
Abstract
Objective
This study aimed to assess the practicality and optimal approach for inserting an anterior occipital condyle screw, as well as to measure the screw placement characteristics.
Methods
A total of 80 normal head and cervical spine computed tomography scans (40 males/40 females) were used to construct three-dimensional models. The average age of the participants was 45.18 ± 8.86 years (ranging from 25 to 65 years). Three potential entry points for the anterior occipital condyle screw were identified. A simulated screw with a radius of 1.75 mm was created to replicate the screw trajectory and adjusted to establish the maximum and minimum cranial limits for each entry point. The feasibility of screw fixation was assessed, identifying the optimal entry point and analyzing relevant screw placement measurements.
Results
The success rates for screw placement were 95.6%, 94.4%, and 88.1% for the middle, lateral, and medial entry points, respectively. The success rate for the medial entry point was notably lower than that for the middle and lateral points. No statistically significant differences were found in the measured parameters between the left and right sides. The medial entry point exhibited the highest abduction angulation (35.72° ± 2.01°) for screw placement, followed by the middle (25.96° ± 1.86°) and lateral (15.14° ± 1.82°) points. The middle and lateral entry points displayed a considerably wider safe range of cranial angulation and screw placement length than the medial entry point. All three entry points achieved success rates exceeding 90% when the cranial angulation ranged from 2° to 6°.
Conclusion
The anterior occipital condyle screw presents a workable choice for anterior craniovertebral fixation. The middle entry point is identified as the optimal approach for placing 3.5-mm diameter screws.
Introduction
The craniovertebral junction (CVJ) links the base of the skull with the spine, enabling intricate mobility owing to its complex anatomical and functional characteristics. 1 Various factors such as trauma, infection, inflammation, deformities, and tumors can lead to CVJ disability, resulting in myelopathy, cranial nerve dysfunction, and even fatality.2,3 Surgical interventions encompass decompression, resection, and providing sturdy internal fixation of the CVJ. 4
Posterior occipitocervical fusion surgery serves as a vital technique to address occipitocervical instability. 5 However, scenarios in which patients present substantial bone defects at the occipitocervical junction due to tumors or infections, coupled with severe atlantoaxial dislocation or failure of posterior internal fixation, demand combining anterior surgical methods to restore craniovertebral junction stability.6,7 Employing a titanium mesh cage and plate fixation system for anterior surgery has proven effective, ensuring immediate immobility and satisfactory bone fusion. 8 The clivus serves as a feasible structure for upward fixation, with clival screws offering enhanced biomechanical stability.9,10 Nevertheless, the clival screw technique remains surgically challenging owing to the intricate anatomical structures around the clivus. 1
Occipital condyles (OCs) constitute a vital component of the CVJ, anchoring the cranium to the spinal axis and serving as an appealing anchor point for upward fixation. 11 The use posterior OC screw, initially described by Uribe et al. 12 presents an anatomically viable technique, delivering substantial pullout strength and comparable biomechanical stability.13,14 Positive surgical outcomes have been documented in both adults and children.15,16
Therefore, we proposed that anterior condyle screws could serve as an alternative to clival screws for cephalad fixation in anterior occipitocervical fusion. This study investigated the feasibility of anterior OC screw fixation at the craniovertebral junction, pinpointing the optimal entry point and trajectory for screw placement through digital three-dimensional (3D) reconstruction techniques.
Methods
We conducted a retrospective analysis of patients who had undergone computed tomography (CT) scans of the head and cervical spine at Affiliated Hospital of Jiaxing University between September 2020 and September 2022. Exclusion criteria included: (a) age of <20 years or >65 years; (b) presence of trauma, tumors, infections, or deformities; (c) postoperative CT scans; and (d) slice thickness >1.0 mm. A total of 80 adults (40 males and 40 females) with a mean age of 45.18 ± 8.86 years were included in this study. The study protocol was approved by the ethics institution of the Affiliated Hospital of Jiaxing University (approval number: LS2020-31) and written informed consent was obtained from all participants. The study was conducted in accordance with the Helsinki Declaration of 1975, as revised in 2013, and the reporting of this study conforms to Strengthening the Reporting of Observational Studies in Epidemiology (STOBE) guidelines. 17
CT images were acquired using a Philips Brilliance 64 CT scanner (Philips Medical Systems, Eindhoven, The Netherlands). The following scanning parameters were applied: scan voltage 120 kV, scan current 280 mA, matrix 512 × 512, and slice thickness 1 mm. All data were saved as DICOM files and imported into Mimics 19.0 (Materialise, Leuven, Belgium) to generate a 3D reconstruction model of the occiput and atlas.
With the assistance of the View module, the 3D centers of the OCs and three potential entry points were determined (Figure 1(a)). Lines were drawn to define the anterior and posterior edges of the atlanto-occipital joint based on the oblique sagittal plane of each entry point. Measurements included the distance from the anterior cranial edges of the OCs to the line (H1), the distance from the bottom of the hypoglossal canal to the line (H2), and the distance from the posterior cranial edges of the OCs to the line (H3) (Figure 1(b) and (c)). We established that the anterior OCs could not accommodate insertion if H1, H2, or H3 were less than 4 mm, as the screw diameter in this technique should always fall within the range of 3.5–4.0 mm. To simulate screw insertion, a straight cylinder with a radius of 1.75 mm was generated and used to replicate the trajectory of an anterior OC screw (Figure 2(a) and (b)). For each entry point, the optimal screw trajectory, which would allow the longest screw placement length, was devised using the 3D view function. Following the determination of the ideal screw trajectory, the screw abduction angle (SAA) was fixed. Simulation of anterior OC screw placement on each side was performed under conditions of maximum cranial limitation (screw infringing on the hypoglossal canal) and minimum cranial limitation (screw infringing on the posterior occipital-atlas joint) (Figure 2(c)).

The three potential entry points were chosen: the middle entry point was positioned at the midpoint between the medial and lateral borders of the occiput. The medial and lateral entry points were situated 3 mm medially and laterally, respectively, from the middle entry point (a). Three simulated optimal screw trajectories were established (b), and on an oblique sagittal plane traversing the optimal screw trajectory for each entry point, three distance parameters were measured (c). The green line represents the line connecting the anterior and posterior edges of the atlanto-occipital joint.

The simulated trajectories of anterior occipital condyle screws were visualized in a 3D perspective for the three entry points (a). The axial view of the occipital condyle depicted that each simulated screw was appropriately placed along the optimal trajectory (b). Simulated screws were inserted with both maximum cranial limitation and minimum cranial limitation, and the sagittal view illustrated the screw positions along with their spatial relationship with neighboring structures (c).
The following screw placement parameters were measured for each simulated screw (Figure 3(a) and (b)):

Measurement of screw placement length (SL) and screw abduction angle (SAA) (a). Measurement of cranial angle: the angle formed between the screw axis and the McRae line (b).
SAA: the angle formed between the screw axis and the median line of the occiput. Maximum cranial angle (Max-CA): the angle formed between the screw axis and the McRae line under maximum cranial limitation. Minimum cranial angle (Min-CA): the angle formed between the screw axis and the McRae line under minimum cranial limitation. Screw length 1 (SL1): the length of screw placement with maximum cranial limitation. Screw length 2 (SL2): the length of screw placement with minimum cranial limitation. Safe range of cranial angulation (SRCA): the difference between Max-CA and Min-CA.
Statistical analysis was conducted using Statistical Package for the Social Sciences SPSS version 22.0 (IBM, Armonk, New York, USA). Data were presented as means ± SDs. The T-test was employed for comparing sides, while one-way analysis of variance was used to compare parameters at each entry point. The χ2 test was used to compare the feasibility of different entry points. Values of P < 0.05 were considered to indicate statistically significant results.
Results
We reconstructed 64 3D models of the occiput and atlas, analyzing a total of 480 OC entry points, of which 445 entry points were suitable for accommodating the placement of a 3.5-mm diameter anterior OC screw. The lateral entry point had a significantly smaller H1 value (8.18 ± 1.37 mm) than the medial and middle entry points. No notable difference was observed in H2 values between the different entry points. In terms of H3 values, the middle and lateral entry points were significantly larger than the medial entry point (P < 0.05), whereas there was no difference between the middle and lateral entry points (P > 0.05) (Table 1). However, the H3 value of the medial entry point was notably smaller than those of the middle and lateral entry points (Table 1). The middle entry point exhibited the highest success rate (95.6%, 153/160) for screw placement, followed closely by the lateral entry point with 94.4% success (151/160); the success rate of the medial entry point was 88.1% (141/160), considerably lower than the middle and lateral entry points (P < 0.05). No significant differences were found between the left and right sides for these screw placement parameters (P > 0.05) (Table 2). The screw placement parameters for all three entry points are detailed in Table 3. The SAA was the largest (35.72° ± 2.01°) for the medial entry point, followed by the middle (25.96° ± 1.86°) and the lateral (15.14° ± 1.82°) entry points. The difference in abduction angles between the three entry points was statistically significant (P < 0.05). The SRCA was 10.45° ± 2.08° for the middle entry point and 10.24° ± 2.01° for the lateral entry point, both significantly larger than that of the medial entry point (9.02° ± 1.64°; P < 0.05). The screw length, whether considering Max-CA or Min-CA, was notably shorter in the lateral entry point than in the middle and medial entry points (P < 0.05).
Measurement of H1, H2, and H3 (mean ± SD).

H1: distance from the anterior cranial edges of the occipital condyles to the line; H2: distance from the bottom of the hypoglossal canal to the line; H3: distance from the posterior cranial edges of the occipital condyles to the line.
Middle entry point (B) versus lateral entry point (C), statistical significance.
Middle entry point (B) versus medial entry point (A), statistical significance.
Lateral entry point (C) versus medial entry point (A), statistical significance.
Screw placement parameters comparison between sides (mean ± SD).
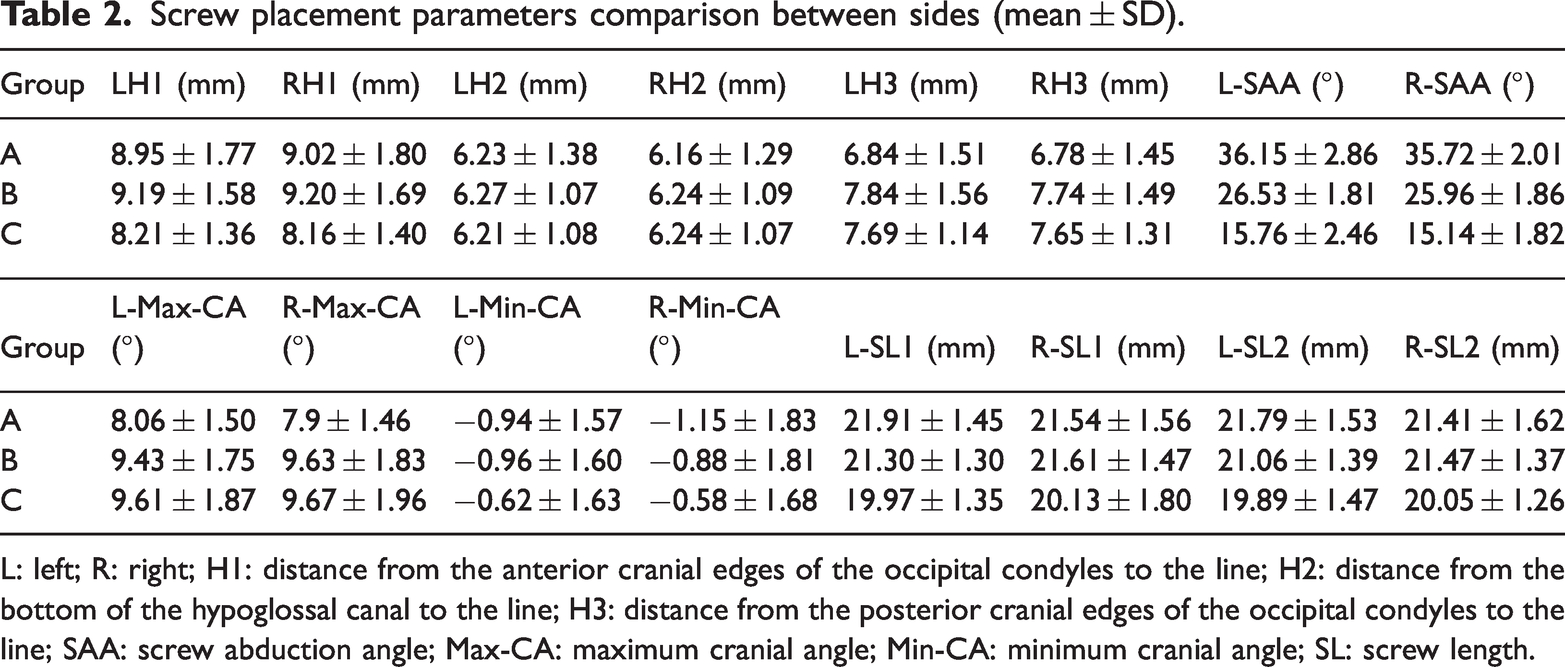
L: left; R: right; H1: distance from the anterior cranial edges of the occipital condyles to the line; H2: distance from the bottom of the hypoglossal canal to the line; H3: distance from the posterior cranial edges of the occipital condyles to the line; SAA: screw abduction angle; Max-CA: maximum cranial angle; Min-CA: minimum cranial angle; SL: screw length.
Screw placement parameters of each entry point (mean ± SD).

SAA: screw abduction angle; Max-CA: maximum cranial angle; Min-CA: minimum cranial angle; SRCA: safe range of cranial angulation; SL: screw length.
Middle entry point (B) versus medial entry point (A), statistical significance.
Lateral entry point (C) versus medial entry point (A), statistical significance.
Middle entry point (B) versus lateral entry point (C), statistical significance.
For each entry point, the success rate of screw placement was compared across various cranial angles, and the cranial angle range resulting in a success rate exceeding 60% was recorded (Table 4). The middle and lateral entry points exhibited screw placement success rates greater than 60% within a cranial angle range of 0° to 9°, whereas the medial entry point achieved this within an angle range of 0° to 7°. All entry points attained a success rate exceeding 90% with cranial angles ranging from 2° to 6°. The middle and lateral entry points achieved the highest success rates of 100% and 99.3%, respectively, at a cranial angle of 4°. Specifically for the middle entry point, cranial angles of 3° or 4° yielded optimal results, with a 100% success rate for screw placement.
The rate of successful screw placement larger than 60% for each degree of cranial angulation.

Discussion
The OCs are situated anterolaterally on each side of the foramen magnum within the occiput. They form an articulation with the upper facet of the atlas, creating the atlanto-occipital joint.18,19 Anterior OC screws were first described as a feasible, novel technique for anterior craniovertebral junction reconstruction by Xu et al. 20 in 2021, who successfully demonstrated their use in cadaver specimens. However, the optimal entry point for the anterior OC screw and its precise placement parameters remains unclear.
Anterior OC screw placement is influenced primarily by the hypoglossal canal and the atlanto-occipital joint. In this study, the middle entry point displayed the highest success rate at 95.6%, followed by 94.4% for the lateral entry point and a lower rate of 88.1% for the medial entry point. This discrepancy can be attributed to the hypoglossal canal's anterior and superior course from the junction of the middle and posterior thirds of the medial OC border, while the morphology of the atlanto-occipital articular surface inclines inferiorly medially and superiorly laterally. 21 Consequently, the available space for screw placement at the medial entry point is more constrained compared with that at the middle and lateral entry points.
Effective screw placement length is crucial for maintaining consistent biomechanical stability and achieving high pullout strength. The abduction angle serves as a significant parameter in determining the optimal screw length for insertion. In our study, the average abduction angle and screw length for the three entry points decreased progressively with outward movement. Notably, the screw length adequately met the requirements for screw placement across all entry points. The abduction angle and screw length observed at the middle entry point closely aligned with the findings of Xu et al. 20 Furthermore, the screw trajectory of the middle entry point closely followed the OC axis. Given that oval-shaped OCs are prevalent, 22 the medial entry point provides a more extensive abduction angle during anterior OC screw placement. Despite offering a similar screw length to the middle entry point, the medial entry point necessitates a broader OC exposure during actual screw placement, and it is difficult to obtain a larger abduction angle through a transoral approach. The lateral entry point poses challenges in controlling the screw placement's abduction angle, increasing the likelihood of foramen magnum damage, and also featuring a disadvantageous screw length.
The cranial angle is a pivotal parameter to consider in avoiding damage to the hypoglossal canal and atlanto-occipital joint during screw placement. 23 A cranial angle of 10° or less is recommended to avoid intraoperative violations of the hypoglossal canal during posterior OC screw placement. 24 In our study, we utilized McRae's line as a reference for measuring the cranial angle of screw placement. Larger cranial angles and wider safe cranial angle ranges were achievable at the middle and lateral entry points. The entry point, SAA, and cranial angle are integral components of the screw placement trajectory. For a given screw entry point, appropriate screw length, and relatively fixed screw abduction, the cranial angle becomes the variable parameter for controlling the screw trajectory. Forbes et al. 25 reported an average angulation in the sagittal plane of 0.16° inferior to the palatal line. Xu et al. 20 demonstrated the ideal abduction angle for the anterior OC screw to be 5.9° ± 3.4°. Our findings indicated that the highest success rate for all three entry points was achieved by maintaining a cranial angle of 4° within OCs suitable for screw placement at each entry point. At success rates exceeding 60%, a reasonably wide range of cranial angles was feasible at the middle and lateral entry points. Additionally, when cranial angles were controlled within the range of 2° to 6°, a screw placement success rate exceeding 90% could be attained at all three entry points. Consequently, considering the collective influence of each screw placement parameter, we conclude that the feasibility of screw placement at the medial entry point is limited, rendering it unsuitable as an entry point for anterior OC screw placement.
While the success rates of the medial and lateral entry points are comparable, the middle entry point offers an advantage in terms of screw length. Therefore, our recommendation is to opt for the middle entry point as the optimal choice for anterior OC screw placement. It is advisable to maintain the SAA parallel to the mid-axis of the OC, while aiming to control the screw cranial angle at approximately 4°.
Limitations
This study has several limitations. First, the sample size and age distribution of the subjects may not be ideal for establishing normative standards. Second, the 3D model utilized in this study was constructed from normal head and cervical CT data, potentially leading to variations in parameters for anterior OC screw placement when dealing with abnormal or craniovertebral junction disabilities. Third, the study participants exclusively comprised Chinese individuals, potentially limiting the generalizability of the findings to other ethnicities. Finally, this study did not involve practical surgical applications or assessments of biomechanical stability. Computerized three-dimensional reconstruction with simulation of screw placement cannot accurately reflect all anatomical structures around the OC; therefore, studies in cadaver specimen study are recommended to further explore the feasibility of this technique.
Abbreviations
computed tomography craniovertebral junction occipital condyle screw screw abduction angle maximum cranial angle minimum cranial angle safe range of cranial angulation screw length
Footnotes
Acknowledgements
The authors thank all participants for their commitment to this study.
Author contributions
Zhenqi Lou: methodology, software, writing—original draft. Jieyang Zhu and Sihui Chen: data curation, formal analysis. Sanqiang Xia: software. Jinyu Zhu: writing—review and editing. Yi Jiang: methodology, funding acquisition. Kanling Jiang: conceptualization, writing—review and editing. All authors read and approved the final manuscript.
Data availability statement
The datasets generated during this study are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical statement
This study was approved by the ethics institution of Affiliated Hospital of Jiaxing University (LS2020-31) and written informed consent was obtained from all participants.
Funding
This study was supported by the Key Laboratory Project of Jiaxing, China (2022-yzcsgtjzjz) and the Key Departments of Jiaxing, China (2023-ZC-012).