance include access to internet-enabled devices, financial benefits, knowledge of ehealthcare, proper training, technology as a valuable tool, motivational aspects, satisfaction and willingness. On the other hand, barriers to acceptance encompass affordability of devices, network connectivity, lack of technical skills and digital literacy, as well as legal issues.68–70 Moreover, factors such as availability of compatible devices, technical support, interactive system features, information accessibility, privacy, quality of questionnaires, patient physical and psychosocial condition and age are associated with patient acceptance and utilisation of home-based TR services. 71
Level of evidence in TR: Efficacy and efficiency
As shown in Figure 1, the data from the literature and SRs on remote rehabilitation are extremely numerous. In total, 198 SRs addressing the efficacy of TR have been identified (Appendix 1).
The efficacy of a treatment refers to its intrinsic ability to produce beneficial outcomes in ideal conditions. In contrast, the efficiency of a treatment focuses on achieving the best possible outcomes while optimally managing available resources.
In terms of efficacy, the Cochrane review of Laver (2020) 72 on post-stroke TR concludes that despite an increasing number of randomised controlled trials testing the efficacy of TR, it is challenging to draw definitive conclusions about its effects. Currently, only low to moderate evidence allows determining if TR is more effective or equally effective as in-person rehabilitation. Studies comparing TR to face-to-face therapy have not revealed significant differences between groups, suggesting that TR is not inferior. Moreover, analysed trials have shown no serious adverse events related to TR. The field is evolving, and additional studies are needed to reach more definitive conclusions. Since then, several studies have strengthened the levels of evidence for the utility of TR.73,74
Another Cochrane review suggests that primary pulmonary rehabilitation delivered through TR for individuals with chronic respiratory diseases yields similar results to traditional centre-based pulmonary rehabilitation, with no safety concerns identified. 75 TR has also proven superior in improving functional capacity in heart failure patients. 76 There is limited evidence for the use of TR in lower limb recovery after a stroke, mainly due to unique safety challenges. 77
Compared to in-person rehabilitation, synchronous remote care is presented as more affordable and accessible 78 and equally effective as in-person rehabilitation for various musculoskeletal pathologies.79,80 Although these interventions are useful in overcoming geographical barriers, they may be insufficient in addressing time and scheduling constraints and do not account for the shortage of human resources, 81 thus asynchronous TR complements them.
Regarding the levels of evidence for asynchronous devices, data collected in the SR by Janela (2023) 82 suggest that asynchronous TR with inertial motion sensor-based biofeedback can be effective in reducing pain and improving function compared to other interventions, although evidence is of low certainty. Very low certainty evidence was obtained for camera-based TR interventions.
Overall, research indicates that TR is as effective as traditional face-to-face rehabilitation in treating pain, physical function and quality of life in adults with physical disabilities. Recent studies and SRs support the positive clinical outcomes of TR, which are comparable to conventional rehabilitation methods. TR can serve as an alternative approach for individuals with physical disabilities, offering similar benefits to traditional rehabilitation interventions. 83 The findings from the Umbrella and Mapping Review With Meta-Meta-Analysis by Suso-Marti in 2021 are consistent with more recent studies, highlighting the efficacy of TR in achieving positive clinical outcomes. 84
Cost-effectiveness
The analysis of SRs on cost-effectiveness reveals that the EuroQol 5-Dimension (EQ-5D) is the most commonly used quality of life assessment. 85
Kloek et al. (2018) 86 noted that few studies were available, but since then, other SRs have enriched the data.87–91
Kloek et al. (2018)86 indicate that e-exercise itself was significantly less expensive than usual physiotherapy in hip and/or knee osteoarthritis patients, but it was not cost-effective from a societal and healthcare perspective. The choice between the two interventions may depend on patient and physiotherapist preferences. Suso-Martí (2021) 84 concludes that TR offers clinical outcomes comparable to conventional face-to-face rehabilitation approaches.
In the field of cardiac rehabilitation, Scherrenberg (2020) 87 concludes that TR results in similar or lower long-term costs, making it as cost-effective as traditional centre-based rehabilitation. However, significant heterogeneity exists among all included TR interventions concerning duration, technology used, cost inclusions and follow-up. These findings are confirmed by Batalik (2023). 92
Duruflé (2023), 93 in the context of severe neurological pathologies in home-based interventions, reports a similar cost-effectiveness compared to in-person rehabilitation, even though the caregiver's time is increased in TR for the same cost. The study also raises the question of the suitability of TR in the face of complex cases. Furthermore, in the case of chronic low back pain, TR, with comparable effectiveness, may show lower short-term costs 94 without the certainty of retaining these gains in the long term.
From a global perspective, there is evidence that TR is a cost-effective intervention for a broad population in various pathological domains, and further studies on cost-effectiveness 89 are necessary.
Discussion
The promise of TR and telemedicine, in general, was to offer better access to healthcare for remote populations (rural areas, medical deserts, chronic diseases and elderly individuals). Post-COVID studies do not confirm this promise. The figures reported by the DRESS (French Research, Studies, Evaluation and Statistics Department) show that in 2021 teleconsultations: nearly a quarter of teleconsultations were conducted among the top 20% of the population living in areas with the highest number of general practitioners, and only barely 18% among the bottom 20% of the population living in the least well-equipped areas. Seven out of 10 general medicine teleconsultations concerned patients from large urban centres in 2021. Additionally, teleconsultations were more often conducted with younger patients, regardless of their area of residence. In 2021, 45.2% of teleconsultations with private general practitioners were conducted with patients aged 15 to 44, compared to 28.7% of in-person consultations and 5% of home visits. 95
Furthermore, even if patients are willing to use it, resistance to change persists among healthcare professionals, and despite the growing interest in rehabilitation technologies, various obstacles to the use of digital services may continue to perpetuate a digital divide. 96 If telemedicine represents a real factor in improving the performance of the healthcare system in the face of national public health challenges, its success inevitably requires significant transformations: extensive training in the use of digital tools, resolving the interoperability issue between business software and telemedicine, reliable internet connections, assurance of data security, evolution of regulatory constraints, and above all, a relaxation of attitudes, such as the fantasy of ‘uberisation’ of healthcare. 97 The 2024 study by Härkönen confirms that compared to standard care, digital services have had a mixed impact on population health as well as on costs. 98
While the literature widely demonstrates the equivalence of TR in measured effects, the importance of the caregiver–patient relationship tends to favour mixed rehabilitation pathways that combine in-person and remote elements. Indeed, studies have noted difficulties with non-verbal communication and missing social cues in telemedicine. 99 One study also highlighted the necessity of physical contact and examination as a means to perform the ‘expected rituals’, which are important in the general practitioner–patient relationship. 100 In TR, the design of the scenario encompasses three temporal phases: (a) the face-to-face interaction, (b) synchronous remote interaction and (c) asynchronous remote interaction. The distribution must align with participants’ expectations and healthcare professionals’ constraints. Furthermore, social cohesion may be augmented in specific instances through synchronous group activities. This form of engagement occasionally elicits very high satisfaction levels. 101
Another limiting factor is the cost and remuneration of healthcare professionals. This issue was raised early on, as early as 1997, 102 suggesting that public authorities and healthcare professionals could act on telemedicine in two areas: (a) intervening in the institutional environment and (b) implementing organisational and financial forms and mechanisms capable of regulating these remote relationships. It took the COVID-19 health crisis to see a forced evolution of regulation and financing, but ‘costs’ are rarely studied in depth in research 103 and remain a barrier to their use.
These actions are highly likely to benefit from remote technologies, minimizing travel and facilitating access to information. Healthcare facilities must heed these demands and develop solutions capable of addressing the challenges encountered and the burden on caregivers.
Limitation
This study, as a scoping review of SRs, presents certain limitations. One notable aspect is our decision not to restrict the selection exclusively to SRs adhering to specific methodological guidelines such as the PRISMA checklist. While PRISMA compliance ensures a high standard of reporting and methodological rigor, our broader inclusion criteria allowed us to capture a wider range of data and insights.
By including SRs with varying levels of methodological rigor, we aimed to provide a more comprehensive overview of the TR landscape. However, this approach also introduces variability in the quality of the included reviews, which can affect the consistency and reliability of our findings. The diverse methodological standards could lead to variations in search strategies, data extraction processes and study selection, potentially impacting the overall conclusions.
Despite these potential inconsistencies, the open selection criteria enabled us to gather a broader spectrum of evidence, reflecting the real-world application and diverse practices in TR. This inclusivity is beneficial for understanding the wide array of clinical outcomes, technical requirements and the role of family caregivers across different settings and populations.
It is important to note that the aim of our study was not to conduct a meta-analysis but to map the existing literature and identify key themes and gaps in TR research. As such, the broader inclusion criteria were appropriate for achieving this objective. Future research could benefit from a more targeted approach, potentially focusing on high-quality SRs to enhance the precision and reliability of specific findings within the TR domain.
Clinical recommendations
Firstly, it is advisable not to limit TR to a single mode but to utilise and mix various methods, including synchronous, asynchronous and in-person sessions. This hybrid approach can enhance the effectiveness and flexibility of rehabilitation programs, catering to individual patient needs and preferences.
Secondly, involving patients or caregivers in remote evaluations is essential. Encouraging self-assessment, guided by digital tools, can be an effective strategy. Future research should focus on developing and refining these self-directed assessment methods to ensure their reliability and ease of use.
Thirdly, healthcare professionals must be trained and actively engaged in the digitisation process. Their involvement is crucial in maintaining a strong and consistent connection with patients, which is fundamental for successful TR. Training should encompass not only technical skills but also strategies for effective communication and patient engagement in a digital environment.
European rehabilitation medicine aligns with our study findings by recommending Physical and Rehabilitation Medecine (PRM) physicians provide remote rehabilitation services through digital or communication technologies to eligible individuals when necessary and feasible across various health conditions. 104 This approach prioritises the patient and their family, focusing on evidence-based effectiveness and adherence to regulations. This strategy ensures that rehabilitation services are accessible and efficient for patients, allowing for timely and effective interventions that can improve outcomes and quality of life. By utilizing digital tools and communication technologies, PRM physicians can overcome barriers to traditional in-person rehabilitation services and reach a broader population in need of care.
Conclusion
A thorough examination of TR practices in the field of rehabilitation reveals a complex landscape. The effectiveness of these approaches compared to in-person rehabilitation varies depending on the pathologies, methods and technologies employed. Current evidence demonstrates that TR can be as effective as in-person rehabilitation for various conditions, including musculoskeletal disorders and cardiac diseases. Additionally, it offers advantages in terms of accessibility and, in some cases, cost-effectiveness, making it an appealing alternative.
However, uncertainties persist, particularly concerning asynchronous TR and cost-effectiveness considerations. The quality of evidence varies from one study to another, underscoring the need for further research to consolidate findings. Moreover, it is important to note that TR may not address all practical constraints, such as time constraints and limited human resources.
Ultimately, TR holds promising potential for expanding access to rehabilitation care, but its application should be carefully tailored to the needs of patients and the specificities of various conditions, with trained professionals. The choice between in-person rehabilitation and TR should take into account patient preferences, demonstrated clinical effectiveness and the practical context in which it is implemented.
Overall, healthcare facilities and professionals should focus their thinking on planning and storyboarding mixed-care solutions tailored to the typology of health issues. Additionally, when caregivers are involved, they should be able to rely on both national and local resources to best support this population.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076241294110 - Supplemental material for Telerehabilitation solutions in patient pathways: An overview of systematic reviews
Supplemental material, sj-docx-1-dhj-10.1177_20552076241294110 for Telerehabilitation solutions in patient pathways: An overview of systematic reviews by Benoit Nicolas, Emilie Leblong, Bastien Fraudet, Philippe Gallien and Patrice Piette in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076241294110 - Supplemental material for Telerehabilitation solutions in patient pathways: An overview of systematic reviews
Supplemental material, sj-docx-2-dhj-10.1177_20552076241294110 for Telerehabilitation solutions in patient pathways: An overview of systematic reviews by Benoit Nicolas, Emilie Leblong, Bastien Fraudet, Philippe Gallien and Patrice Piette in DIGITAL HEALTH
Supplemental Material
sj-docx-3-dhj-10.1177_20552076241294110 - Supplemental material for Telerehabilitation solutions in patient pathways: An overview of systematic reviews
Supplemental material, sj-docx-3-dhj-10.1177_20552076241294110 for Telerehabilitation solutions in patient pathways: An overview of systematic reviews by Benoit Nicolas, Emilie Leblong, Bastien Fraudet, Philippe Gallien and Patrice Piette in DIGITAL HEALTH
Footnotes
Acknowledgements
The authors do not have acknowledgements to declare.
Author contribution
BN initiated the collaborative project, managed and coordinated the research activity; PP and PG wrote the method; PP and BF designed data collection tools, monitored data collection; PP wrote the initial draught; EL, PG and BN revised the draught article and had critical review, commentary or revision; PP prepared and created the published work.
Consent statement
This article is a review of SRs and does not involve patient data; therefore, consent is not required.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
Ethical approval was not required for this study, as it involved a review of previously published data.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Guarantor
The guarantor of this study is PG.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.