
Abstract
The zygomatic buttress is the functionally and structurally important vertical buttress. The strength and support of the midface are mainly by the buttresses. A study was done to evaluate and compare vertical with horizontal vestibular incision to reduce and plate fractures involving zygomatic buttress. Intraoperative evaluation and comparison of exposure time and time taken for surgery, herniation of the buccal fat pad and exposure of the fracture site were performed, followed by postoperative evaluation and comparison of pain, wound, sialocele formation and infection done on 7th, 14th and 21st days. Horizontal incision gives limited accessibility and visualization, with buccal fat interference and difficulty in suturing the distal part of the incision. It also, in some instances, caused injury to Stenson’s duct. An obliquely placed vertical incision eliminates the need to reflect all muscle attachments and provides a good amount of soft tissue for closure. Vertical incision shows no instances of injury to the duct of the parotid gland.
Keywords
Introduction
The face can be divided into upper, middle and lower thirds. The middle third is important for aesthetic and functional purposes and comprises many bones. 1 Out of which the zygomatic bone is the most important pillar structure of the midface region. The complex nature of the midface region is such that it will withstand all the forces of mastication and protect vital structures. 1 Zygomatic buttress is functionally and structurally important, giving prominence to cheeks as well as being important for eye globe function. Zygomatic buttress is the most commonly fractured bone in all types of facial fractures. The strength and support of the midface are mainly by the buttresses, which are also known as pillars of the face. The zygomatic-maxillary buttress starts above the first molar and travels along the lateral maxilla through the zygomatic bone, along the lateral orbital rim through the frontal processes of the zygoma, and finally through the zygomatic process of the frontal bone. 2 Vertical pillars primarily transmit all masticatory forces towards the base of the skull. 1
On application of external forces, the buttress pillar guards the facial skeleton from any disruption up to a threshold level beyond which fractures occur. 2 The conceptual philosophy of maxillary reconstruction is based on the distribution and transmission of forces throughout the facial skeleton. 2
The major causative factor for the fracture of the main buttress is road traffic accidents. While other causes involve falls and assault. Sports injury is the least responsible factor causing midface and zygoma fractures. The majority of patients with buttress fractures are male within the age group of 20-40 years, with aetiology being road traffic accidents (RTA) and in most of the patients, the right-side fracture is more common than the left side of the face. 2
Proper history, clinical inspection and palpation will help in the diagnosis. Disruption of the Dolan’s lines, orbital line, zygomatic line, maxillary line and loss of elephant trunk appearance are the radiographic findings seen on Waters view and jug handle view. Other important lines to be taken into consideration are McGregor-Campbell’s lines.2, 3 Few zygomatico-maxillary complex (ZMC) fractures are non-displaced, for which a conservative approach is undertaken. According to various analyses, 8%-51% of ZMC fractures do not require any surgical intervention. For open reduction with or without fixation of midface fracture, there are many well-documented surgical approaches and incisions, both intraoral and extraoral. 4
The intraoral vestibular approach for the maxilla is most commonly used when one has to perform any of the procedures on the central and peripheral midface region. 3 It gives appropriate visibility and accessibility to the complete facial region of the midface, including the arch up to the inferior orbital rim and frontal process of the maxilla. 3 This incision may cause injury to Stensen’s duct. 5 The posterior part of this incision is not so easy to suture, so wound dehiscence can occur, leading to plate exposure and infection.
A new intraoral incision has been described by Benjamin Bush to approach the zygomatic buttress region.5, 6 Obliquely placed vertical incision technique reduces complications of the conventional vestibular approach by avoiding buccal fat herniation and injury to Stenson’s duct.
Methodology
The investigators implemented a comparative study that was approved by the ethical committee of the university (SVIEC/ON/Dent/BNPG16/D17054). Patients included were those who reported at our hospital and Department of Oral and Maxillofacial Surgery and also patients referred from other departments from January 2020 to January 2022 with midface fracture involving zygomatic buttress. Subjects eligible for the study had isolated non-pathologic fractures involving the zygomatic buttress. Male or female with the age >18 and <65 were included. Vertical vestibular incision was evaluated in the parameters of accessibility, visibility and exposure of the fractured buttress and complication and then compared with findings of horizontal incision. The clinical study evaluated and compared exposure to the fracture site, exposure time, buccal fat herniation and complications of healing as wound dehiscence, postoperative pain, infection and sialocele formation on the 7th,14th and 21st day.
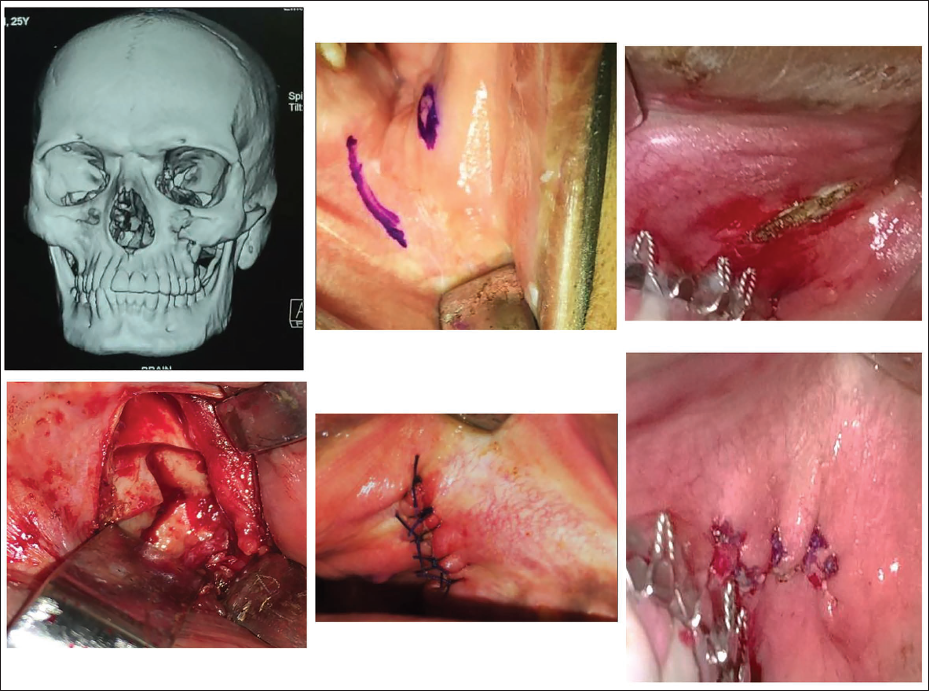
All patients were operated under general anaesthesia through nasal intubation by the same surgeon following all standard aseptic protocols. An obliquely placed vertical curvilinear was placed 8-10 mm anterior to Stenson’s duct. A horizontal anterior extension may be placed 3-5 mm above the mucogingival line if needed. This incision starts superiorly from the body of the zygoma up to the alveolar bone of the maxilla. Subperiosteal dissection is performed to allow adequate access to the fracture site. This incision was performed on Group A patients (Figure 1).
Group A: Intraoral Vertical Incision.
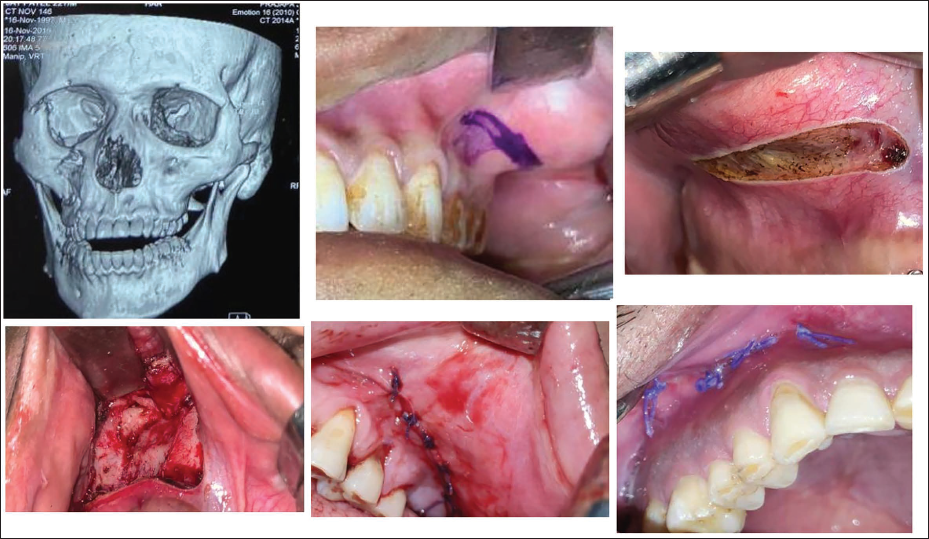
On palpation of malar eminence and the buttress, a horizontal incision was marked 3 mm above the mucogingival line, which extended posteriorly behind the buttress and anteriorly towards the nasal rim. Full-thickness, mucoperiosteal incision was made starting on the body of the zygoma and extending to the maxillary alveolus and buttress region. Subperiosteal dissection is performed in all directions to allow adequate access to the fracture site. This incision was performed in Group B patients (Figure 2).
Group B: Intraoral Horizontal Incision.
No standardized protocol for closure of incision was fixed or pre-decided. After performing fixation, closure of both vertical and horizontal incision was performed using resorbable round body 3-0 Vicryl suture by interrupted technique in almost all the cases. Material and technique for closure were not considered as parameters for evaluating the efficiency of incision as it does not affect the study.
Statistical Methodology
The data analysis was done with IBM SPSS 20 for Windows statistical software. Statistical analysis was done using the chi-square test and paired sample t-test for quantitative data. For all statistical analyses, probability levels of P < .05 will be considered statistically significant.
Result
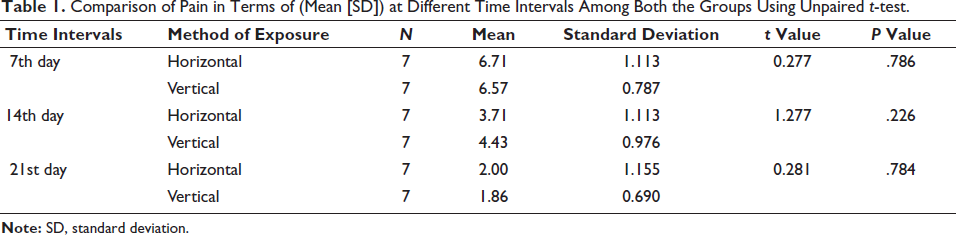
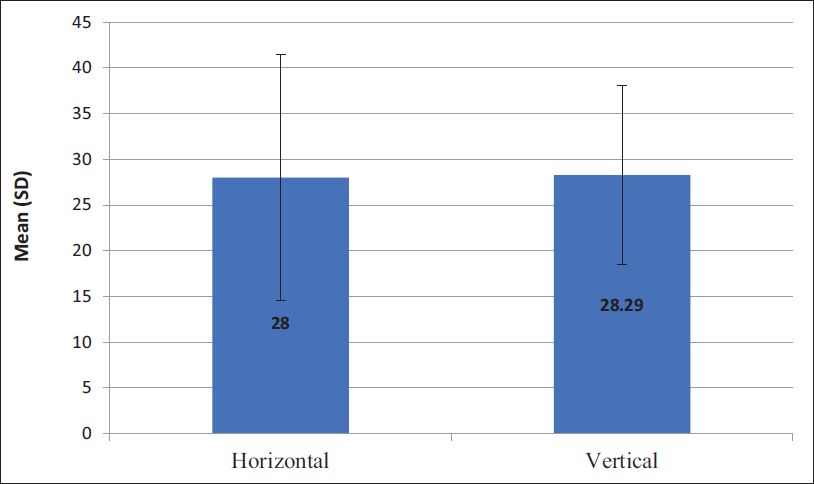
A total of 50 patients with midface fractures were treated during the study period, from which 14 patients fulfilling the inclusive criteria were included in the study, 7 patients in each group, Group A—intraoral vertical incision and Group B—intraoral horizontal incision, which were chosen randomly. Of 14 patients selected for our study, all were male with a mean age of 28 years (Figure 3). Evaluation and comparison for visualization of fractures, exposure time (Figure 4) and amount of exposure of fracture site, intraoperative buccal fat herniation, healing process and incidences of wound dehiscence, postoperative pain (Table 1), infection and sialocele formation were evaluated on days 7th,14th and 21st postoperatively.
Comparison of Pain in Terms of (Mean [SD]) at Different Time Intervals Among Both the Groups Using Unpaired t-test.
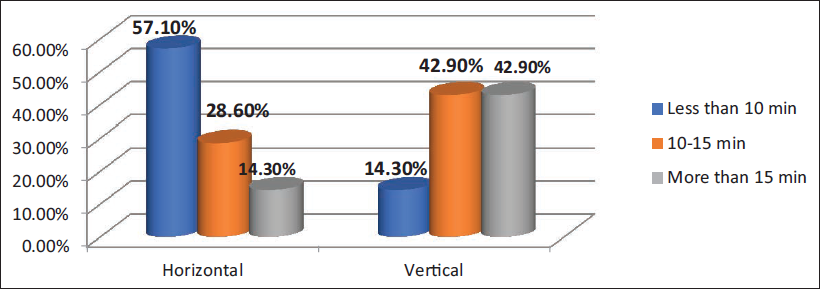
Comparison of Time Taken for Exposure of Fractured Site Among Both the Groups Using Chi-square Test.
Discussion
Jain et al. suggested that zygomatic fracture is the most common facial fracture and second in frequency after the nasal fracture.7 The incidence, ethnicity, aetiology, age group and sex predilection of zygomatic injuries vary depending on the socioeconomic, political and academic standing of the population. Many studies on zygomatic fracture show a predilection of males, with a quantitative relation of 4.1:1.2 roughly over females. 7 The left zygomatic fracture is mostly seen, mainly because of the greater number of right-handed people. 8 The data of our study showed that the mean age for zygomatic buttress fracture was 28 years for all 14 patients, including both groups A and B. Of 14 patients selected for our study, all were male. The zygomatic bone has a vital role in facial structure. Changes in the zygomatic bone position cause disturbance in function. So for aesthetic and functional purposes, zygomatic-complex trauma must be diagnosed properly and effectively treated. 9
Various approaches are effectively used for treating zygomatic-complex fractures. Pre-existing lacerations are mostly used for reduction and fixation so that it avoids extra scarring. In the cases where lacerations did not exist, properly placed incisions provide adequate exposure, with minimal morbidity and scarring. There are extraoral as well as intraoral approaches. Intraoral approaches are always better as they are scarless. 8 In our study, we have compared two different intraoral incisions. We did a prospective, comparative study of intraoral vertical incision and horizontal incision in patients with fractures involving the buttress region to find out the advantages and disadvantages of both intraoral approaches.
Ellis and Kittidumkerng 7 studied different surgical approaches; according to their study and research, they analysed and concluded that the transoral upper vestibular approach was used most frequently, either alone or in combination with different extraoral approaches. The maxillary vestibular approach is one of the most important and least complicated approaches for the open reduction of zygomatic fractures. It gives adequate visibility to the entire midfacial region with good accessibility up to the infraorbital rim. In other extraoral approaches like trans-conjunctival, an additional intraoral approach is needed for zygomatic buttress fixation.
Rehman et al. suggested the advantages and disadvantages of various surgical approaches by research on 81 patients with zygomatic fractures to study different patterns, causes and treatment options.9 The author also explained many benefits of transoral vestibular incision like better visibility and good exposure of fracture site.9
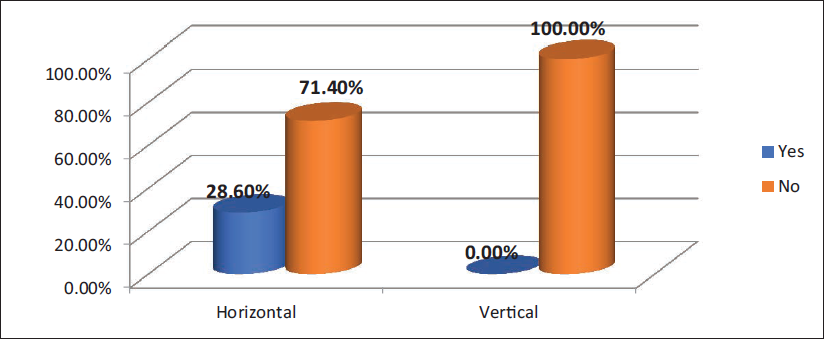
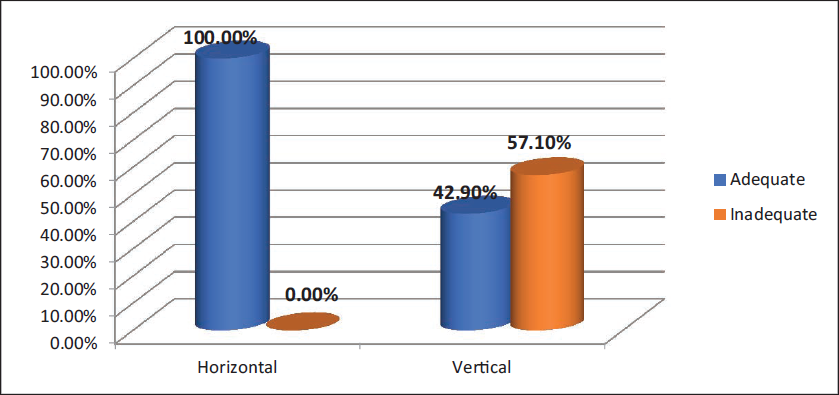
In our study, we placed a vertical incision in Group A and a horizontal vestibular incision in Group B patients. The horizontal incision provided good visibility and exposure to the zygomatic buttress fracture site. Complications with horizontal incision included buccal fat herniation, injury to Stenson’s duct and damage to the infraorbital nerve. Herniation of the buccal fat pad may disturb the visibility of the fracture site if a surgeon is unable to properly retract the buccal fat pad. In our study, buccal fat pad herniation was seen in two cases (28.60%) with horizontal incision. With vertical incision, there was not a single case with buccal fat pad herniation. We did not find any other postoperative complication in the patient with herniation of the buccal fat pad (Figure 5). Exposed buccal fat pad (BFP) increases suturing time. It also intervenes in the visibility and exposure of the fracture site. In our study, buccal fat herniation did not affect exposure and visibility of the fracture site because of better retraction. The result of our study shows that for Group B, visibility and exposure of the fracture site were adequate in all seven cases, which is 100%, whereas for Group A, in three patients, 42.90% had adequate visibility and 57.10%, that is for four patients, visibility was not adequate (Figure 6).
Comparison of Herniation of Buccal Fat Pad Among Both the Groups Using Chi-square Test.
Comparison of Visibility and Exposure of Fractured Site Among Both the Groups Using Chi-square Test.
The vertical curvilinear intraoral incision overcomes the complication of buccal fat pad herniation and injury to the duct causing sialocele and gives good access and visibility to the zygomatic buttress and infraorbital rim. This incision is more useful in isolated buttress and unilateral ZMC fractures than in the fractures involving bilateral zygoma, Le Fort and comminuted fractures. Vertical incision provides less visibility to the pyriform region than the horizontal incision. 10
Superior reflection of the flap for better accessibility to the fracture region using maxillary vestibular incision can damage the Stenson’s duct due to the pressure of the retractors. 11 Damage to the Stenson’s duct causes fistulous tract formation or swelling over the parotid region. In our study, we did not find sialocele in any case in either Group A or Group B on the postoperative 7th, 14th and 21st days.
Complications such as postoperative wound dehiscence and infection depend on many factors like oral hygiene and suturing technique. In our study, we observed some patients with horizontal incisions had infections and wounds gaping in the postoperative period as distal extension of incision is difficult to suture and difficult to maintain hygiene. Another observation noted in all cases with vertical incisions was the absence of wound gapping.
The oblique orientation of the vertical incision eliminates the need for the transection of muscle fibres, thereby making this design less invasive than horizontal vestibular incision.10, 11 The absence of wound gapping could be attributed to the free mobility of alveolar mucosa aiding in tension-free primary closure. Infection was present in 14.30% of cases on the seventh postoperative day in Group B and there was not a single case with infection in Group A. 12 The disadvantage of the vertical approach is the closure of the incision that directly occurs on the plate. To avoid complications, one can place the incision anteriorly and the plate posteriorly.
The total time taken was counted from the time of the start of the incision till the complete exposure of the fractured segments. In our study for the horizontal incision Group B, the time taken for exposure of the fractured site was less than 10 min for four patients (57.10%), whereas in three patients, that is, 28.60%, it was 10-15 min. There was a single case where the time taken was more than 15 min with 14.30%.
In the vertical incision group (A), the time taken for exposure of the fractured site was less than 10 min for one patient (14.30%), whereas in three patients, it was 10-15 min (42.90%). There were three cases where the time taken was more than 15 min (42.90%; Table 2).
Comparison of Time Taken for Exposure of Fractured Site.
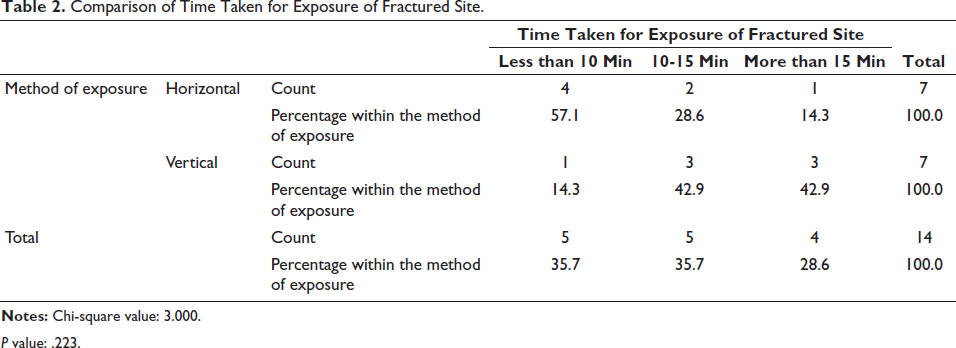
P value: .223.
Conclusion
After evaluation and comparison of both the intraoral incisions for the management of zygomatic buttress fracture, we concluded that intraoral vertical incision can be efficiently used for the reduction and fixation of zygomaticomaxillary complex fractures. This incision does provide sufficient exposure to the fracture site, and its orientation eliminates the need for muscle transection allowing abundant soft tissue for easy tension-free closure reducing postoperative complications. It also eliminates the risk of injury to the duct of the parotid gland. Further study should be carried out before including this incision routinely.
Footnotes
Acknowledgement
The authors would like to thank Gulam Naviwala for his comments, insightful suggestions and careful reading of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest concerning the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent and Ethical Approval
Necessary ethical clearances and informed consent were received and obtained respectively before initiating the study from all participants.