
Abstract
A pilot study was conducted to analyze and compare the stability of dental implants using 2 different graft materials (autologous dentin graft and an alloplastic hydroxyapatite [HA] crystal) in the same patient. As far as we know, this study is first of its kind where socket preservation has been done using 2 different grafts in the same patient. Ten patients undergoing extraction of at least 2 teeth were selected. Atraumatic extractions were performed. Out of the 2 extraction sockets, 1 was grafted with autogenous tooth graft and other with HA crystals. Computed tomography scan was performed 3 months after grafting to evaluate bone mineral density. Primary implant stability was measured using resonance frequency analysis. It was observed that among both sites, autogenous tooth grafted sites showed better results.
Introduction
Dental extractions reduce the dimensions of alveolar bone significantly.1–3 From a restorative point of view, it is commonly recommended to perform ridge preservation procedures after tooth extraction. For this, autologous graft possessing the properties of osteogenesis, osteoinduction, and osteoconduction is considered gold standard. 4 The use of xenografts and allografts is limited due to their lack of osteogenic potential.5, 6 Moreover, these grafts are expensive, and have associated risk of transmission of various diseases.7–9
Recently, it has been demonstrated that dentin has both osteoconductive and osteoinductive potential.5, 6 Investigators have used dentin as bone fillers or volume maintainers in sinus augmentation as well as guided bone regeneration.10–12 Use of autologous dentin reduces the cost of treatment and recycles medical waste. In the present study, we have compared autologous dentin with hydroxyapatite (HA) crystals in terms of their effect on bone density and primary implant stability when used for socket preservation.
Materials and Methods
A randomized, controlled, prospective clinical pilot study was conducted in our department after obtaining institutional ethical clearance in compliance with the appropriate EQUATOR guidelines. Ten patients who required at least 2 implant placements after extractions were selected. In every patient, out of the 2 extraction sockets, 1 was preserved using autologous dentin (group A) and another was preserved using HA crystal (group B). Endodontically treated, restored, and grossly decayed were not used. Patients with diabetes, history of smoking, patients with active periodontal disease, oral pathology, osteoporosis, advanced cardiovascular disease, retinopathy or renal disease, blood dyscrasias, connective tissue disorders, liver dysfunction, auto immune deficiency, active tuberculosis, and psychosis were excluded. Patients on anticoagulant therapy, anticonvulsant therapy, steroid therapy, long-term radiation therapy, and immunosuppressors were also not included in the study. All the extractions were performed by the same surgeon under local anesthesia.
In order to prepare dentin graft, previous temporary or permanent restorations were removed. The carious portion, if present, and remnants of periodontal ligament were taken off using sterile tungsten carbide burs. The roots of molar teeth were sectioned off from the crown. The extracted tooth was then put into the sterile grinding chamber of Smart Dentin Grinder (Kometa Bio Limited) (Figure 1) after air drying and machine was turned on ultimately producing particles with size 300 to 1200 µm in its lower chamber (Figure 2). The dentin particles which were obtained following the previous step, were placed in a small sterile glass chamber and immersed in Basic alcohol [0.5 Mol NaOH and 30% alcohol (v/v)] for 10 min to dissolve all organic debris, bacteria, and toxins of the. For washing the dentin particulate, phosphate buffered saline (PBS) was used in sterile glass chamber containing the graft for about 2 to 3 min. The excess of PBS solution was absorbed using a cotton gauze. The graft was then ready for use (Figure 3). After preparation of the dentin graft, 1 of the 2 extraction sockets received this graft while other socket was packed with HA crystals with average particular size of 0.1 to 0.4 mm (G.Surgiwear Limited) (Figure 4). All the grafted sites were covered with a chorion membrane obtained from the Tissue Bank, Tata Memorial Hospital, Mumbai, India. Postoperative instructions were given and patient was prescribed a chlorhexidine containing mouthwash. Patients were recalled after 7 days for suture removal. After 3 months, patients were recalled for evaluation of bone mineral density using computed tomography and implant placement.
The Smart Dentin Grinder Used in the Study.

Process of Obtaining Dentin Particles.
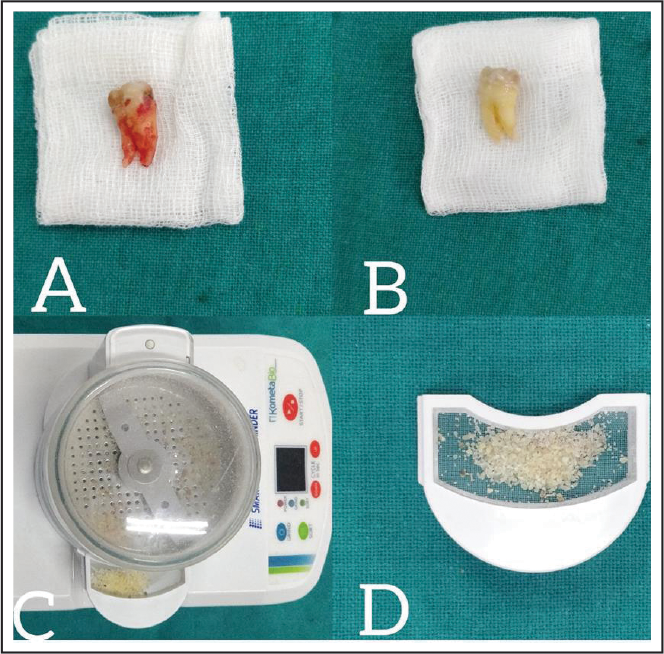
Prepared Dentinal Graft.

Socket Preservation Using HA and Dentin Graft in the Same Patient.

For implant placement, crestal incision was given to expose the alveolar bone. Using manufacture recommendations, drills were used for implant osteotomy and appropriate size tapered, and rough surface implants (Alpha Bio Tec) were placed. The primary implant stability was then assessed using resonance frequency analysis (RFA) using Penguin Resonance Frequency Analysis (Integration Diagnostics). The data obtained was statistically analyzed using SPSS 16.0 (SPSS Inc) and used for analysis of data. The significance of density (in Hounsfield Unit) and implant stability (implant stability quotient) between groups were tested by parametric test independent t test. The 95% confidence Interval and 5% level of significance was used for analysis of data.
Results
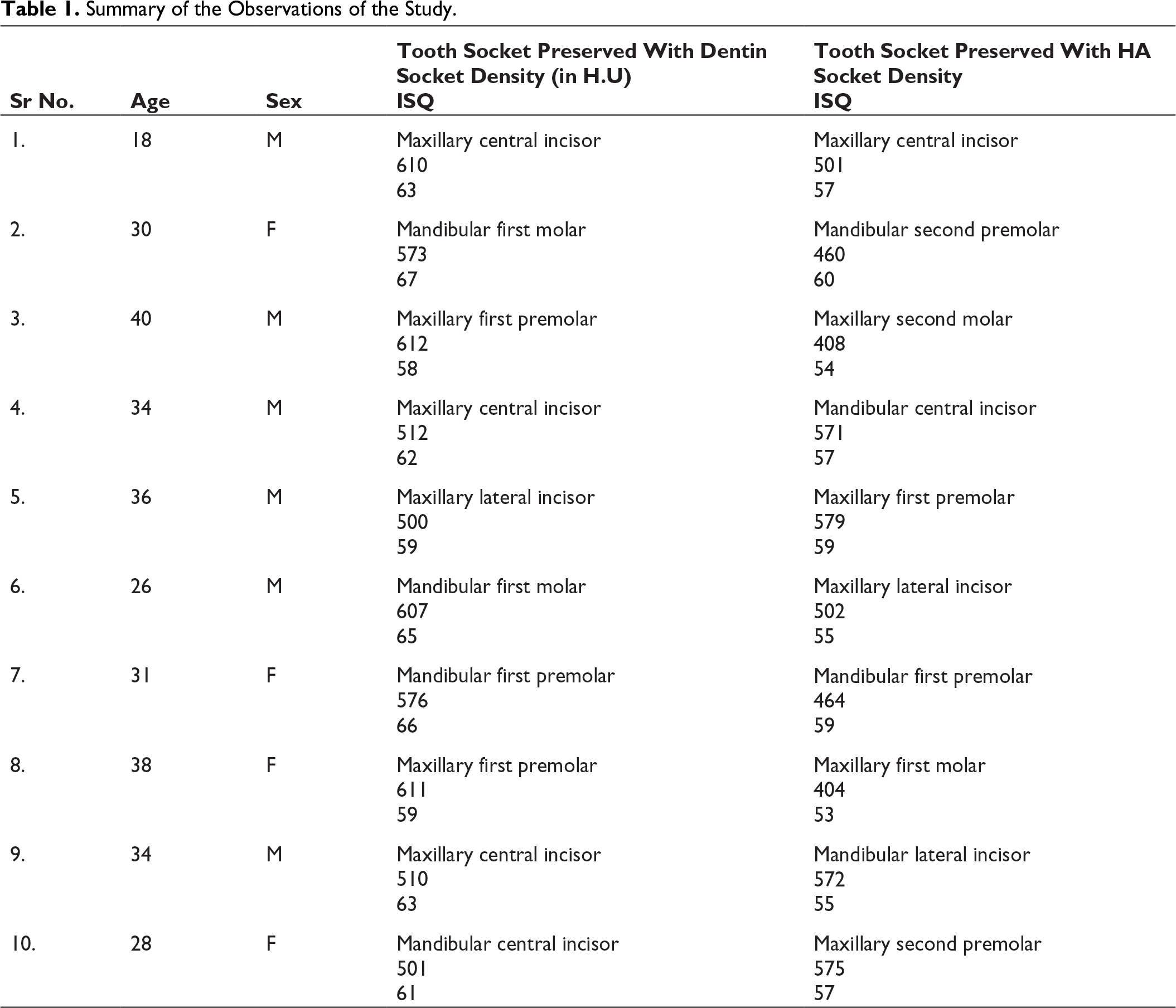
The study included 6 male and 4 female participants. Of the 20 selected sites, 10 sites were grafted with autogenous dentin and 10 with HA crystals. Among 20 grafted sites, 12 were in maxilla and 8 were in mandible—9 in anterior region and 11 in posterior region (6 central incisors—4 in maxilla and 2 in mandible; 3 lateral incisors—2 in maxilla and 1 in mandible; 5 first premolars—3 in maxilla and 2 in mandible; 2 second premolars—1 in maxilla and 1 in mandible; 3 first molars—2 in mandible and 1 in maxilla; 1 second molar in maxilla).
Summary of the Observations of the Study.
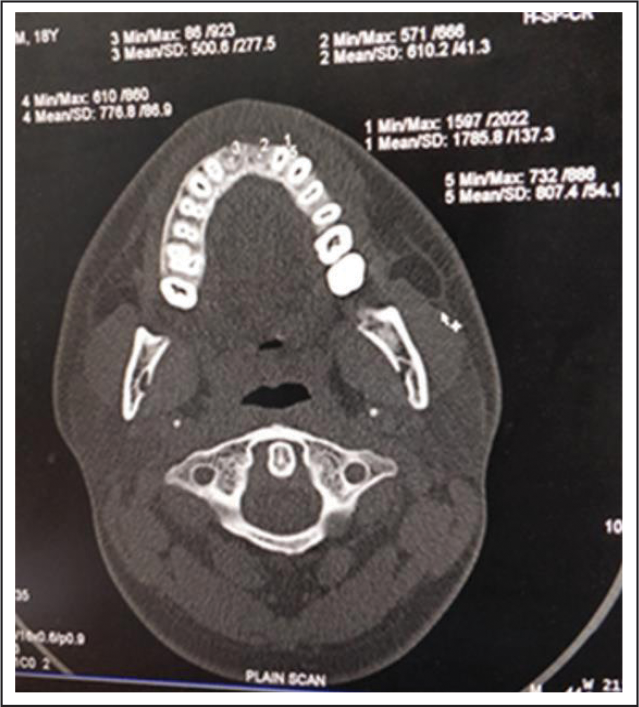
CT Image Demonstrating Bone Densities of the Grafted Sites (Bone Densities Shown as Numerical Values on the Film).
None of the patients reported any sign of infection or graft rejection. Satisfactory healing was observed in all patients at end of 3 months.
Discussion
Different types of grafting techniques are under practice by the clinicians for more than 10 decades. 13 Constant research and development as well as academic progressions have led to the formulations of diversity of biomaterials which have been commercialized. Autogenous grafts are considered as gold standard in different hard tissue deficiencies because of their properties of osteogenesis, osteoinduction, and osteoconduction, with swift healing. 14 Limited harvesting volume, resorption, and production of secondary defect in donor region are some of the drawbacks for autogenous graft.15, 16 To overcome these limitations, allogeneic bone, xenogeneic bone, and synthetic bone are used in clinical scenario with constant efforts to harvest an perfect grafting material.17, 18
The traditional classification of bone graft materials includes autogenous bone, allografts, xenografts, and alloplasts. 19 Allografts consist primarily of freeze-dried human bone with or without demineralization (demineralized freeze-dried bone allograft; freeze-dried bone allograft). Xenografts are formed from bovine bone-derived materials which are divided into 2 types in accordance to whether they are exposed to a chemical or thermal deproteinization process (chemically deproteinized bovine bone; thermally deproteinized bovine bone). Alloplasts utilize either HA or other calcium phosphate compounds such as betatricalcium phosphate. However, only HA and betatricalcium phosphate have been satisfactorily clinically assessed as bone substitutes till date. 20
The major concern linked with the use of allogeneic and xenogeneic bone is cost and possible spread of infections which marks practitioners and patients to choose in contrast to these types of grafting materials.7–9 Despite this, synthetic bone is comparatively cheap with no risk of spread of infection, but osteogenesis and osteoinduction properties are lacking, so its usefulness is imperfect for the foundation of viable bone.
HA is one of the families of orthophosphate molecules and considered as the most biologically compatible substances used as bone graft substitute material. HA is the dominant inorganic component of the hard tissues of the human body. HA has been used in particulate or granule forms and porous blocks also. HA shares similarities with the mineral phase of the bone.
Numerous literature ranging from case reports to randomized controlled trials have discovered the usage of extracted teeth as grafting material.21–24 Kim et al 24 concluded that a new grafting material assimilated autogenous teeth, experienced gradual resorption, and was substituted by fresh bone of good quality through osteoinduction and osteoconduction. Gual-Vaques et al 25 evaluated the use of autogenous tooth bone graft material in alveolar ridge augmentation procedures. The graft is osteoinductive since it contains various growth factors including bone morphogenetic proteins, transforming growth factor-beta, insulin-like growth factor-1 and -2. Unlike other autogenous grafts, when the autogenous dentin graft is used for extraction sockets, no resorption becomes evident and also no secondary defect results and adequate volume is obtained.15, 16 Moreover, the risk of graft rejection is also minimal because the tooth matrix is autologous and reduces the cost to the patient. Ascertaining the abovementioned qualities, we found that sockets preserved with dentin showed higher bone density compared to those preserved using HA crystals.
The primary implant stability is well-defined as “biometric stability immediately after implant insertion.” 26 It is also a mechanical phenomenon which is exclusively related to quality and quantity of bone, geometry of implant including length, diameter, type, and to the placement method used. Primary implant stability is dignified as the most significant fundamentals for preservation of osseointegration. 27
Earlier, primary stability was determined by the clinician on his perception after implant insertion. However, main drawback of this technique was that it was extremely subjective and examiner-reliant. Meredith et al 28 proposed use of RFA and damping capacity assessment as trustworthy, reproducible, and very easy to operate devices. 28 One of the latest versions of RFA available includes a wireless device in which a metal rod is linked to the implant by a screw connection. Advantages of RFA include that it is a noninvasive technique which is used to establish a clinically related information during any stage of implant placement that automatically converts kHz to implant stability quotient (ISQ) values. 29
The findings of our study validated the osteoinductive potential of allogenic, demineralized, and lyophilized dentin. We came to conclusion that autologous dentin graft leads to an increase in bone mineral density as compared to HA crystals when utilized for socket preservation. Moreover, the resulting higher bone density also leads to higher primary implant stability. A demerit of the study is that the grafts were placed in extraction sockets of nonidentical teeth and in individuals of varying age which might have confounding effect based on pre-existing cortical bone density. Furthermore, the sample size was too small for statistical analysis. This could be explained on the observation that enrolling patients fitting the inclusion criteria was a difficult task as one of the criteria was the requirement of simultaneous extraction of 2 teeth in the same patient. The authors are of the opinion that further continuation of research based on finding of this pilot study with removal of confounders through even stricter inclusion criteria will provide more reliable data.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Necessary ethical clearances and informed consent was received and obtained respectively before initiating the study from all participants