
Abstract
Fracture of the condylar process is the most common site within the fractures of the mandible and causes problems such as occlusal dysfunction, temporomandibular joint dysfunction, and facial deformities. Therefore, proper treatment of this entity is paramount in preventing such problems. Essentially, there are three treatment approaches, namely, observational, close reduction and open reduction, and internal fixation. 1 The debate between open and close reduction has been going on ever since with the proof that open reduction aims at restoring the facial asymmetry of the patient faster: although it has its own demerits like limited access even through surgical exposure and difficulty in reduction. Medially displaced fractures that pose such problems are treated with extracorporeal fixation of the fractured segment. 2 We hereby present such a case with the detailed technique and the literature around it.
Case Report
A 32-year-old male reported to the emergency of our institute after a road traffic accident and was admitted under the Department of Neurology for conservative management for a week. After getting discharged, he was referred to the Department of Maxillofacial Surgery for his complaint about facial asymmetry. Upon admission, the patient was well-oriented to the time, place, and person with all his vitals under normal conditions.
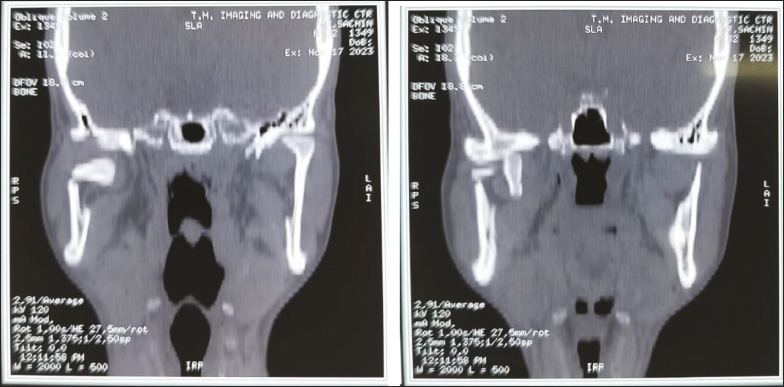
Upon examination, his malar prominences were depressed and tender on percussion as well as restricted mouth opening with a deranged occlusion with left posterior openbite was observed. NCCT Face was advised for the patient which revealed a right subcondylar fracture (Figure 1) with medial displacement of the fractured segment (Figures 2 and 3) along with the right zygomatico-maxillary buttress fracture and left fronto-zygomatic suture fracture.
Preoperative Radiograph.
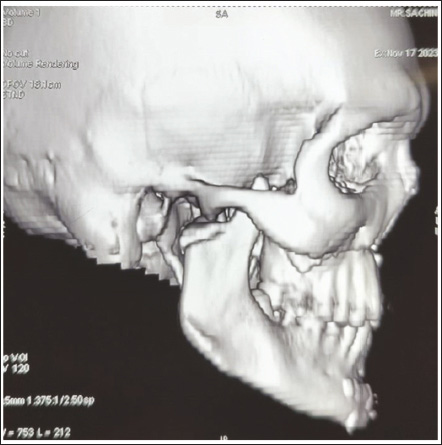
Medial Displacement of the Condyle.
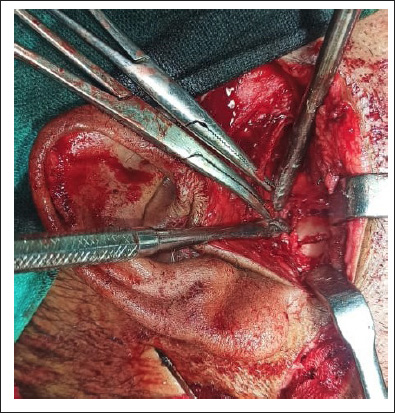
According to the criteria given by Zide and Kent 3 the case was taken up for general anesthesia. No clearance from the local ethics committee was required as the treatment plan is a routine procedure (ORIF). Nasotracheal intubation and inter-maxillary fixation were done. The fracture was approached by Thoma’s incision (Figure 4). After retraction of the skin edges, the scant platysma muscle overlying the superficial musculoaponeurotic system (SMAS) was visible. A scalpel was used to incise through the fusion of platysma muscle, SMAS, and parotid capsule in the vertical plane. The gland was then clearly visible. Blunt dissection was done within the gland in an anteromedial direction toward the posterior border of the mandible, and the facial nerve branches were retracted out of the operative field. After retraction of the dissected tissues anteriorly, the posterior border of the mandible was seen and the distal part of the fracture, that is, fractured condyle was seen (Figure 4). However, adequate reduction of the fractured segment into the previous anatomical position was found to be unsuccessful because of the severe medial displacement as well as the limited access to the site. Additional medial displacement would have resulted in an unwanted and difficult-to-control hemorrhage from the internal maxillary artery.
Exposure of the Fractured Segment.
With all these factors in mind, the decision to fixation of the condyle was taken to be done extracorporeally which proceeded with the careful dissection of the muscular and soft tissue attachments from the condyle and taking it out (Figure 5) followed by the fixation by a three-dimensional delta plate and was then secured completely with the native mandible (Figure 6) which resulted in the anatomically acceptable position of the condyle with the glenoid fossa.
Condyle Taken Out Extracorporeally.

Explanted Segment With the Distal Segment Fixed With a 3D Delta Plate.

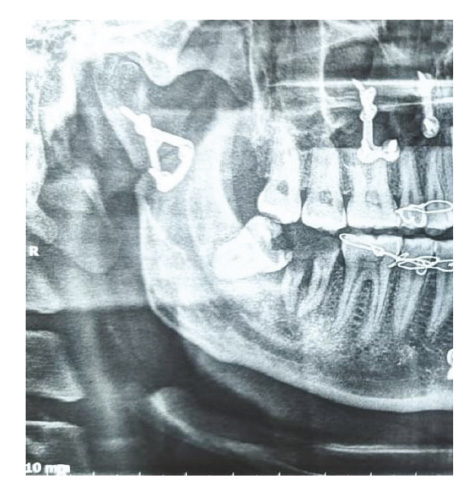
Other fractures were subsequently plated. The surgical site was then closed in layers with water-tight closure, and the patient was put on anticholinergics. Postoperative OPG revealed fixation of the condyle (Figure 7). Healing was uneventful, and the patient was advised physiotherapy and regular follow-ups.
Postoperative OPG.
Discussion
The use of extracorporeal fixation for condylar fracture has been infrequently reported in the English literature. Boyne 4 described the technique of extracorporeal fixation in 35 cases of severely displaced condyle fracture resulting in no resorption. Mikkonen et al. 5 advocated extracorporeal fixation combined with ramus osteotomy to improve access for management of anteromedially displaced condylar head fracture and proposed fully rehabilitated joint function. In 2009, Gupta and Sahoo 6 conducted a study on extracorporeal fixation of 18 condylar fractures and experienced satisfactory occlusal stability and functional recovery. Upon every observed positive aspect from many authors, it should also be taken into consideration that extracorporeal fixation can also result in resorption of the condyle as it will turn it into a free graft by reducing its blood supply 7 while severing the fibers of the lateral pterygoid and periosteal stripping and long-term follow-ups are required for these patients in order to make this technique more reliable and considerable in the future.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author received no financial support for the research, authorship and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Necessary ethical clearances and informed consent was received and obtained respectively before initiating the study from all participants.