
Abstract
Maxillofacial surgery encompasses a range of procedures on the head and neck, often presenting unique challenges for anesthetists due to the shared airway with surgeons and the common occurrence of difficult airways. This comprehensive overview addresses key aspects of anesthesia for maxillofacial surgery, including pre-assessment, airway management, anesthetic techniques, and postoperative care.
Keywords
Introduction
Anesthesia for dental procedures has a long history, dating back to 1846 in Boston when Dr. William T. G. Morton first demonstrated painless surgery 1 with ether for a dental extraction. In maxillofacial surgery, anesthesiologists face unique challenges due to the shared airway with surgeons. These surgeries, often necessitated by infections or trauma, encompass a wide range of procedures on the head, neck, oral, and facial regions. The primary goal for an anesthesiologist in this field is to maintain an uninterrupted airway and provide a clear surgical field for the operating team. A thorough patient history and examination are crucial, as individuals undergoing maxillofacial surgery frequently present with more complex airway challenges compared to other types of surgeries. This history should include any previous surgeries and treatments like chemotherapy or radiotherapy, which can alter tissue characteristics and complicate direct laryngoscopy.
Pre-assessment and Optimization
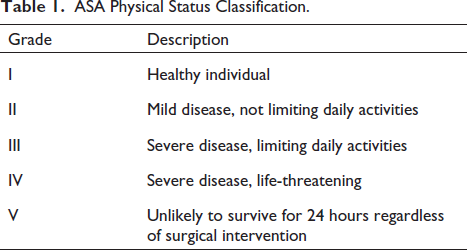
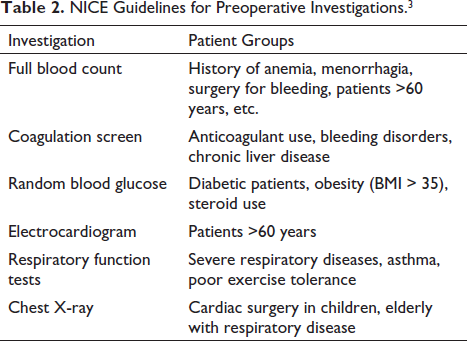
Pre-assessment is crucial in understanding anatomical alterations and reducing patient anxiety. 2 Patients range from infants to the elderly with varying comorbidities. Special attention is given to those with an ASA (American Society of Anesthesiologists) physical status of three or above. Airway examination includes assessing the Mallampati score, interdental distance, thyromental distance, neck movements, and pharyngeal structures. The ASA physical status classification helps in assessing patient fitness for surgery (Tables 1 and 2).
ASA Physical Status Classification.
NICE Guidelines for Preoperative Investigations. 3
Types of Maxillofacial Surgery
Maxillofacial surgery can be categorized into infective, traumatic, cancer, and craniofacial surgery. Each type presents specific challenges and complications, such as airway compromise, hemorrhage, and trismus in trauma cases, or the need for extensive resection and reconstruction in cancer surgeries.
Odontogenic Infections
The process begins with tooth decay and progresses to pulpitis, which is the inflammation of the nerve chamber at the center of the tooth. The infection then spreads to the bones, causing perforation of the bone cortex into the subperiosteal region. At this stage, the infection may either resolve, become localized, and form an abscess, or continue to spread. Despite advancements in microbiology and antibiotic therapy, the treatment of head and neck infections often necessitates surgical intervention. Complications: Cysts, sinusitis, Ludwig’s angina, cavernous sinus thrombosis, mediastinitis.
Trauma: (Most Common Cause of Facial Trauma) 4
Understanding the mechanism of injury is crucial in evaluating the status of patients with trauma. 5 Maxillofacial injuries can result from either blunt or penetrating trauma. Low-force injuries, often arising from interpersonal altercations, typically affect the nasal bones and zygomatic arch without usually impacting the airway. In contrast, high-force injuries, such as those from motor vehicle accidents or high-velocity weapons, can lead to fractures of the mandible or maxilla and are more likely to compromise the airway.
Blunt injury: Facial fractures from blunt injuries typically result in minor bleeding from the nose or mouth. Circulatory shock is rare in cases of maxillofacial injury alone; if significant resuscitation is required, other sources of blood loss should be investigated. 6 The most commonly fractured site in blunt and penetrating laryngeal injuries is the thyroid cartilage (47%), followed by the arytenoid cartilage (24%), and the cricoid cartilage (22%). 7
Penetrating injury: Penetrating facial injuries encompass a range of traumas and pose multiple management challenges. The two primary types of penetrating facial trauma are gunshot wounds and stab wounds. Stab wounds most commonly injure the trachea. Approximately one-third of upper airway injuries involve the larynx, with the cervical trachea accounting for the remaining two-thirds. 8
Oral Cancer Surgery
Oral cancer ranks as the sixth most common cancer globally 9 and accounts for approximately 2% of all cancer-related deaths. In India, it is the most prevalent cancer among men. 10 The primary risk factors for this cancer include smoking and alcohol consumption, which seem to have a synergistic effect. Additional risk factors are chewing tobacco, poor oral hygiene, and exposure to wood dust. The incidence of head and neck cancers has risen over the past decade, partly due to the increased transmission of the human papillomavirus linked to orogenital sex. 11 The staging of head and neck cancers is based on the tumor, node, and metastasis system, which is instrumental in planning treatment and predicting outcomes. Cancer surgery typically involves the surgical resection of head and neck cancers and reconstruction, which may include bone grafting and microvascular free tissue transfer. These procedures are often lengthy and may involve rotational or free-flap surgeries.
Craniofacial Surgeries
Craniofacial surgeries focus on the craniofacial region, which includes the skull, orbits, forehead, nose, maxilla, mandible, ears, tongue, and lips. This area can be affected by congenital malformations, inflammation, neoplasms, and trauma.12, 13 In adults, the most common craniofacial procedures involve temporomandibular joint and orthognathic surgery.
Congenital malformations in the craniofacial region include craniofacial clefts and faciocraniosynostosis.
Craniofacial clefts: These clefts primarily arise from developmental anomalies during the embryonic stage. They can be categorized into predominantly cranial, predominantly facial, or a combination of both, known as craniofacial, with the palpebral tissue serving as a reference line. Common types of facial clefts include cleft lip, cleft palate, cleft nose, Treacher-Collins syndrome, and orbitomaxillary cleft. Other forms of craniofacial clefts encompass cranial bifidum, hypertelorism, and orbital dystopia.
Faciocraniosynostosis: This condition occurs due to the premature fusion of cranial sutures, resulting in an abnormal skull shape. The specific type of faciocraniosynostosis depends on the location and number of sutures involved. 14 Examples include brachycephaly (short skull) in bilateral coronal synostosis, scaphocephaly (boat-shaped skull) in sagittal synostosis, trigonocephaly in metopic synostosis, and plagiocephaly in unilateral coronal synostosis.
Mandibular micrognathia: This condition, characterized by a receding mandible, can lead to difficulties in breathing and feeding. It is typically corrected through elongation osteotomy performed on the mandible’s body, followed by bone grafting. This procedure is usually conducted between the ages of 6 and 9 to prevent dental malocclusion. 15
Airway Management
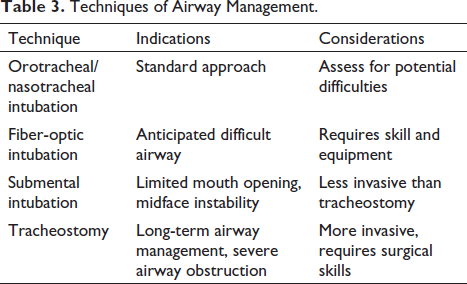
Airway management is a critical aspect, requiring a tailored approach based on the patient’s condition and the type of surgery. Techniques include orotracheal/nasotracheal intubation, fiber-optic guided intubation, submental intubation, and tracheostomy (Table 3). Awake intubation may be indicated in cases of anticipated difficult intubation. Despite advances in airway management techniques, performing surgery in the maxillofacial region under general anesthesia continues to present distinct challenges for anesthesiologists. The maxillofacial area, being a shared operative field for both surgeons and anesthetists, 16 poses unique difficulties for these medical specialists.
Techniques of Airway Management.
Blind Nasotracheal Intubation
Blind nasotracheal intubation is a technique used for managing difficult airways, particularly in patients with restricted mouth opening or damaged teeth. 17 This technique requires expertise and includes several aids:
Listening to breath sounds directly through the endotracheal tube (ETT).
Inflating the tracheal cuff to guide the tube into the trachea.
Monitoring end-tidal carbon dioxide levels.
Contraindications for blind nasotracheal intubation:
Increased potential for bleeding.
Midface instability.
Likelihood of prolonged intubation.
Presence of basilar skull fractures.
Apnea or imminent respiratory arrest.
Fiberoptic Intubation (FOI)
FOI, first performed in 1967, is the standard for managing awake, spontaneously breathing patients with anticipated difficult airways. 18 It involves using a flexible fiberoptic device to place an ETT through the oropharynx or nasopharynx.
Contraindications for FOI:
Lack of time.
Inadequate airway skills.
Patient refusal or non-cooperation.
Coagulopathy.
Heavy airway secretions.
Near-total upper airway obstruction (unless for diagnostic purposes).
Video-assisted Laryngoscope
Video laryngoscopes, which provide a better view than direct laryngoscopy, are increasingly used for both routine and difficult airway management. They are particularly useful in patients with limited mouth opening or distorted upper airway anatomy. 19
Contraindications for video-laryngoscope:
Inadequate operator experience.
Restrictive mouth opening.
Traumatic injury or deformity of the larynx and posterior pharynx.
Obstruction of the camera lens by vomit, secretions, or blood.
Laryngeal Mask Airway (LMA)
In recent years, the supraglottic device has gained popularity as an alternative to mask anesthesia, nasal airway ventilation, or endotracheal intubation. It is used in various procedures, including simple dental extractions, nasal surgeries, zygomatic surgeries, and other superficial facial operations. 20
The use of a supraglottic device in oral surgery requires close collaboration between the anesthetist and the surgeon to maximize benefits and minimize risks. This device limits access to the surgical field, especially for procedures involving the posterior teeth. While LMAs do not completely prevent aspiration, the risk of aspiration increases if patient ventilation exceeds 20 cm of water.
Contraindications for LMA:
Inability to open the mouth.
Complete upper airway obstruction.
Increased risk of aspiration.
Abnormalities in supraglottic anatomy.
Retrograde Intubation
Retrograde intubation is indicated for patients with severely limited mouth opening where traditional laryngoscopic or blind techniques are unsuccessful. It involves the introduction of a wire into the larynx through a cricothyroid puncture.
Contraindications for retrograde intubation:
Unfavorable anatomy in the cricothyroid area.
Significant coagulopathy.
Laryngotracheal disease (stenosis, malignancy, infection).
Submental Intubation
Submental intubation is a practical and less invasive alternative to tracheostomy for securing airways when orotracheal and nasotracheal intubation is not feasible. This technique involves passing the ETT through a surgical incision made on the floor of the mouth. It has been effectively utilized in the anesthetic management of both trauma and elective orthognathic surgery patients, demonstrating a low complication rate. The FASTRACH ETT, designed for use with the intubating LMA, is particularly suitable for submental intubation due to its reinforced structure and easily removable connector.
Submental intubation is contraindicated in patients with severe neurological deficits, those requiring long-term airway support and maintenance, and individuals with a history of severe keloid formation.
Surgical Airways
Surgical airways, such as cricothyroidotomy and tracheostomy, are employed in high-risk scenarios where basic airway management techniques are unsuccessful. Cricothyroidotomy is specifically indicated in situations where ventilation or intubation is not possible, in cases of impending or acute complete airway obstruction, and in instances of acute oropharyngeal bleeding. However, it is contraindicated in patients under the age of 12 and in cases involving tracheal transection.
Tracheostomy:
Used for creating a surgical airway through the tracheal wall.
No absolute contraindications.
Maintaining a Secure Airway
Ensuring the security of the orotracheal tube is challenging in maxillofacial surgery. The tube must be placed to avoid obstructing the surgical field and ensure easy access for the anesthetist. Precautions include preventing inadvertent dislodging, disabling, occluding, or kinking of the ETT and LMA.
ASA Standard Basic Intraoperative Monitoring
The ASA recommends the following minimum standard monitoring for all patients undergoing surgery under anesthesia:
Pulse oximetry: Measures the oxygen saturation level in the patient’s blood.
Electrocardiogram: Monitors the heart’s electrical activity.
Non-invasive blood pressure monitoring: Tracks the patient’s blood pressure without the need for invasive procedures.
Capnography: Measures the concentration of carbon dioxide in exhaled air, indicating the patient’s ventilatory status.
Anesthetic Technique
General anesthesia in maxillofacial surgery is challenging due to the shared surgical field. The choice of anesthetic agents, muscle relaxants, and pain management strategies must be carefully considered. Maintenance of anesthesia often involves a combination of volatile agents, opioids, and intraoperative steroids.
Preoperative Preparation for Awake Intubation in Maxillofacial Surgery
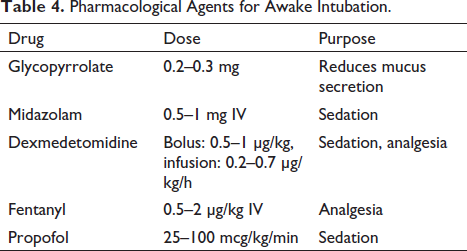
Preoperative preparation for awake intubation, a critical component in maxillofacial surgery, involves both physiological and pharmacological strategies to ensure patient comfort and safety (Table 4).
Pharmacological Agents for Awake Intubation.
Physiological Preparation
The success of awake intubation significantly depends on the patient’s understanding and cooperation. Educating the patient about the procedure helps in reducing anxiety and discomfort. Informed consent, detailing the intubation process, is a vital step in psychological preparation.
Pharmacological Preparation
Pharmacological preparation aims to alleviate anxiety, ensure a clear airway, and prevent aspiration.
Anesthesia Application to the Airway
Local anesthesia is essential for patient comfort during awake intubation. It can be achieved through topicalization, nerve blocks, or a combination of both.
Topicalization: Application of lidocaine or benzocaine using an atomizer, nebulizer, or direct swabbing.
Nasal route: Mixing phenylephrine or Afrin spray with lidocaine for vasoconstriction and anesthesia.
Common Airway Blocks
Glossopharyngeal nerve and lingual branch block: Application of 1% lidocaine at the tonsillar pillar to suppress the gag reflex.
Superior laryngeal block: Injection of 1% lidocaine through the thyrohyoid membrane to anesthetize the larynx.
Transtracheal block: Injection of 4% lidocaine through the cricothyroid membrane to anesthetize the lower airway.
Airway Management in Maxillofacial Surgery
Securing the orotracheal tube during maxillofacial surgery is a complex task. Challenges such as blood from the surgical area, patient saliva, and the impact of disinfectant solutions on tape adhesion make maintaining a secure airway difficult. Additionally, frequent repositioning of the patient’s head by surgeons can compromise the stability of the orotracheal tube. Anesthesiologists must ensure that the patency of the difficult airway is not compromised once it is successfully secured. Effective pre-planning, including the use of long circuit tubing and gas monitoring lines, is essential, particularly as the patient’s head is often positioned away from the anesthesia machine. 21 The ETT and LMA must be positioned to avoid obstructing the surgical field while remaining accessible for rapid airway management.
Use of Throat Pack
Throat packs are commonly used in airway surgeries to prevent blood and debris from soiling the airway, which can cause complications during emergence from anesthesia. They also help reduce cuff leaks around the tracheal tube. Safe placement and removal of the throat pack are crucial, and both should be carefully documented to ensure patient safety.
Maintenance of Anesthesia
After successful intubation, anesthesia is maintained using muscle relaxants, volatile agents (such as sevoflurane in air or nitrous oxide), and opioids. Intraoperative steroids, typically dexamethasone, are administered to minimize postoperative swelling and reduce nausea and vomiting. For procedures lasting more than 30–45 minutes, active warming is required to maintain normothermia, thereby preventing shivering during emergence, which can be uncomfortable for patients and increase their oxygen demand. Normothermia is maintained using forced air warming blankets, under-heating mattresses, warmed fluids, and heat and moisture exchangers.
Postoperative Management
The decision to extubate after surgery is made on a case-by-case basis, in consultation with the surgical team. Safe extubation requires a thorough reassessment of the airway and a well-planned strategy. Extubation carries risks such as laryngeal spasms or airway obstruction due to edema and bleeding. Careful laryngoscopy and suction should be performed, and any throat pack should be removed prior to extubation. In patients with significant swelling, it may be advisable to keep them intubated and ventilated until extubation is deemed safe. Special consideration is needed for patients with compromised airways, such as those who have undergone neck dissections, uvulopalatoplasty, mandibular resections, or maxillomandibular fixation. The primary goal in the immediate postoperative period is to maintain ventilation to prevent hypoxia and hypercapnia. Supplemental oxygen is required postoperatively, with high-risk patients needing it for a longer period. Monitoring fluid balance following major surgery is essential, with fluid input and output closely monitored and a cumulative fluid balance recorded.
Pain Management
Effective pain management is a critical aspect of postoperative care. A combination of non-opioid analgesics, non-steroidal anti-inflammatory drugs, and local anesthetic infiltration by surgeons is often used. Patient-controlled analgesia with morphine or fentanyl provides effective pain relief but is rarely required. Pain levels should be regularly assessed using a pain score chart, such as the Visual Analog Scale for adults or the Faces Pain Rating Scale for pediatric patients.
Complications
Postoperative complications in oral and maxillofacial surgeries can significantly increase morbidity and mortality. Early postoperative hematoma formation, although uncommon, can be a potentially airway-threatening complication, especially following neck surgery, thyroid resection, and floor-of-the-mouth surgeries. Postoperative nausea and vomiting are common and distressing for patients. 22 The ASA recommends the prophylactic use of antiemetics to improve patient comfort, satisfaction, and reduce discharge time. Common antiemetics include antiserotonergics (ondansetron), antihistamines (cyclizine), antidopaminergics (prochlorperazine), and dexamethasone. 23
Conclusion
Anesthesia for oral and maxillofacial surgeries presents significant challenges for anesthesiologists. Careful assessment, thorough preparation, close collaboration with the surgical team, and effective anesthesia management are crucial to enhance patient safety and improve perioperative outcomes.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Necessary ethical clearances and informed consent were received and obtained respectively before initiating the study from all participants.