
Abstract
In the conventional method of fixation of symphyseal fractures, 2 miniplates are fixed in the interforamina region of the mandible at the lateral cortex. However, with the better understanding of tension and compression areas defined according to the place of energy insertion, it is now possible to fix miniplates at the lower border of the mandible. In this study we assumed that the application of perpendicular miniplates, in contrast to the placement of the plates on the lateral surface of the mandibular cortex, will constrict the motion in horizontal as well as vertical planes leading to better functional outcomes, which can be evaluated by measuring bite forces. The results obtained were affirmative with the hypothesis.
Introduction
Fractures of the mandible lead to the changes in the skeletal configuration and in components of the masticatory system. The treatment of the mandibular fractures becomes complex because of the involvement of various factors especially muscles of mastication, inferior dental nerve, and teeth.1, 2 In the conventional method of fixation of symphyseal fractures, according to Champy’s 3 ideal line of osteosynthesis, 2 miniplates are fixed in the interforamina region of the mandible at the lateral cortex. However, with the better understanding of tension and compression areas defined according to the place of energy insertion, it is now possible to fix miniplates at the lower border of the mandible. 4 In this study we are assuming that the application of perpendicular miniplates, as contrast to the placement of the plates on the lateral surface of the mandibular cortex, will constrict the motion in horizontal as well as vertical planes. This will result in better stability on the lateral surface of the mandible when compared to the conventional plates. A useful indicator of the functional state of the stomatognathic system and the load on teeth is the maximum bite force. 5 So, considering the inadequate studies in the literature regarding comparison of various fixation techniques in the mandibular anterior region (interforamina) and its association with bite force, this study aims to compare the clinical outcome of the open reduction and internal fixation of symphysis fracture with conventional and perpendicular plating system along with changes in the bite force at varying intervals among both the groups.
Materials and Methods
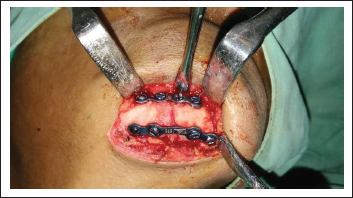
A prospective interventional study was designed including 40 patients of isolated mandibular symphysis fractures and institutional ethical clearance was obtained. Patient with preexisting systemic illness or conditions affecting musculoskeletal system and patients with partial dentition or edentulous patients were excluded. Informed consent was obtained from all the patients. Patients were randomly allotted to either of the 2 groups which were created based on the type of fixation applied. Group A patients were treated with conventional 2 titanium miniplates fixed with 2.0 mm monocortical screws (Loyal, Mumbai, India) at the lateral cortex, and group B patients were treated with 2 titanium miniplates applied perpendicular to each other with 1 plate at the lateral cortex and another along the inferior border and fixed using 2.0 mm monocortical screws (Loyal, Mumbai, India). Fractures of Group A patients were exposed intraorally and those of Group B were approached either through the existing laceration or transcutaneously. After obtaining anatomical reduction of the fracture fragments, plates were fixed. In group A, 2 plates were applied to overcome the torsional forces. The first plate was placed below a line joining mental foramina and the second plate was placed above it maintaining 4 to 5 mm distance from the first plate and below the apices of the teeth roots. In group B, a 2.00 mm infraorbital miniplate was placed along the inferior border of the mandible first followed by a conventional 2.00 mm miniplate above the imaginary line joining the mental foramina and another (Figure 1). The incision was closed in layers and the patient was extubated after applying pressure dressings.
The Device Used to Measure Bite force.
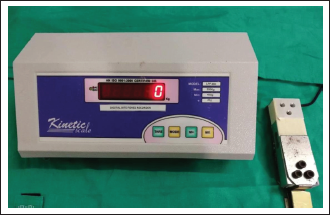
Bite forces were measured preoperatively, immediately postoperatively and at first, second, and fourth week intervals and at the completion of 3 months after surgery. A bite force recorder which was developed at the Division of Ergonomics, Department of Mechanical Engineering, Aligarh Muslim University, Aligarh, was used for this purpose. The device consisted of a transducer based on Wheatstone bridge which worked as a pressure-sensing device, an adjustable knob for adjusting zero of the display and a digital electronic display. For the application of force, the equipment consisted of a metallic fork covered with disposable cushioned adhesive tape (Figure 2). The equipment was connected to 250 V electrical supplies for charging the equipment. The bite force was recorded by asking the patients to bite on a fork with maximum pressure using their incisors and then by molars of both the sides. Each patient was asked to sit erect and relaxed keeping the head in Frankfort horizontal plane parallel to the ground floor. 3 successive readings were taken on all the sides after giving a rest of 10 s on each side and the highest value of the bite force was considered as maximum bite force. Unpaired t test was utilized to statistically analyze the recordings.
Apllication of Two Miniplates Perpendicular to each other.
Results
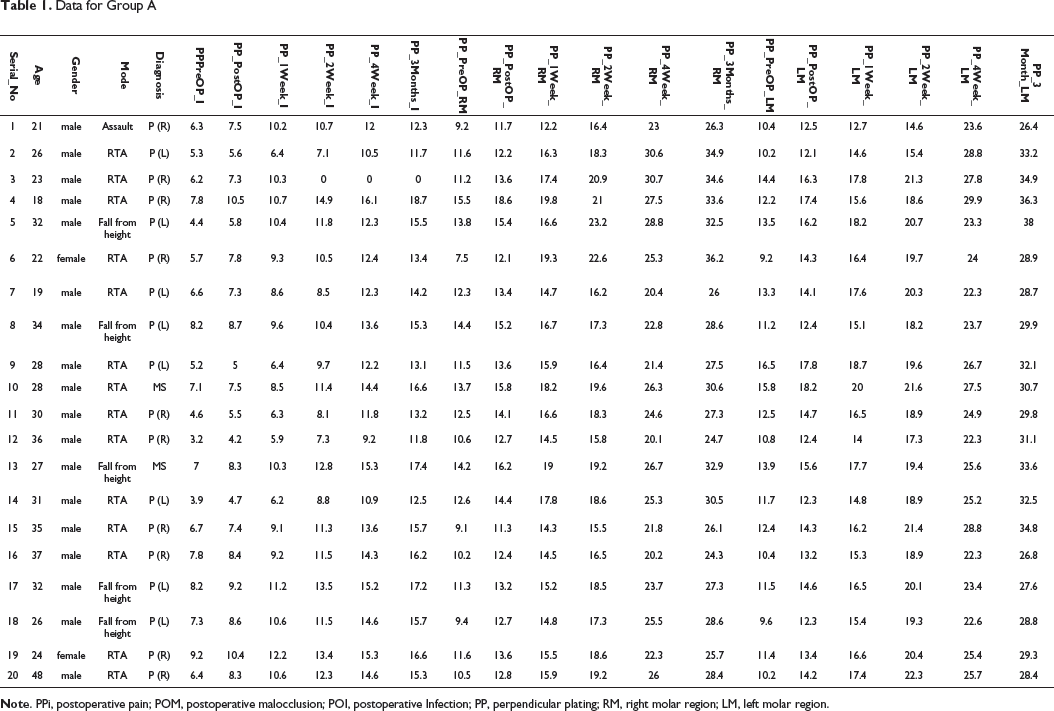
Data for Group A
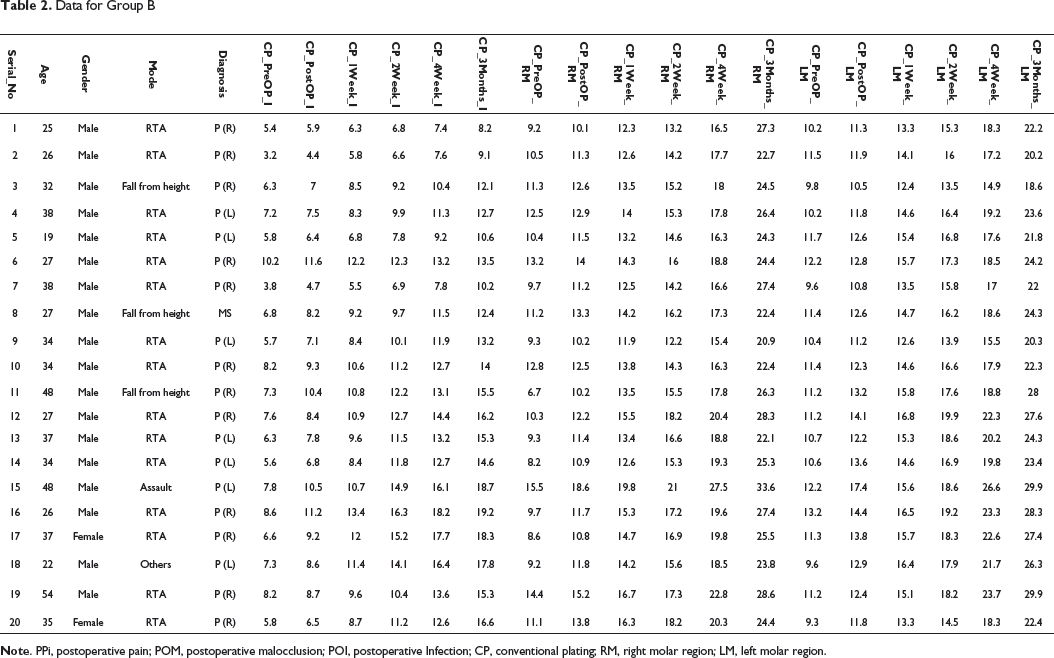
Data for Group B
Discussion
Several choices which are available for the internal fixation of symphysis/parasymphysis fractures via extraoral or intraoral approach include lag screw, reconstruction plate, 3D plates, double miniplates, and single stronger bone plate. However, there are not many strong evidence in the literature which state the superiority of 1 rigid internal fixation technique for treating simple (linear) symphysis fractures over another.
There are certain advantages of perpendicular plating when compared to conventional method which include easy application, simplified adaptation to bone without distortion or displacement of the fractured segment. The main disadvantage with conventional plating is that the plate must be perfectly adapted to the underlying bone to prevent alterations in the alignment of fractured segments which may lead to malocclusion. The adaptation of conventional miniplates to the contours of bone can be compensated as the human mandible shows an uneven surface. 6 Repeated bending may cause excessive strain to the material and thus create predetermined breaking points. 7 Also, the inappropriate adaptation of conventional plates causes displacement of the mobile bony fragments when the screws are tightened and can decrease primary stability. Theoretical advantages proposed include less precision required in plate adaptation because of the internal/external fixator, less alteration in osseous or occlusal relationship on screw tightening, and greater stability across the fracture site. 8
We performed clinical testing on patients of symphyseal fracture reporting to our department and evaluated the efficacy of the 2 different plating systems using bite force as a useful indicator of the functional state of the stomatognathic system and the load on teeth. 9 Bite force is the net result of different components (muscles, bones, and teeth) acting in a coordinated manner. Trauma to the muscle of mastication or to protective neuromuscular mechanisms of the masticatory system during the surgery may lead to significant reduction of bite forces after the treatment of mandibular fractures. Maximum bite force can be considered as a major factor in influencing the success of treating mandibular fractures. A maximum voluntary force which also gives the idea of different forces that are countered in a fractured mandible may be in order of 15.3 Kilopascal (kPa) in the incisor and 48.3 and 49.3 kPa in the left and right molar regions. 10 Gerlach evaluated maximum bite forces in 22 patients with mandibular angle fracture. These patients were treated with miniplate osteosynthesis according to Champy. 7 For evaluating the load resistance between the incisors, canines, and molars, an electric test procedure was carried out 1 to 6 weeks following the surgical procedure. A similar test was performed in 15 controls also. The test revealed that 1 week postoperatively only 31% of the maximal vertical loading found in controls was registered. These values increased to 58% at the sixth week postoperatively. 11
In our study, there was an increase in the bite force in both the groups at varying intervals. But the values of bite forces at incisor, left molar region, and right molar region were more in group B than in group A. However, the bite force obtained in patients with mandibular fracture, who were treated either by conventional or perpendicular plating method, failed to meet the required maximum voluntary bite force as reported by Ellis and Thockmorton. 12 The maximum bite force recorded in our study at incisor, right molar, and left molar regions was on the lower side when compared with bite forces of healthy individuals as reported by Ahmed et al and Gupta et al in their respective studies.13, 14 The values observed by us were comparable to the study performed by Kshisagar et al who also observed a trend of increased bite force with increase in age in males, but it was not true for females. 15
Trauma to the muscle of mastication or to protective neuromuscular mechanisms of the masticatory system during the surgery may lead to significant reduction of bite forces after the treatment of mandibular fractures. Another major factor is the patient’s willingness to bite hard. Some patients are afraid to use their jaws vigorously, especially during the first postoperative week may be attributed to their mental attitude as well as to the comfort of the teeth. Hence, this can lead to very low values of bite forces recorded at the end of the first postoperative week. This can also be supported by the fact that the first protective mechanism which comes into play after fracture is muscle splinting, where selective components of the neuromuscular system are activated or deactivated to take off the forces acting on the damaged bone. Also, a bite force is related to several factors such as pain, tactile impulse, and pressure perception in periodontal ligament and number of remaining teeth which may limit the patient’s ability to apply preinjury bite force.16, 17
There was a significant increase in the bite force values at all intervals of time at which it was measured, but the increase in the bite force values from the fourth week to 3 months was less. This may be attributed to the phenomenon of regeneration of nerve and re-innervation of reflected periosteum with return of pain sensation. 12
The present study shows that fractured mandibular symphysis when treated with perpendicular plates will lead to improved and optimal functional rehabilitation of the patient when compared with conventional 2 plate fixation. Better stability at fracture site was observed with this combination allowing greater loading and functional use of the jaw during the healing phase as shown by significantly improved bite forces. The only demerit of the method of applying perpendicular plates is that the fracture must be approached through extraoral approach for applying plates which will result in the creation of a scar, although inconspicuous.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Necessary ethical clearances and informed consent was received and obtained respectively before initiating the study from all participants.