
Abstract
Pediatric maxillofacial surgery airway management is difficult due to physiological and anatomical differences between children and adults. Pediatric patients have a bigger tongue, omega-shaped epiglottis, and cranially positioned larynx, which makes intubation and breathing difficult. For anesthesiologists, children with limited mouth opening can impair airway access and increase induction problems. Maxillofacial surgery includes oral, facial, ear, nose, and throat (ENT), plastic, neurosurgical, and base of skull operations. This article provides an overview of the various types of pediatric maxillofacial surgeries that are commonly performed. These surgeries include cleft lip and palate repair, mandibular distraction osteogenesis, orthognathic surgery, craniosynostosis surgery, and trauma treatment. Since pediatric maxillofacial surgery can significantly affect the airway, adequate airway management in these patients is a challenging task for anesthesiologists. This review article also discusses pediatric patients’ unique anesthesia and maxillofacial surgery challenges and specific anesthetic plans for each procedure. Anesthesiologists can improve pediatric maxillofacial surgery safety and outcomes by completely addressing these difficulties and personalizing anesthetic regimens for each patient.
Introduction
Craniofacial and maxillofacial deformities in children are one of the challenging conditions for both surgeons and anesthesiologists. A wide range of congenital and acquired diseases affects the craniofacial region in the pediatric population. Most of the congenital deformities are syndromic, but non-syndromic deformities are also seen. 1 Acquired diseases include neoplasms of the soft tissue or bones of the craniofacial region. The anesthesia protocol and challenges vary for these congenital and acquired maxillofacial conditions. Younger patients present significant challenges for anesthesia because of their small airways and physiological differences from adults. Children also have different pharmacokinetics and pharmacodynamics for various anesthetic agents and drugs compared with adults. Therefore, pre-operative evaluation and planning for general anesthesia in children with craniofacial and maxillofacial disorders are crucial.
Challenges in Pediatric Oral Maxillofacial Anesthesia
Management of the Airway
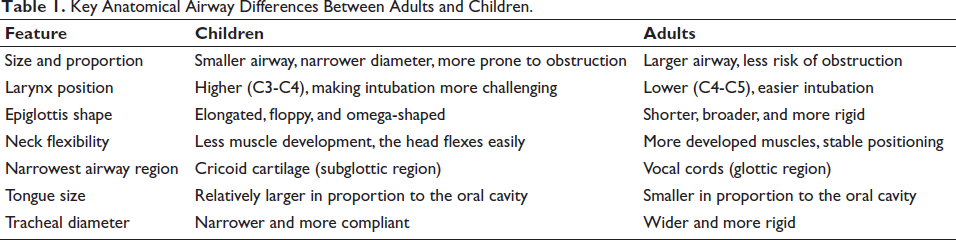
Administering anesthetic while maintaining a child’s airway presents significant problems, particularly in maxillofacial procedures due to their distinctive anatomical features. The airways of children are smaller and anatomically distinct from those of adults (Table 1), which results in conventional intubation techniques not consistently yielding the anticipated outcomes. Factors such as reduced mouth opening due to surgery or anatomical variations can make it much more difficult.1, 2 In contrast to adults, children possess a proportionately larger tongue, enlarged tonsils and adenoids, and a pliable epiglottis that can readily obstruct the airway. Their larynx is positioned higher in the throat, and their trachea is more constricted—these distinctions necessitate further caution and particular methods for airway management. 3 To address these issues, sophisticated instruments such as video laryngoscopy can be exceedingly beneficial. They offer an enhanced visualization of the airway anatomy, which facilitates the safe and effective placement of the endotracheal tube. Occasionally, in cases with limited mouth opening, a fiber-optic bronchoscope is required for the accurate placement of the endotracheal tube. In many instances, employing ultrasonography prior to the procedure can provide critical insights into possible airway complications, 4 enabling the anesthetic team to prepare in advance and circumvent any complications.
Key Anatomical Airway Differences Between Adults and Children.
Pharmacological Aspects
Pharmacological considerations are critical in pediatric oral and maxillofacial surgery, given the distinct physiological characteristics of children. Pediatric patients demonstrate considerable variability in drug metabolism due to their developing organ systems, which requires precise dosage calculations based on weight and age to prevent complications arising from over- or under-dosing. 5
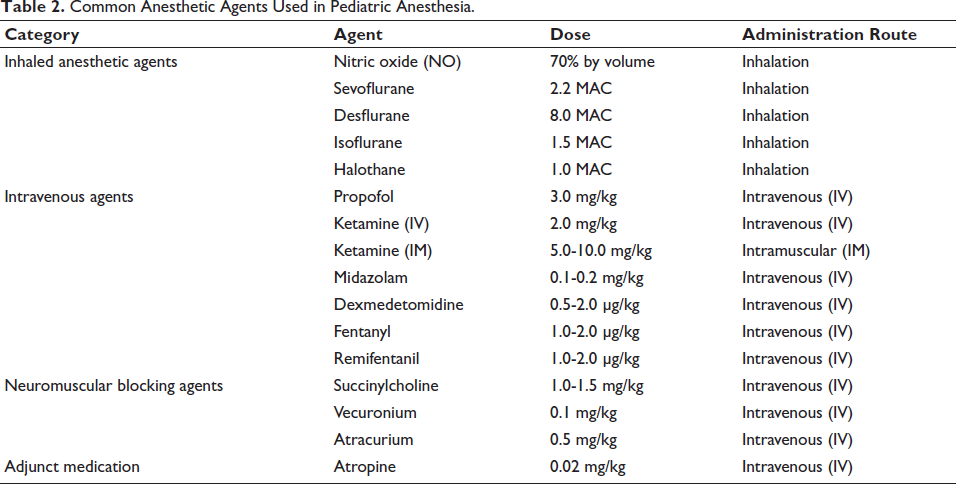
The choice of anesthetic agents should consider their pharmacokinetics and potential side effects in pediatric populations. Volatile anesthetics are frequently favored due to their rapid onset and recovery characteristics; however, their use requires careful consideration to avoid complications, like post-operative nausea and vomiting (Table 2).
Common Anesthetic Agents Used in Pediatric Anesthesia.
Psychological Factors
The feeling of fear that children have prior to surgical procedures is totally natural; yet, this nervousness can make it more difficult to administer anesthetic and may even have an impact on their recovery following the procedure. 6 Providing assistance to youngsters in achieving a sense of comfort and security is an essential component of the process.
Talking to children in a way that they can comprehend, taking into account their age and the amount of comprehension they have, can go a long way toward reducing the concerns that they have. Play therapy, storytelling, or even watching cartoons are all methods that can be utilized to assist children in feeling more at ease prior to the administration of anesthesia. 7
When it comes to relaxing their child’s anxiety, parents also play a significant role. They will be able to reassure their children and make them feel more secure if they have a better understanding of what will take place throughout the surgical procedure. As a matter of fact, research has demonstrated that children tend to have less anxiety when their parents are present during the process of inducing anesthesia.
On occasion, it may be necessary to administer medicine, such as light sedatives, in order to assist a child in relaxing before surgery; however, it is essential to carefully select the appropriate method for each individual child. 8
Comorbidities
Pediatric patients undergoing oral and maxillofacial surgery frequently exhibit comorbid conditions that complicate anesthesia management. A thorough pre-operative assessment, encompassing a detailed medical history and physical examination, is crucial for identifying underlying conditions that may affect anesthesia. Identifying these factors enables anesthesiologists to formulate improved perioperative care plans, thus promoting patient safety and surgical outcomes. 9
Obstructive sleep apnea (OSA) is a common comorbidity in this population, elevating the risk of perioperative airway obstruction. Children with OSA are especially vulnerable to respiratory complications during sedation or general anesthesia, requiring careful monitoring and customized anesthetic approaches. 10
Syndromic pediatric patients frequently pose distinct challenges in airway management due to craniofacial anomalies like micrognathia and mandibular hypoplasia, which complicate intubation and ventilation procedures. Conditions such as Pierre Robin sequence, Treacher Collins syndrome, and Goldenhar syndrome often necessitate tailored anesthetic strategies. 11 Macroglossia in children with Beckwith–Wiedemann syndrome notably elevates the risk of challenging airway management. Age under 1 year, reduced weight, and related endocrine disorders further exacerbate airway challenges in these patients. 12
The preparation and proficiency in handling complex pediatric airways are essential. Proficiency in airway management algorithms and consistent refresher training is crucial for achieving successful outcomes.
Technical Challenges
Establishing intravenous (IV) access in pediatric patients presents challenges due to smaller vein sizes and increased anxiety levels. Topical anesthetics, such as EMLA cream, which contain a combination of local anesthetics, have demonstrated effectiveness in alleviating discomfort and facilitating a smoother process. Studies indicate that EMLA cream effectively alleviates pain in children undergoing venipuncture. 13
In cases where IV access is challenging, inhalational induction using agents such as sevoflurane presents a rapid onset and is generally well-tolerated in pediatric patients. Inhalational induction presents a greater risk of respiratory complications relative to IV methods. Research indicates that children undergoing sevoflurane inhalation induction are at a higher risk of experiencing respiratory complications compared to those receiving IV induction with propofol. 14
Anesthesiologists must evaluate the advantages and disadvantages of each induction method to ensure the safest and most effective anesthesia, customizing their approach to meet the unique needs of each patient and the particular surgical context. A comprehensive pre-operative assessment, along with the implementation of suitable techniques and supportive strategies, can address these technical challenges and facilitate a more seamless anesthesia experience for pediatric patients undergoing oral and maxillofacial procedures.
Unique and Distinctive Challenges Encountered in Pediatric Anesthesia for Maxillofacial Surgery
Pediatric patients undergoing maxillofacial surgical procedures represent a unique challenge for anesthesiologists for multiple reasons. The challenges faced in anesthesia for pediatric surgeries are often further complicated for maxillofacial surgeries due to certain unique characteristics of this patient population. Maxillofacial surgeries in pediatric patients are mostly orthodontic in nature. Hence, the underlying diagnosis often presents elastic, compliance, or age-related challenges in anesthesia. In addition, these patients often come with significant comorbidities such as craniofacial syndromes or associated syndromes affecting the airway and other physiologic baseline. 11 The anatomic and physiologic differences in pediatric patients compared to adults cause challenges in airway management, drug dosing, choice of anesthetic agents, post-operative analgesia, and others. These differences create a relative lack of safety margin in vital functions such as neurologic, respiratory, and cardiac, which are often most stressed by anesthetic agents and surgical manipulation. The technical challenges in pediatric anesthesia for maxillofacial surgeries are further exacerbated by long-duration surgeries, the use of head fixation equipment, the use of adjuncts for control of bleeding, and others. Anesthesia for pediatric maxillofacial surgeries represents a very delicate balance of managing multiple expected and serendipitous challenges occurring at once. This section discusses the relevant challenges faced in anesthesia for pediatric patients undergoing maxillofacial surgical procedures.
Pre-operative Assessment
Pre-operative assessment is crucial for the effective management of general anesthesia in pediatric patients undergoing maxillofacial surgical procedures. Factors such as age, weight, medical history, presence of comorbidities, and surgical complexity are carefully evaluated. Children with congenital facial deformities often have associated systemic anomalies and comorbidities, making a thorough pre-operative assessment even more important. Routine laboratory tests like complete blood count, hemoglobin level, and electrocardiography may not be necessary for otherwise healthy children undergoing elective procedures, but they should be considered for those with potential syndromes or significant comorbidities. Additionally, diagnostic imaging plays a vital role in planning surgical procedures. For children under 3 years of age, all efforts should be made to obtain imaging without sedation. Most imaging studies can be done without general anesthesia if the child is cooperative and has been adequately prepped. However, children with significant maxillofacial trauma, especially those younger than 3 years, often require emergency computed tomography (CT) scans under general anesthesia.
Children scheduled for elective maxillofacial surgical procedures should ideally be examined pre-operatively 1 day prior to surgery, allowing sufficient time for the workup of any associated comorbidities. Traumatized children should be triaged according to the mechanism of injury, and those with significant maxillofacial trauma should generally undergo pre-operative imaging studies. In instances of airway compromise due to maxillofacial injury, the pediatric airway should be addressed following guidelines.
Assessment of Physical Condition and Airway Evaluation
A thorough physical examination is essential to assess the child’s airway and identify any issues that may complicate intubation or ventilation. Key elements of this evaluation encompass the following: Mouth opening: Evaluating the inter-incisor distance to ascertain whether restricted mouth opening may hinder laryngoscopy. Neck mobility: Assessing the range of motion in the neck, as limited movement may hinder appropriate alignment during intubation. Mandibular dimensions and orientation: Assessing for micrognathia or retrognathia, which may influence the alignment of the oral, pharyngeal, and laryngeal axis. Identification of craniofacial syndromes: Recognizing syndromes such as Pierre Robin sequence or Treacher Collins syndrome, linked to challenging airways.
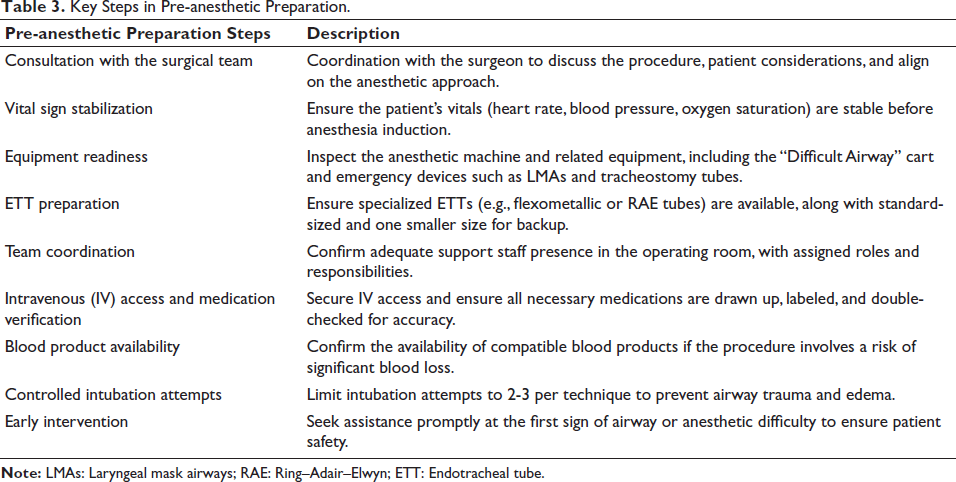
A meticulous assessment of these characteristics enables anesthesiologists to foresee and mitigate probable airway complications, so assuring a thoroughly planned strategy for safe and effective anesthetic administration (Table 3). 11
Key Steps in Pre-anesthetic Preparation.
The Infant Safe Airway Score
We recognized the absence of a specialized approach for evaluating airway hazards in infants, prompting our development of the infant safe airway (ISA) score. The current Colorado Pediatric Airway Score (COPUR) is effective for older children but fails to adequately address the distinct airway characteristics and difficulties associated with newborns.
The objective of the ISA score is to furnish a dependable, user-friendly instrument that assists physicians and anesthesiologists in assessing an infant’s airway prior to surgery. This approach enables us to plan more efficiently, foresee any complications, and guarantee safer anesthetic care for our smallest patients.
Common Pediatric Maxillofacial Surgeries and Anesthesia Plans
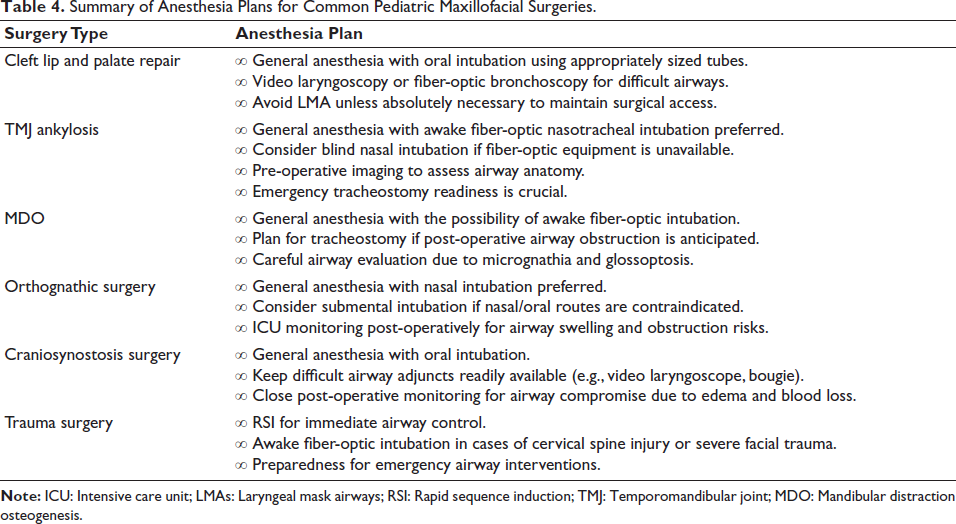
Craniofacial reconstructions often involve complicated maxillofacial reconstructive procedures and are commonly conducted on children with congenital conditions. Anesthesia has a unique challenge in providing maxillofacial surgery due to the complexity of airway procedures and the possibility of multiple simultaneous interventions, such as ophthalmologic, endoscopic, or neurosurgical surgeries. Children present an even greater challenge due to their anatomic differences compared to adults and the associated cardiac anomalies they may have. 11 This presents a brief overview of the challenges anesthesia encounters when providing surgical fixes for pediatric maxillofacial anomalies. Surgical repairs of various maxillofacial anomalies and the corresponding anesthesia plans used at an institute will also be discussed (Table 4).
Summary of Anesthesia Plans for Common Pediatric Maxillofacial Surgeries.
Repair of Cleft Lip and Palate
Cleft lip and palate repairs represent prevalent congenital interventions within pediatric surgery. Cleft lip repair is generally conducted between 6 weeks and 6 months of age, facilitating patient growth and the assessment of associated anomalies prior to the procedure. Cleft palate repair is typically performed between 6 and 12 months of age. 15
Airway management in these surgeries poses distinct challenges, stemming from anatomical variations linked to cleft anomalies. Establishing an effective seal for mask induction presents challenges, especially in infants with micrognathia or other craniofacial abnormalities. A comprehensive pre-operative evaluation is crucial for anticipating and addressing these challenges. 16
Oral intubation is typically favored, utilizing appropriately sized endotracheal tubes to suit the smaller pediatric airway. When direct laryngoscopy proves difficult, adjuncts like video laryngoscopy or fiber-optic bronchoscopy can be employed to improve visualization during intubation. Laryngeal mask airways (LMAs) are advantageous for brief procedures; however, they are generally not utilized when complete access to the oral cavity is necessary. In exceptional cases where airway management is essential, the establishment of an emergency surgical airway may be required. 16
For cleft palate surgeries, special preformed oral south-facing Ring–Adair–Elwyn (RAE) tubes are often used. These tubes can be positioned and secured to the child’s chin, which helps keep them out of the way and allows the surgical team to have better access to the operative area.
Temporomandibular Joint Ankylosis
Management of TMJ Ankylosis in Pediatric Patients
Temporomandibular joint (TMJ) ankylosis in pediatric patients poses considerable difficulties for surgical and anesthesia teams. This condition arises from the fusion of the mandibular condyle to the skull base, resulting in limited mouth opening, facial deformities, and challenges in fundamental activities, such as speaking and chewing. The primary causes of TMJ ankylosis in children are trauma, infections, and systemic diseases impacting the joint. 17
Challenges in the Management of Anesthesia
Administering anesthesia to pediatric patients with TMJ ankylosis presents significant challenges, primarily due to their restricted mouth opening, which complicates airway management. Standard intubation techniques are frequently impractical, necessitating the use of alternative methods. Fiber-optic nasotracheal intubation is the preferred method, conducted under sedation or general anesthesia while preserving spontaneous breathing. This technique enables anesthesiologists to visualize the airway and securely position the breathing tube without necessitating full mouth opening. 17
Significance of Pre-operative Evaluation
A comprehensive pre-operative assessment is crucial for addressing potential challenges. Imaging studies, including CT scans, are frequently employed to evaluate the severity of ankylosis and to inform the optimal surgical strategy. Due to the complexity of airway management in these patients, it is essential to be prepared for unforeseen challenges by ensuring that emergency equipment, including tracheostomy kits, is readily accessible.
Considerations for Post-operative Care
Post-surgery, it is essential to monitor for airway swelling and to manage pain effectively. Effective pain management is crucial for promoting early jaw movement, thereby aiding in the prevention of re-ankylosis of the joint.
Employing a strategic, multidisciplinary approach enables healthcare providers to effectively tackle the distinct challenges associated with TMJ ankylosis in children, thereby enhancing their functional outcomes and overall quality of life.
Mandibular Distraction Osteogenesis
Mandibular distraction is a surgical procedure aimed at lengthening the mandible through the gradual distraction of the bone segments. This technique is often utilized in cases of congenital deformities or after trauma to restore function and aesthetics. Mandibular distraction osteogenesis (MDO) is a surgical intervention employed to address hypoplasia of the mandible, frequently associated with conditions such as Pierre Robin sequence and Treacher Collins syndrome. Infants with these conditions frequently exhibit reduced lower-jaw size (micrognathia) and a propensity for the tongue to retract, potentially obstructing the airway and complicating respiration. Airway management, both pre-operatively and post-operatively, presents significant challenges.
Detailed imaging is essential for understanding the extent of the condition and planning the optimal surgical approach. In severe cases, physicians may need to conduct an awake fiber-optic intubation to safely secure the airway while minimizing distress and complications. A tracheostomy may be considered in advance or as an emergency measure if there is a significant risk of airway obstruction post-surgery. 18
Orthognathic Surgery
Orthognathic surgery is conducted to rectify substantial jaw misalignments that may impact respiration, mastication, and articulation. Managing the airway during surgery can be challenging due to the necessity of accessing the mouth in these procedures. Nasal intubation is typically favored as it maintains an unobstructed oral cavity for the surgical team. In certain instances, where nasal or oral intubation is not feasible, submental intubation may be required.
Post-surgery, swelling may pose a significant risk, potentially obstructing the airway. Consequently, patients are frequently monitored in the intensive care unit (ICU), with the medical team prepared to intervene promptly in cases of respiratory distress. In certain circumstances, reintubation or a tracheostomy may be required to facilitate a safe recovery. 19
Craniosynostosis Surgical Intervention
Craniosynostosis surgery aims to rectify the premature fusion of cranial bones, which may influence an infant’s head morphology and cerebral development. These procedures present distinct airway challenges, resulting from the associated structural abnormalities. Infants undergoing this surgery face an increased risk of respiratory complications; therefore, a comprehensive airway assessment prior to the procedure is crucial to anticipating potential challenges.
Oral intubation is typically the preferred technique; however, due to the risk of significant blood loss and post-surgical edema, the anesthesia team must be adequately equipped with airway management tools. 20 Post-operative monitoring is essential for the early detection of respiratory complications and the provision of timely intervention as necessary.
Trauma
Maxillofacial trauma in children frequently necessitates surgical intervention to address fractures of the mandible or maxilla. These procedures require accurate realignment and stabilization, all of which must be performed under anesthesia. Airway management in these cases presents significant challenges due to possible obstructions from bone fragments, edema, or blood accumulation. Rapid sequence intubation (RSI) is frequently employed to swiftly secure the airway and minimize the risk of aspiration. 21
In cases of severe trauma, particularly those with multiple facial fractures or potential cervical spine injuries, awake fiber-optic intubation may represent the safest approach. This technique enables continuous visualization of the airway by physicians while preserving spinal stability, thereby aiding in the prevention of additional spinal injury. 22
An effective strategy for airway management in pediatric trauma begins with a thorough pre-operative assessment. This involves a thorough evaluation of the airway to detect possible obstructions, alongside the application of advanced imaging methods to devise the most secure intubation approach. A well-prepared multidisciplinary team, comprising anesthesiologists, surgeons, and critical care specialists, is essential for effectively addressing the unique challenges associated with pediatric maxillofacial trauma. 23
Pain Management
A child’s comfort and recuperation following maxillofacial surgery depend on pain management. A multimodal strategy, which combines medicines and localized nerve blocks, is often used to relieve pain without opioids. This method improves pain management and reduces negative effects.
Non-opioid Pain Relief Medications
Acetaminophen (paracetamol) is a commonly used pain medication for mild to moderate discomfort. Oral, IV, or suppository administration is possible. To reduce pain without heavier drugs, acetaminophen is often used.
NSAIDs (nonsteroidal anti-inflammatory drugs): Ibuprofen and ketorolac reduce inflammation and relieve post-surgery pain. They relieve surgical pain and reduce narcotic use.
Opioids
Morphine: Used for moderate to severe pain management, usually by IV post-surgery. It must be monitored to avoid negative effects, including respiratory problems.
Fentanyl: A potent opioid used for surgery and acute pain. Its fast onset and brief duration make it useful for acute pain treatment.
Regional Nerve Blocks Help Targeted Pain
Regional nerve blocks relieve concentrated pain, minimizing systemic medication use and speeding recovery. Common nerve blocks in pediatric maxillofacial surgery include the following: Infraorbital nerve block: Benefits procedures on the upper lip, nose, and lower eyelids, including cleft lip repairs. These locations receive focused pain alleviation. Inferior alveolar nerve block: Effectively numbs the lower jaw during treatments, including mandibular surgery and dental work. Maxillary nerve block: Effective for midface procedures such as cleft palate repairs and maxillary osteotomies, relieving upper jaw pain. Mandibular nerve block: Provides effective pain control for difficult lower jaw treatments like TMJ procedures.
Conclusion and Takeaway
Due to children’s unique airway and metabolic characteristics, pediatric maxillofacial surgery anesthetic management requires specific knowledge of anatomy and physiology.
Key Takeaways
Pediatric anatomy and physiology knowledge is essential
Smaller airways, higher respiratory risks, and immature organ function impact anesthesia and drug metabolism.
Thorough pre-operative assessment
Identifies airway difficulties and comorbidities to ensure safe anesthesia planning.
Specialized airway management
Techniques like fiber-optic or awake intubation may be required in complex cases.
Optimized pain management
A multimodal approach using non-opioid analgesics, opioids (when necessary), and regional nerve blocks ensures effective pain relief.
Emergency preparedness is critical
Pediatric patients can deteriorate rapidly; having airway rescue strategies and appropriate equipment is essential.
In conclusion, pediatric anesthesia requires specialized expertise, careful planning, and teamwork to assure safety, limit complications, and improve surgical outcomes.
Footnotes
Declaration of Conflicting Interest
The authors declared no potential conflicts of interest regarding the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Necessary ethical clearances and informed consent were received and obtained, respectively, before initiating the study from all participants.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.