
Abstract
Difficult visceral cancer pain is defined as pain that does not improve with conventional non-pharmacological and pharmacological strategies, including opioids and adjuvants, and occurs in up to 15% of patients with cancer. In oncological practice, we must be prepared to establish strategies for dealing with such complex cases. Different analgesic strategies have been described in the literature, including managing refractory pain through palliative sedation; however, this might become a dilemma from a clinical and bioethical point of view in end-of-life situations. We present the case of a young male patient with moderately differentiated intestinal-type adenocarcinoma of the left colon, with intra-abdominal sepsis, and for whom despite the multimodal treatment for difficult visceral cancer pain, the pain was refractory leading to palliative sedation. Difficult visceral cancer pain is a pathology that affects the quality of life of patients and is a challenge for pain specialists, for both pharmacological and non-pharmacological management.
Keywords
Introduction
Pain is one of the most prevalent symptoms in patients with cancer, making it a challenge for the oncological professional because it involves two major interventional components: first is the physical component because of the effect of tumor and effects of oncospecific treatment, and second is the non-physical component represented by emotional, socioeconomic, and in several patients, spiritual suffering.1–4
Difficult visceral cancer pain (DVCP) occurs in up to 15% of patients with cancer worldwide 3 and is defined as the absence of adequate analgesic control with non-pharmacological and conventional pharmacological strategies, including potent opioid medications at maximum tolerable doses and adjuvant drugs. In parallel, the phenomenon of tolerance to opioids should always be considered, which is defined by the Food and Drug Administration as “those who are taking at least: oral morphine 60 mg/day, transdermal fentanyl 25 mcg/h, oral oxycodone 30 mg/day, hydromorphone 8 mg oral/day, or an equianalgesic dose of another opioid for one week or more.”1,2,4,5
In addition, it is important to define a refractory symptom, which refers to a symptom that cannot be adequately controlled despite aggressive efforts to identify a tolerable therapy that does not compromise consciousness and generally implies suffering that cannot be alleviated with routine measures.
The pathophysiology of convergent afferents with integration into the secondary somatosensory cortex is specifically given for visceral cancer pain. It is significantly represented in the limbic system, increasing its complexity, and allows a greater capacity of chronification and opioid-induced hyperalgesia, making it essential to approach it from the viewpoint of different visceral pain syndromes in the oncological context or secondary to the development of specific oncological treatments for chronic visceral pain syndrome.1,6–8
Case
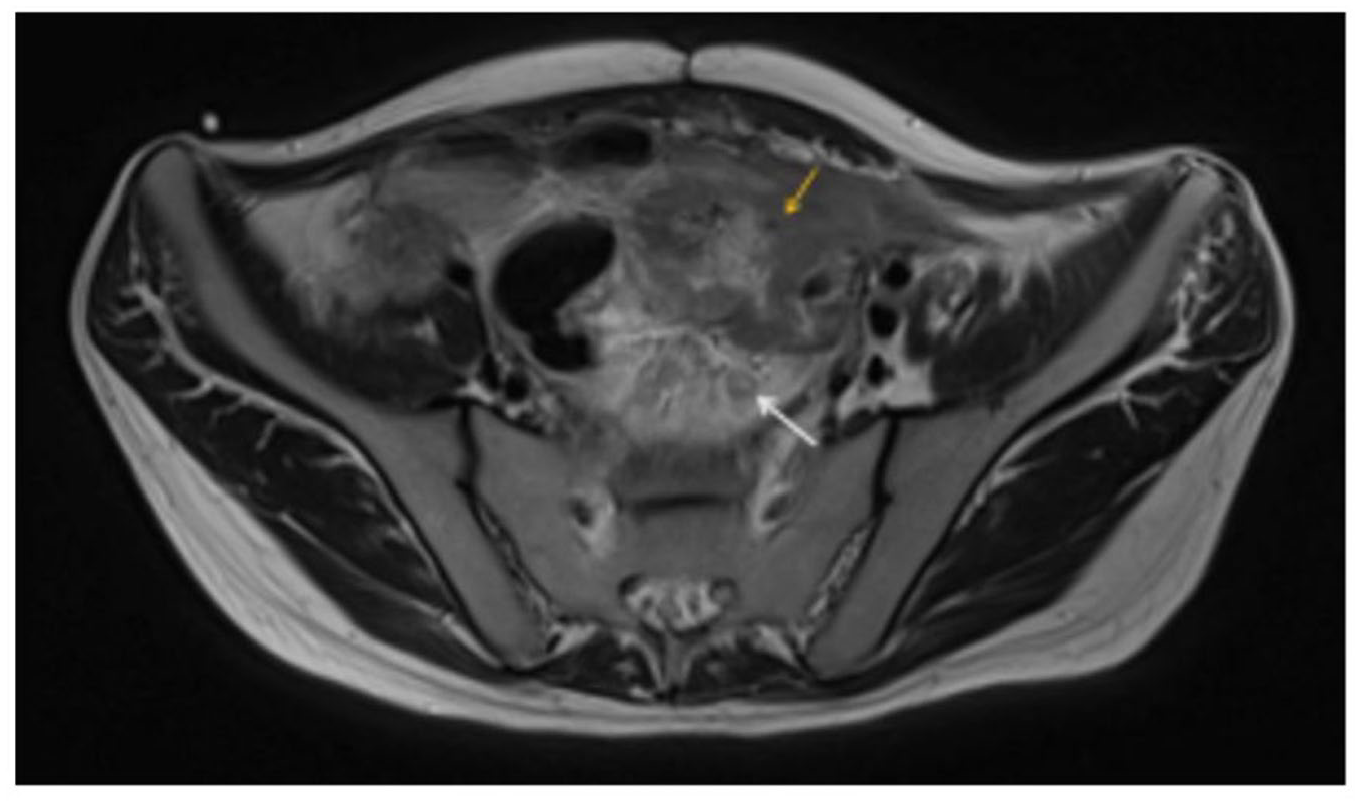
A 27-year-old man was diagnosed with a family history of lynch syndrome and a diagnosis of intestinal-type left colon adenocarcinoma, moderately differentiated, ulcerated, and necrotic with imminent intestinal obstruction minimal stage T4NXM0. Mutation was not detected in the pathogenic variant of MLH1 gene Braf gene, and mutation was detected in the KRAS gene in EXON 2 (G12x), associated with chronic abdominal pain for more than 6 months, prior to surgical management with a performing status: Karnofsky Index 60 and Eastern Cooperative Oncology Group (ECOG) Performance Status Scale 2. He received surgical treatment first and then adjuvant chemotherapy as shown in Table 1, with subsequent evidence at 5 months of progression of the disease of increased peritoneal nodules (some on the bladder) and lymph node conglomerate at the mesenteric level. The patient was admitted to the emergency department 10 months after initial surgical management due to cramping pain of strong intensity in the left hemiabdomen (visual analog scale (VAS) score, 10/10), associated with signs of systemic inflammatory response. Broad-spectrum antibiotic management was started with piperacillin/tazobactam at a dose of 4.5 g every 6 h, and a nuclear magnetic resonance was taken to rule out tumor involvement versus intra-abdominal collections with the following findings: mass dependent on the rectum and superior rectosigmoid junction (orange arrowhead) and dilatation of the inferior rectum (arrow white) (Figure 1), mass with circumferential, lobulated involvement of sigmoid walls (yellow arrowhead), suspicious lymph nodes and mesorectal lymph nodes (white arrow) (Figure 2), and dilatation of the inferior rectus (white arrow) (Figure 3.)
Summary of the treatment of pain and complications of oncological disease.
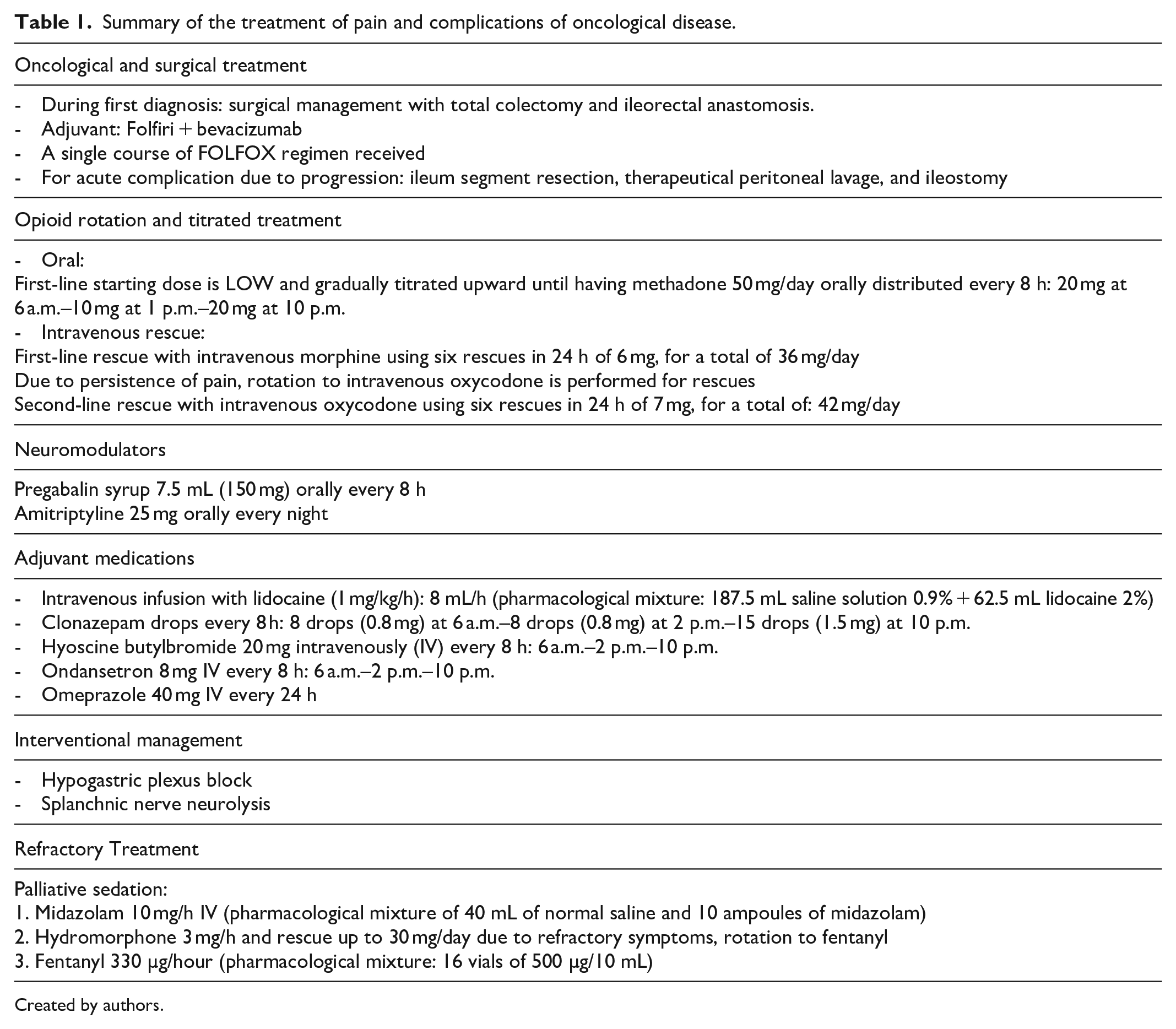
Created by authors.

Magnetic resonance imaging of the pelvis. T2-weighted sequence, mass dependent on the rectum and superior rectosigmoid junction (orange arrowhead) and dilatation of the inferior rectum (arrow white).
Magnetic resonance imaging of the pelvis. T2-weighted sequence, identifying a mass with circumferential, lobulated involvement of sigmoid walls (yellow arrowhead) and suspicious lymph nodes and mesorectal lymph nodes (white arrow).

Magnetic resonance imaging of the pelvis, T2-weighted sequence shows dilatation of the inferior rectus (white arrow).
With these findings, an exploratory laparotomy was performed, in which intestinal perforation and small bowel loops, mostly blocked and adhered to the abdominal wall, were observed, with generalized peritonitis being observed. Based on these results, resection of the ileal segment, therapeutic peritoneal lavage, and ileostomy were performed, leaving the abdomen open with a Bogota bag (sterile plastic bag used to close abdominal wounds). The patient required two more peritoneal lavages, and a new peritoneal lavage and closure of the abdominal wall was performed 7 days after the first intervention.
During these interventions, the surgical team used general anesthesia (remifentanil-propofol) with immediate intubation and extubation after the procedures, with no description of complications.
Prior to surgery, the patient had an average opioid consumption of 100 mg daily morphine milligram equivalents, which increased with each of the surgical interventions.
The patient presented a high consumption of opioids (>300 parenteral morphine milligram equivalents), given the increased requirement due to persistent pain. Rotation to other opioids was also used as a strategy, as well as the use of multimodal analgesics including the use of neuromodulation; given the lymphatic involvement at the mesenteric level and pelvic nodes, lidocaine infusion was also used, with an average time of 48 h on at least two occasions for DVCP. Due to refractoriness to intravenous opioids, it was decided to perform interventional management with chemical neurolytic blockade of the hypogastric plexus with 10 mL of 96% absolute alcohol using the transdiscal technique (L5-S1), with subsequent pain modulation for 4 days. One week later, a chemical neurolytic block of the splanchnic nerves was performed with 10 mL of 96% absolute alcohol using the transdiscal technique (T11-T12). Pain was modulated for approximately 10 days. The summary of the treatment received during hospitalization is shown in Table 1.
Due to torpid clinical course, uncontrolled pain despite multimodal treatment, intestinal fistula, persistence of sepsis, and cancer progression, there was a high probability of death with survival of less than 3 weeks.
Taking into account that he was a young patient with an advanced and complex oncological disease, psychosocial risk and difficult symptom control, bad oncological prognosis, a high risk of short-term complications, and pain refractory to different multimodal management strategies (VAS score of 8/10, 2 months after admission to the emergency department), ne needed to receive support for mental health (psychology and psychiatry).
Even after all medical efforts, the pain was refractory, so with the patient’s mother’s consent it was decided to start palliative sedation, explaining the risks and benefits of the same. Given this decision, midazolam infusion was titrated as shown in Table 1, with sedation measured using the Richmond Agitation-Sedation Scale (RASS +1)9,10 and Edmonton Staging System (11/24). 11 After 48 h, the opioid was changed from hydromorphone to fentanyl, achieving better symptom control and deeper sedation (RASS −3),9,10 with continued monitoring and multimodal symptom support until death 7 days after the start of sedation due to his advanced oncological disease.
Discussion
Chronic visceral pain associated with cancer is usually related to disease progression (due to visceral involvement, compression, or neural infiltration) or complications related to specific oncological management, such as hemorrhage, abscess, or perforation, leading to the development of chronic pain.
DVCP is characterized by a short duration of pain with severe intensity, or it may be spontaneous (involuntary) and of longer duration (approximately 30 min to 4 h), with one to four episodes a day. Somatic and neuropathic pathophysiological mechanisms are observed, which may explain the characterization of a diffuse underlying pain associated with other clinical manifestations, such as irradiation, autonomic symptoms, and neurological signs, that allow the differentiation of chronic pain syndromes associated with cancer as mentioned by Cherny et al. 3
Also, patients can present with infiltration plexopathy, which manifests as diffuse abdominal pain due to distension, mesenteric tension, or mural ischemia in relation to peritoneal compromise or chronic malignant intestinal obstruction, making more complicated the treatment of pain and requirement of a multimodal approach. 12
When facing DVCP diagnosis, we usually categorize individuals into three types: those who present with basal pain controlled with the use of strong opioids, those who present with basal pain and require the use of titrated opioids for rescue, or those with non-modulated basal pain; this classification can help define the steps toward pharmacological treatment. In the pharmacological treatment of visceral cancer pain, it is unlikely that a single analgesic will significantly control pain because multiple transmitters and receptors, such as ion channel receptors, are responsible for pain transmission. Therefore, certain analgesics need to penetrate the central nervous system to relieve pain completely and effectively; examples of these are lidocaine infusions and neuromodulators which may be used as a strategy of multimodal treatment.13,14
Although the first line of treatment is the management and titration of the potent opioid, where there is no evidence of superiority of a particular opioid and considering the high incidence of hyperalgesia in cancer abdominal pain, methadone is a good option. 15 Among the adjuvants, the combination of non-steroidal anti-inflammatory drugs or corticosteroids in short cycles may have better results than monotherapy. There are also medications such as anticholinergics and octreotide that show greater benefits, mainly for malignant intestinal obstructions. Antidepressants or anticonvulsants are selected based on the symptoms of the patient. 16
The use of short-term oral opioid rescues (usually between 10% and 20% of the total dose) and transmucosal fentanyl with an adequate analgesic for basal pain is considered. Therefore, treatment will be conditioned according to the functionality, the degree of tolerance, and not the number of episodes per day. Education about “pain anticipation” should also be provided for incident pain to decrease pain intensity.17,18 A non-pharmacological treatment approach is necessary, which comprises preventing the trigger by adapting to the environment and interventions by occupational and physical therapy.
Among the concepts to be treated in DVCP are tolerance and hyperalgesia induced by opioids (HIO). 19 We defined tolerance as the requirement of an increase in dose to achieve pain control. This action may be one of the factors that perpetuates DVCP and makes it chronic. Similarly, the presentation of HIO must be considered; this reaction is very common in individuals with advanced oncological diseases and chronic cancer pain of any type. It is defined as the increased sensitivity to painful stimuli because of the chronic use of opioids, that is, pain intensifying on increasing the opioid dose, making analgesic management and symptomatic control challenging.20–22
While implementing the multimodal approach, in this case report, two interventional techniques were mainly used that we consider effective in optimizing the proposed analgesic management since they mitigated DVCP as the main refractory symptom. Chemical neurolytic blocks with absolute alcohol were administered to the splanchnic and hypogastric plexuses.
The interventional management of DVCP is fundamentally based on neurolytic-type procedures with chemical agents (phenol and absolute alcohol) or thermal agents acting on the abdominal–pelvic sympathetic axis, including the approach of the splanchnic nerves or celiac ganglia (pain in the upper abdomen), hypogastric plexus (pelvic pain), and ganglion impar (genital or perianal pain). Selective dorsal root ganglion neurolysis or even mixed root ganglion neurolysis can be performed to block nerve conduction in areas compromised by tumor progression. In cases of an extensive advanced abdominal–pelvic disease, regional epidural analgesia with or without an entry port or implantation of programmable intrathecal pumps is useful. Similarly, for pain with a neuropathic component, posterior cord or dorsal root ganglion stimulation implant can be used. 12
Here, we described a case where analgesic strategies for multimodal management and interdisciplinary treatment for an advanced oncological diagnosis, along with highly complex palliative management, were adopted at the Instituto Nacional de Cancerología in Bogotá, Colombia. This additionally brought together multiple physical and psychosocial factors with a high symptomatic load. We must face these scenarios daily by performing interventions based on biological, psychological, and social models, including the combination of a multimodal approach using strong opioids plus rescues that could be intravenous, subcutaneous, or oral, anti-neuropathic agents; continuous intravenous infusions; interventional neurological procedures, and all of these accompanied by the support of mental health and social work. The goal, despite clinical and functional deterioration, is to contribute to an improved quality of life and mitigate the suffering of the individual with cancer and their family, and support patients in end-of-life conditions.
Figure 4, created by the authors, summarizes DVCP as an entity given by multiple reversible and non-reversible etiologies in which to define management, the clinical status of the patient and their functionality must be taken into account, for which we can use the scales described above.
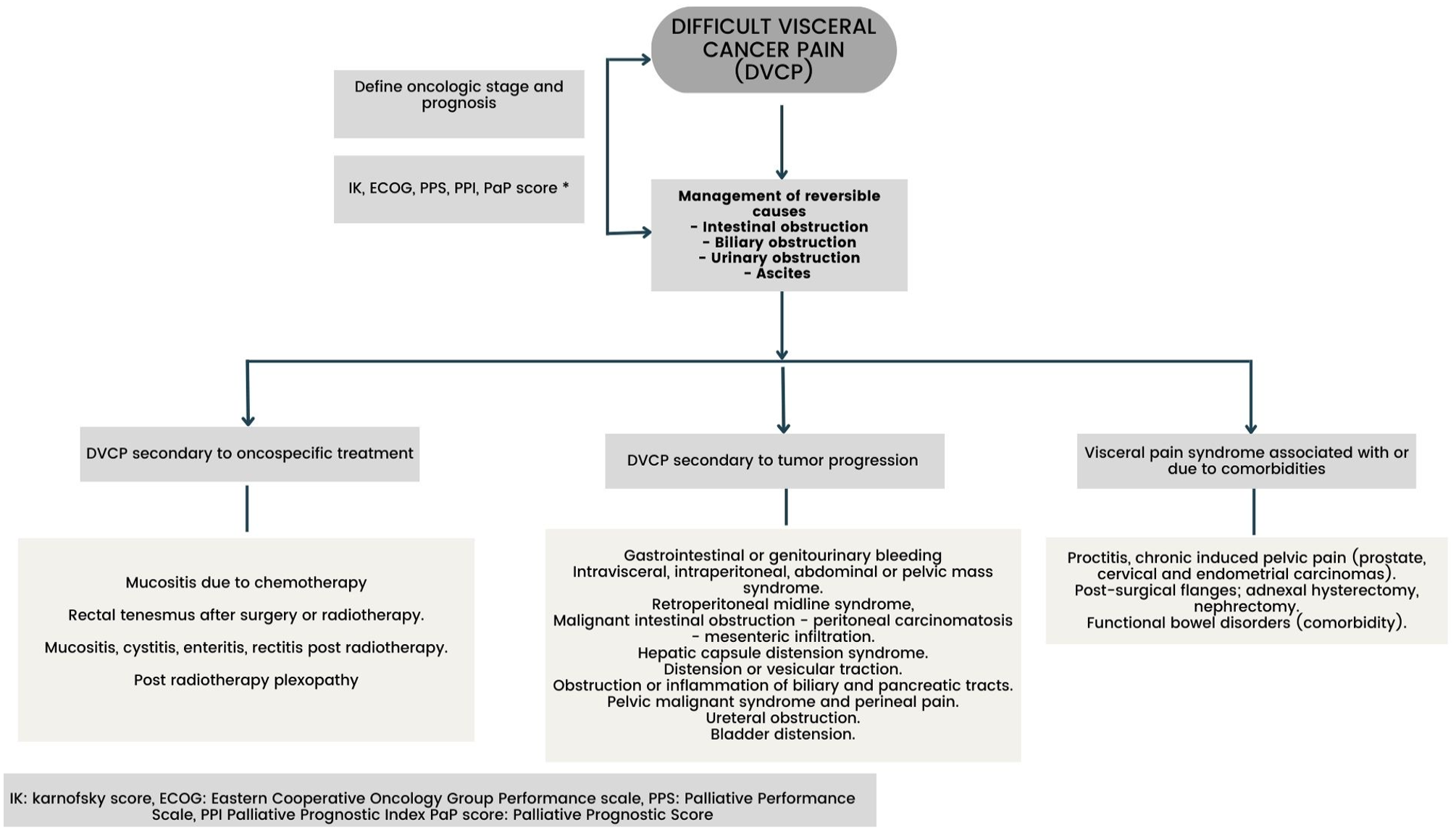
Difficult visceral cancer pain syndromes.
Conclusion
DVCP is a challenge for physicians, as it is a complex entity that requires multiple interventions, not only pharmacological but also non-pharmacological. This explains the importance of multimodal management in those patients with refractory pain. This case report shows some points about the clinical presentation of the DVCP, as well as emphasizes the multimodal strategy of the oncological pain approach that requires the recognition of the entity, as well as the importance of having guidelines to manage complex cancer pain problems in an optimal way.
Footnotes
Acknowledgements
Author contributions
All authors listed have significantly contributed to the investigation, development, and writing of this article
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Disclosures
Edmonton Staging System (Copyright 2019) was obtained from the Director, Division of Palliative Care Medicine, Department of Oncology, University of Alberta and is freely available for use. The Spanish version by C. Centeno, A. Noguera, B. Lopez, and A. Carvajal was used. Eastern Cooperative Oncology Group Performance Scale and Karnofsky Index circulate in the public domain and are therefore available for public use. Visual Analog Scale does not require a license and is available for free download directly from Scott & Huskissonor Medscape.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval to report this case was obtained from Institutional review board of the Instituto Nacional de Cancerología in Bogotá, Colombia (approval number 0014) and was performed according to the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards
Informed consent
Written informed consent was obtained from a legally authorized representative for anonymized patient information to be published in this article.