
Abstract
Background and Introduction:
Maxillofacial fractures are less common in children. Mandibular fractures are less in children because of the protective anatomy in them. Management of the pediatric fracture depends on the type and severity of the fracture displacement. It can vary from conservative management with acrylic splint and arch bar fixation to surgical exposure of the fracture site with internal fixation. Special consideration is needed in children for the interferences of growth and developing tooth buds while going for the surgical management. The hardware for internal fixation can be made up of either titanium or bioresorbable material.
Case Presentation:
Here is the presentation of a case of a 7-year-old male patient who had a history of trauma because of falling from a tractor while playing, 2 days back from reporting. He had multiple mandibular fractures with extensive soft tissue laceration. Following the emergency tracheostomy, he was managed with open reduction and internal fixation of the compound mandibular fracture.
Conclusion:
Displaced mandibular fractures require open reduction and internal fixation of the fractured fragments with either titanium or biodegradable hardware. Open reduction also shortens the period of intermaxillary fixation and hence reduces the possibility of the development of temporomandibular joint (TMJ) ankylosis.
Keywords
Introduction
The incidence of mandibular fracture is less in children as compared to adults because of protection through anatomical features and lesser exposure to trauma because of road traffic accidents. The incidence of mandibular fracture is high among the maxillofacial injury in children. The notorious nature of children make them prone to many injuries. The goal of treatment of mandibular fractures in children is to restore a stable preinjury bony architecture through a noninvasive procedure with minimal esthetic and functional deficit. The type of reduction in pediatric fracture depends on the displacement of the fractured fragments. Closed reduction is preferred over open in most of the fractures as the latter may affect the growth of the jaw and the developing dentition.
Case Report
A 7-year-old male patient reported to the Oral and Maxillofacial Trauma Unit of King George’s Medical University, Lucknow, with the chief complaint of pain and swelling on the lower face since 2 days of reporting. The patient had a history of trauma because of fall from a tractor, 2 days back from reporting while playing, with a negative history for loss of consciousness, seizures, and vomiting.
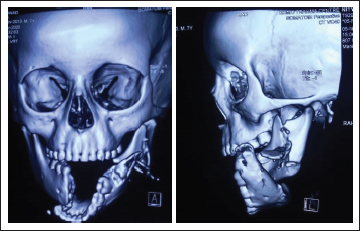
The patient was unable to speak and had difficulty in breathing. On extra oral examination, patient had lacerated wounds on the lower third of the face. One laceration extended from right angle of the mouth to the lower border of the mandible. Other laceration was on the left cheek including skin, subcutaneous tissue, buccinators, and intraoral mucosa. This laceration extended from the left corner of the mouth to the left preauricular region (Figure 1). On intraoral examination, the patient had step deformity between right mandibular deciduous canine and first premolar, and distal to left permanent mandibular first molar with deranged occlusion. Examination through computed tomography revealed a fracture of the right parasymphysis and comminuted a fracture of the left angle-ramus complex of the mandible (Figure 2).
Lacerated Wound of the Lower Face with the Compound Fracture of Mandible.

Preoperative CT Images Showing Mandibular Fractures.
Emergency Ear Nose and Throat (ENT), Department of Otorhinolaryngology, team was called for emergency tracheostomy to maintain the airway, which was done after sedating the patient under observation by the help of the anesthetic team. This was followed by fixation of upper and lower arch bars and intermaxillary fixation (IMF) through elastics to stabilize the mandible. The laceration was debrided and sutured. The patient was kept on intravenous antibiotics and analgesic after consultation from the Department of Pediatrics for proper dosage.
Patient was then operated under General Anaesthesia (GA) the following day. The fracture sites were exposed through the laceration, and open reduction and internal fixation (ORIF) was done with 1.5 mm Ti system. One 5-hole plate with 4 bicortical screws was fixed on the inferior border of the mandible on the right parasymphysis region (Figure 3). One 6-hole straight plate with 3 screws and one 6-hole L plate with 4 screws were fixed on left angle-ramus complex after simplification of the fractured fragments (Figure 3). This was followed by copious irrigation of the operated site. Ceftriaxone powder was used as a local antibiotic and the site was closed in multiple layers using vicryl and prolene suture materials.
Intraoperative Images Showing Fixation of the Fractured Fragments.

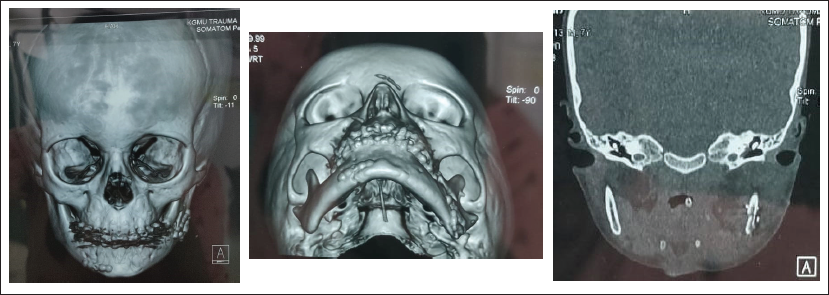
After 7 days, the soft tissue healing was satisfactory and suture removal was done. Postoperative CT scan showed accurate reduction of the fractured fragments (Figure 4). The tracheostomy tube was also removed through sequential closure of the tube after 15 days. The patient was kept on regular follow-up and the arch bars were removed after 1 month postoperatively after confirming the occlusal status. The patient is now on regular follow-up and plate removal will be planned after 3 months postoperatively.
Postoperative CT Images.
Discussion
Pediatric facial fractures constitute 5% of all the facial fractures. 1 Mandibular fractures are the most common facial skeletal injury in pediatric trauma patients.2-4 In Posnick and colleagues’ study 39% of all fractures were of the mandible. Mandibular fracture sites included the condyle (59 of 107, 55%), parasymphysis (29 of 107, 27%), body (10 of 107, 9%), and angle (9 of 107, 8%). 5
General considerations for the young injured patient include airway maintenance, fluid and electrolyte balance, and rational nutritional intake throughout treatment.6, 7 As in adults, the primary evaluation of a pediatric trauma patient should pursue “ABCs” of advanced trauma life support. In the presented case, because of the severely displaced fracture of mandible the patient had difficulty in breathing and hence an emergency tracheostomy was performed.
The management of mandibular fractures in children differs from that of adult because of the possible disturbances in the growth of the mandible. The presence of developing tooth buds is also a concern while treating a patient with mandibular fracture with open reduction. The short length and the shape of the deciduous teeth make arch bar fixation and, hence, closed reduction difficult. The management option depends on the severity of the displacement of the fractured fragments. Undisplaced and mildly displaced fractures of mandible can be managed conservatively with acrylic splint and circum-mandibular wiring or closed reduction with arch bars and IMF.
IMF in children becomes difficult because of mixed dentition, less availability of teeth, root resorption of deciduous teeth, and unfavorable form of crown of deciduous teeth. Posnick stated that approximately 42% of mandibular fractures in his series were managed by closed reduction, mainly with the help of maxillomandibular fixation.7, 8
Currently, ORIF have become the standard care for the treatment of displaced pediatric mandible fractures6, 9-11 with miniplates, microplates, or biodegradable plates. ORIF has many advantages like primary healing, 3-dimensional stability, and shortened treatment time. But it also has a risk of possible damage to the developing tooth buds, disturbances in growth and plate migration. 12
There are some disadvantages related to the use of titanium hardware for ORIF. These include imaging interference, temperature sensitivity, corrosion, hypersensitivity reactions, stress shielding, hardware translocation through the growing skeleton, palpability, chronic pain, and infection.13, 14 This leads to the use of biodegradable plates in pediatric fractures. A systematic review by Pontell et al 15 concluded that neither titanium nor resorbable hardware has a superior complication profile when treating pediatric mandible fractures that require ORIF. There is no benefit of using one material over the other with regard to specific fracture patterns and neither material obviates the need for maxillomandibular fixation. Consideration of the use of resorbable hardware should be given when available, given the noninferior complication profile and the fact that titanium hardware often requires extraction with additional anesthetic.
Conclusion
Undisplaced pediatric mandibular fractures should be treated with conservative approaches like acrylic splint or closed reduction with IMF. But displaced mandibular fractures require ORIF of the fractured fragments with either titanium or biodegradable hardware. Open reduction also shortens the period of IMF and hence reduces the possibility of development of TMJ ankylosis. In the presented case, authors successfully treated a case of compound mandibular fracture with ORIF resulting in a satisfactory occlusion and adequate mouth opening.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Necessary ethical clearances and informed consent was received and obtained respectively before initiating the study from all participants.