
Abstract
Mucormycosis is a rare fatal fungal infection which has caused havoc in the present scenario of COVID-19 pandemic usually infecting post-COVID-19 recovered patients who were treated with corticosteroids or those who had ill regulated diabetes or immunocompromised states. The causative organism is a saprophytic fungus of the order mucorales and has a high affinity for blood vessels causing endothelial damage and thrombosis which results in necrosis of the affected tissues. Rhinocerebral mucormycosis is the most common infection being diagnosed in the current cases requiring the combined surgical approaches of an ENT Surgeon, a Maxillofacial surgeon and a Neurosurgeon. The disease may progress to involve the cranium thereby increasing the mortality rate. The first line of management in mucormycosis is antifungal therapy which may extend and also include surgical management by debridement/resection of the necrosed structures. In this article, we have reported a case series of 50 mucormycosis patients most of whom are post COVID, with the discussion of their demographics, affected structures, teeth mobility, blood sugar levels and neutrophil count with detailed description of the cases.
Introduction
Ever since the advent of novel corona virus epidemic in 2019, a myriad of associated diseases have gripped the post-COVID patients due to the inadvertent use of glucocorticoids to control the viral disease which leads to immunosuppression leaving the patient vulnerable to a variety of secondary opportunistic bacterial and fungal infections of which mucormycosis is one of the most fatal infections. Mucormycosis is a fungal infection that invades blood vessels which is caused by a saprophytic fungi which belong to the order of mucorales and the family of mucoracea. It is commonly found in waste materials like decayed food or organic matter as well as soil. It is an opportunistic infection which becomes pathogenic when people with a non-intact immune system take in these fungal spores through either the nasal passage, oral passage, or lacerated mucosa of the oral or nasal cavity. Individuals with a history of having diabetes are at a higher risk compared to non-diabetic individulas. 1 Pathologically, the fungus shows a great attraction for blood vessels especially the arteries. The fungus invades the arterial microstructure and causes detachment of the innermost elastic lamina from the tunica media, which results in a great amount of cell damage to the arterial walls and may causes thrombosis in the affected blood vessels. The histopathology of this condition shows acute inflammation and signs of necrosis.2, 3 This fungal infection is quite time sensitive having a global fatality rate of 46%. 4 Individuals who are at risk of getting this opportunistic infection are people with diabetes, individuals who are on chronic steroid use, patients with malignancies or those who have had stem cell transplants and whose immunity has been compromised. 5 Manifestation of Mucormycosis has various clinical forms, like rhinocerebral form, gastrointestinal form, pulmonary system form, central nervous system form and disseminated kind. Rhinocerebral mucormycosis is further divided into 3 groups: rhino-orbital, rhinomaxillary, and rhino-orbito-cerebral mucormycosis. 6 Early detection, diagnosis and aggressive treatment in the form of injectable and local amphotericin b, surgical debridement of the necrosed tissues can prevent lethal outcomes and dictate the prognosis of the disease. This article aims at presenting the various extraoral and intraoral findings in post-COVID mucormycosis cases which are of particular interest from an oral and maxillofacial surgeons outlook as well as their part in the complete treatment of these patients.
Material and Methods
This is a case series of 50 patients infected with the rhino-orbito-cerebral mucormycosis with maxilla involvement which were managed at the Department of Oral and Maxillofacial Surgery, Faculty of dental sciences, KGMU, Lucknow, Uttar Pradesh which covers the patient load from most of the eastern Uttar Pradesh. Off the total of 252 patients of mucormycosis admitted to our hospital, 50 had maxillary involvement leading to the involvement of oral and maxillofacial surgeons. A majority of the patients had a history of being COVID positive in the recent past with most of them being treated with steroids thereafter. All the patients were admitted in the various mucormycosis wards of KGMU and triaging was done based on the age the patient(younger patients were preferred) and the extent of the destruction(milder diseased individuals were preferred first). The patients optimisation before any surgical intervention was done by using IV broad spectrum antibiotics, antifungals, oral hypoglycaemic drugs and/or insulin if required. The surgical debridement and/or resection of the complete or partial palate/ inferior level maxillectomies were done at our department OT.
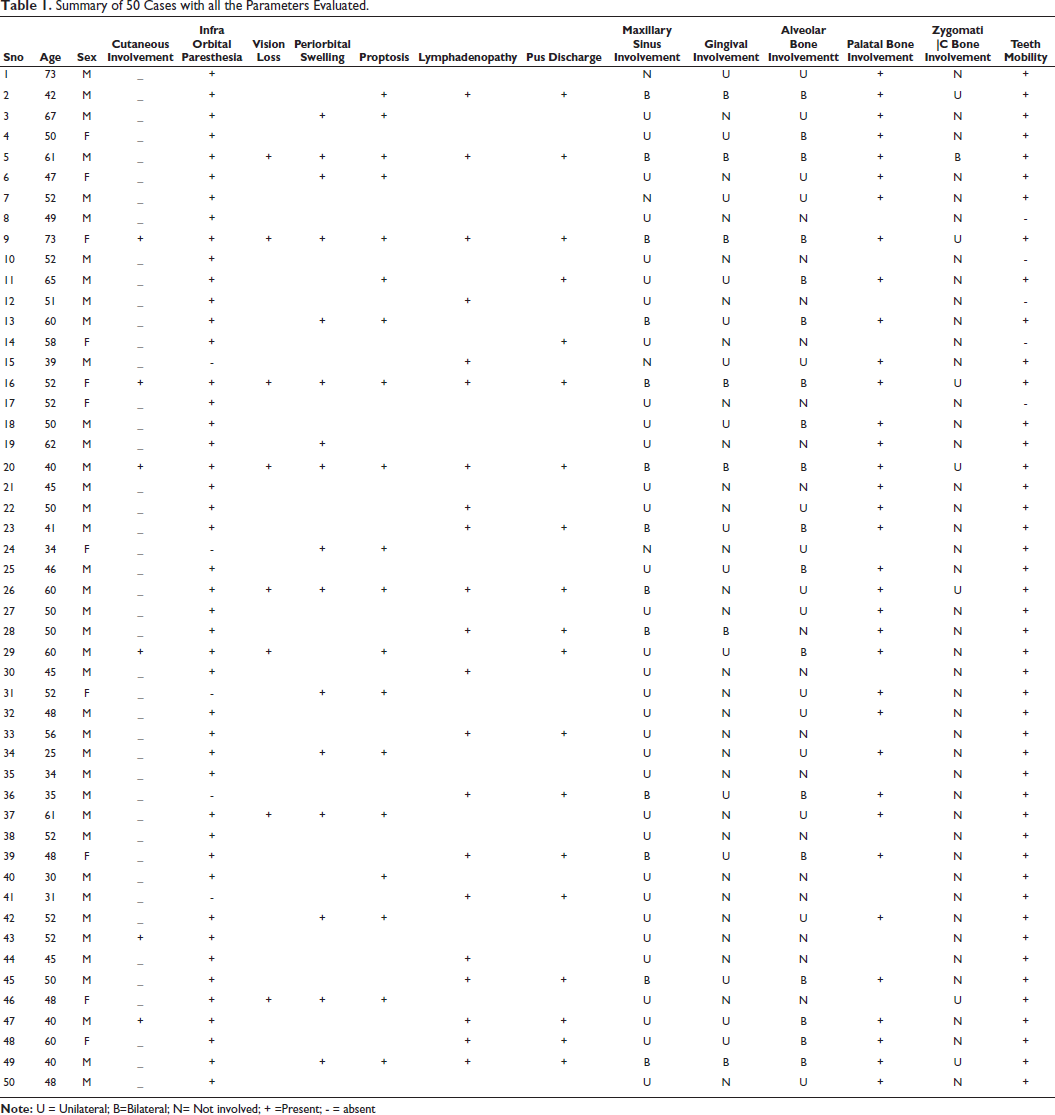
A complete summary of 50 cases with all the parameters evaluated in this article has been described (Table 1).
Summary of 50 Cases with all the Parameters Evaluated.
Results
The unprecedented spurt in the mucormycosis infection in the COVID positive and post-COVID patients in our region is clearly related to the excessive use of steroids to control the viral infection with little regard given to glycaemic levels. The incidence of finding such a huge number of patients of mucormycosis establishes this fungal disease as a separate epidemic within this global pandemic.
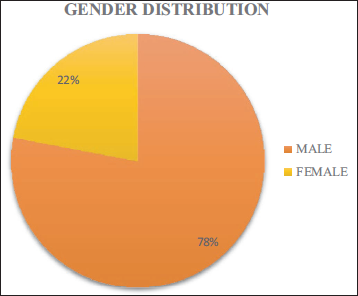
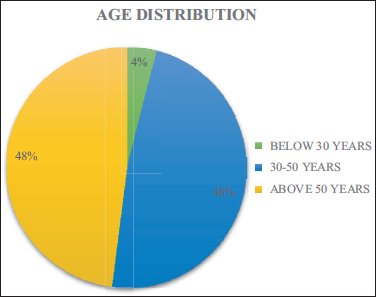
In our case series of 50 patients, a larger number (96%) were middle aged and elderly (>30 yrs) with males forming a larger part of the sample population (78%) (Figure 1 & 2, Table 2).
Showing Gender Distribution of the Patients.
Showing Age Distribution of the Patients.
Showing Age and Gender Distribution of the Patients.

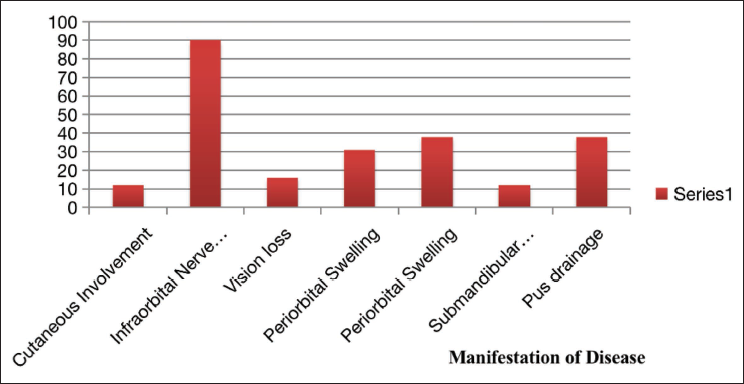
On the account of manifestation of the disease (Figure 3, Table 3)
Showing Manifestation of Disease in the Patients.
Showing Clinical Features of the Patients.

Cutaneous involvement showing necrosis of skin of head and neck region was considerably low with just 12% having skin necrosis.
Incidence of Infraorbital nerve paresthesia of the involved site was quite high with patients having 90% of infraorbital nerve paresthesia.
Ocular symptoms were relatively less with percentage of vision loss, periorbital swelling and proptosis being 16%, 31% and 38% respectively; 42% of the patients had submandibular lymphadenopathy and pus was draining out of 38% patients. Intraorally (Table 4).
Showing Involvement of Various Facial Parts of the Patients.

Maxillary sinus was involved unilaterally in 66% of patients whereas bilateral maxillary sinus involvement was seen in 26% of the patients of sample population.
Buccal gingiva was involved in 30% of patients unilaterally and 14% bilaterally.
Alveolar bone of entire maxillary arch was involved in 36% of the patients while just a single quadrant of either side was involved in 30% of the patients.
Palatal bone involvement was reported in 70% of the patients whereas just 14% and 2% of the patients had zygomatic bone involvement on uni- and bilateral sides respectively.
Teeth mobility in various grades according to miller was present in almost all the patients with 38% of the sample population having at least 5-10 teeth mobile in the maxillary arch (Table 5).
Showing Mobility of Teeth in the Patients.

Low haemoglobin and uncontrolled high blood sugar was the case in quite a few sample population but none of the patients who were electively operated on our side suffered from diabetic ketoacidosis as such (Table 6, 7).
Showing Haemoglobin Status of the Patients.

Showing Blood Glucose Status of the Patients.

Also neutropenia over an extended time period is a risk factor for mucormycosis, 18 along with immunosuppressive drugs and diabetes, however in our sample group the mean neutrophil count was within the normal range and hardly any patient showed any neutropenia (Table 8).
Showing Mean Neutrophil Count of the Patients

Discussion
Mucormycosis presents itself as variety of infections which are caused by zygomycetes, which reproduce sexually through zygospores. The fungus is a common commensal in nasal mucosa or paranasal sinuses or maybe inhaled as spores but does not wreak havoc due to body’s intact phagocytic response. 7 The fungus is responsible for the various aggressive clinical manifestations in different parts of the body when the body’s immunity is compromised. The most commonly affected patients are those with poor control over their diabetes, especially during an episode of ketoacidosis, which translates to around 88% of the cases of rhinocerebral mucormycosis. Other than diabetics, the individuals at risk are those who are immunocompromised due to malignancies, organ transplants, or those on long-term immunosuppressive medications like corticosteroids. 8
When a healthy person contracts this fungus through nasal or oral route, his body’s intact immunity prevents any fatal outcome due to limiting power of the phagocytic response of the body. However, when a person with low PMNL count contracts it, the fungal spores get a chance to germinate, form hypheas and infect the most suitable place for their growth; the paranasal sinuses. The fungus can simultaneously spread to the adjacent structures: inferiorly to the palate, superiorly into the brain and laterally with in the orbits and the cavernous sinus. It invades the blood vessel’s lamina interna causing thromboembolisms and tissue infarcts. It can lead to dire consequences such as orbital cellulitis, OAS, cerebral inflammation, brain abscess, and lastly death. 9
The commonest risk factor for mucormycosis is diabetes mellitus, especially if the person is in a state of ketoacidosis. Diabetes is associated with reduced neutrophil function, microvascular insufficiency. In episodes of ketoacidosis—the resulting Ketone bodies which are produced accentuates the fungus’ ability to utilize and produce the enzyme—ketoreductase, which is an important cofactor for its growth.10–12
Clinical presentation of the disease compromises of: rhinitis with discharge of pus, blackened necrosed sinus mucosa and/or skin, facial swelling and paresthesia, paranasal sinusitis, ophthalmoplegia with visual acuity impairment and/or blindness, proptosis, headache, stroke or hemiplegia, and compromised mental functioning.13, 14 These clinical findings most of which appear on face or in the oral/nasal cavities as well as the paranasal sinuses are easily and more commonly diagnosed by the maxillofacial surgeons who specialize in the region of head and neck. These clinical findings more or less were found in most of our patients (Figure 4, 5).
Showing Extraoral Clinical Findings of the Mucormycosis Patient.

Showing Intraoral Clinical Findings of the Mucormycosis Patient.

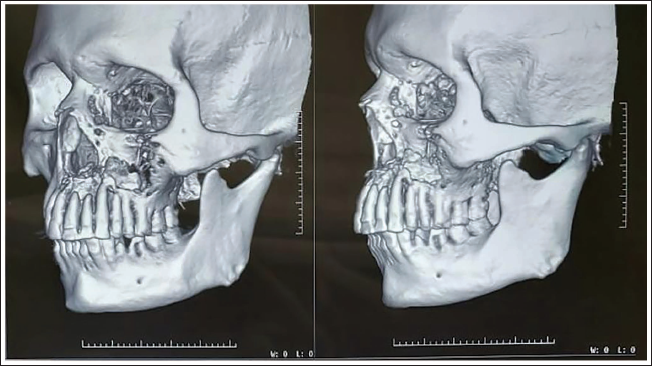
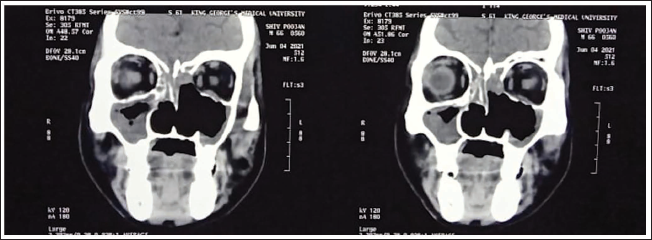
This fungal infection has a poor prognosis with the mortality rate in the range of 33.3%-80%.15, 16 Computed tomography (CT) is the basic tool for assessing the health of sinuses, although the extra-sinus spread, orbital and central nervous system involvement is best visualised by MRI. 17 The CT findings usually denote the heterogenous thickening of the mucosal linings of the affected paranasal sinuses(maxillary, ethmoid, sphenoid, frontal) which is common finding in these cases of mucormycosis. Associated thinning and rarefaction of the bones usually the maxilla, vomer, palate, floor of the orbit are also seen. If the infection invades the soft tissue around the paranasal sinuses, then soft tissue thickening of the various masticatory spaces, retroantral region, etc., can be observed in the CT scans. The CT findings showing thickening of maxillary mucosal linings, destruction of maxillary, vomer, palatal bone and infraorbital region can be appreciated in most of the cases (Figure 6, 7).
Showing Bony Involvement of Midface Bones on a 3d Reconstruction CT Scan of Mucormycosis Patient.
Showing Paranasal Sinuses and Orbital Involvement in a Coronal Section of CT Scan of a Mucormycosis Patient.
A definitive diagnosis of mucormycosis is achieved only after a biopsy and its histopathological examination has been done. KOH mounts and fungal culture examination is only used to screen for the presence of any fungus.
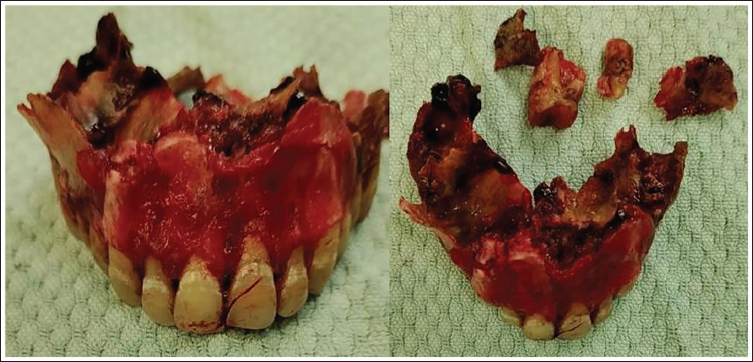
The treatment strategy incorporates eliminating the predisposing factors responsible for this opportunistic infection and improving the overall systemic condition of the patient. At our centre, the critical patients were managed in the ICU and the non-critical ones in mucormycosis wards; where they were administered IV broad spectrum antibacterial and antimycotic medication to control the fungal or any superimposing bacterial infections, insulin or OHA to keep blood glucose in check, and interdepartmental references when required. The necrosed tissues were excised by the concerned departments residents (OMFS, ENT, Ophthalmology) which helped in eliminating invasive fungi which was out of bounds for the systemic antifungal. The maxillofacial surgeons were able to reach the areas which were not easily reachable via an endoscopic method (commonly being used by the ENT surgeons) as they removed the palate/anterior maxillary wall exposing the diseased maxillary sinus, floor of orbit, lateral nasal walls, zygomatic bone etc. The removal of these non-vital structures lead to the better take up of the systemic antifungals being used (Figure 8). The standard Antifungal therapy with amphotericin B for mucormycosis at a dose of 1–1.5 mg\kg\day was used for all patients with strict monitoring of kidney functions due to its nephrotoxic nature. However, the lyposomal version of amphotericin B were given higher preference as they are less toxic and can be used for over an extended period of time with lesser side effects. Posaconazole, a drug belonging to the family of triazoles anti-fungals was used in patients who were either resistant to or allergic to amphotericin B and it was also used in adjunction with liposomal amphotericin B.
Showing Resected Maxilla of a Mucormycosis Patient.
Conclusion
The triad of COVID-19 infection, diabetes and the corticosteroids used in its treatment has led to the rise in this mucormycosis epidemic within this pandemic. Rhino-orbito-cerebral mucormycosis is an aggressive and proliferative infection usually affecting people with uncontrolled hyperglycaemia and having an immunocompromised state of health. Although the fungus is detected histopathologically and microbiologically, but one needs to be aware and suspicious to first detect the disease. Prompt diagnosis of the disease followed with rapid action to treat it may be lifesaving to the affected patients. Multifaceted approach to its treatment includes optimizing the patient’s blood glucose, swift necrosed tissue debridement, and antifungal management followed by reconstruction of the lost body structures. A maxillofacial surgeon being in the treating team plays an important role by early diagnosis of the disease during intraoral and facial examination as well as helps in the surgical treatment which is required by these patients.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
Ethical clearance was obtained from the institutional ethical committee (Ref: VIPGTSC-IIA/P35).
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
Written consent was obtained from all the patients.