
Abstract
Background
The management of facial fractures varies due to a variety of reasons in the pediatric age groups. The clinicians should therefore attune themselves to managing pediatric patients and the variations thereof. Every modality mentioned in the literature has its own advantages and disadvantages. The right choice of treatment by clinicians depends on their knowledge of pediatric anatomy, physiology, age-dependent bone growth, and the type and extent of fractures. Three different modalities of treatment in the form of circummandibular wiring, intermaxillary fixation and open reduction, with internal fixation were rendered to the patients, considering various factors such as the patient’s age, location of the fracture line, status of occlusion, and dentition. All three modalities showed good results in the form of adequate reduction and no post-op complications.
Conclusion
Pediatric trauma is a challenging entity for the surgeon. The choice of the ideal treatment modality ultimately depends on the presence of tooth buds and the maintenance of uninterrupted growth of the jaw bone. Thus, a well-thought-out and customized treatment plan should be devised for each individual case.
Keywords
Introduction
Pediatric facial fractures are rare, but the incidence increases with age. The mechanism of these injuries changes within pediatric age groups due to the changing architecture of the bones and age-dependent activities by the children. A 5-year-old child will be more engaged in indoor activities than a child of early adolescent age, who will be engaged in outdoor activities, and thus more traumatic injuries are seen in the latter. The bones of younger children have more organic components and therefore tend to bend rather than break under an external force. 1 The underdeveloped paranasal sinuses further strengthen the facial bones of the children against fractures. 2 Compared to other facial bones, the mandibular growth is the last to complete. Therefore, any impact on the growth and development of the mandible can cause significant facial deformity and aesthetic compromise. While considering treatment for pediatric mandibular fractures, multiple factors have to be considered, such as the status of the dentition, the anatomical location of the fracture in the mandible, and the age of the child. These factors will ultimately guide the clinician to use the best modality of management. As a general rule of thumb, it is always advised to approach pediatric fractures as minimally invasively as possible, keeping in mind the growth, esthetic, and functional outcomes without compromising the fracture reduction stability. Here we present three such case reports of mandibular fractures that were treated with different modalities considering the above factors. We used closed reduction with intermaxillary fixation (IMF), closed reduction with an open cap splint, and open reduction with internal fixation.
Case 1
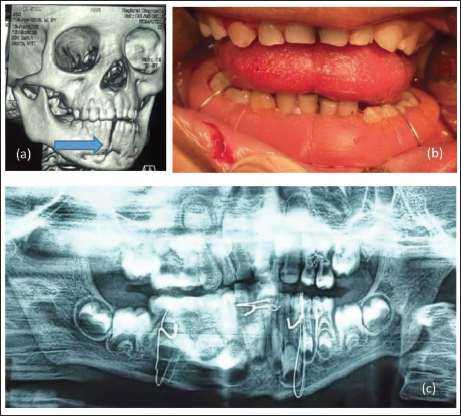
A 5-year-old boy reported to our department with a 1-day history of a road traffic accident (RTA) sustaining a fracture in the mandibular symphysis region (Figure 1a). On examination, an obvious step deformity and mobility were noted between the lower central incisor teeth. The patient had all primary teeth erupted, and no gross malocclusion was noted other than a slight open bite visible in the left canine region. Since primary dentition is not suitable for dental wiring, we ruled out the possibility of closed reduction using such a modality. Open reduction and internal fixation was also ruled out to avoid injuring permanent tooth buds and requiring subsequent implant removal surgery. Consequently, we planned for an open cap splint with circummandibular wiring using intravenous cannula stillete (IVCS) with a modified approach from how it was used earlier. 3
A 5-year-old Boy with a History of RTA. (a) Pre-op Three-dimensional Computed Tomography Scan of Patient Reveals Symphysis Fracture with Deranged Occlusion of the Left Side. (b) Intraoperative Fracture Reduced and Stabilized Using Cap Splint with Circummandibular Wiring. (c) Post-op Orthopantomogram (OPG) of the Patient.
Technique
A 16-gauge IVCS was inserted into the submandibular region and exited into the lingual vestibule while keeping the cannula as close to the lingual cortex as possible during insertion. The needle was removed, and a 26-gauge stainless steel wire was passed through the cannula intraorally to its full length to exit extraorally through the cannula. The intraoral side of the wire was clamped and secured. The cannula was then railroaded through the wire and exited extraorally. The needle was put back into the cannula and then inserted into the buccal vestibule adjacent to the intraoral wire position. The cannula was carefully brought out through the previous extraoral entry adjacent to the previously exited wire. This wire is now carefully bent, reintroduced into the cannula, and brought out in the buccal vestibule after removing the needle. The cannula is railroaded through the wire and exited intraorally. The necessary digital reduction of the fracture was done. The prefabricated open-cap splint was then placed over the lower arch, and wires were brought together and twisted over the splint, securing it to the arch (Figure 1b).
Case 2
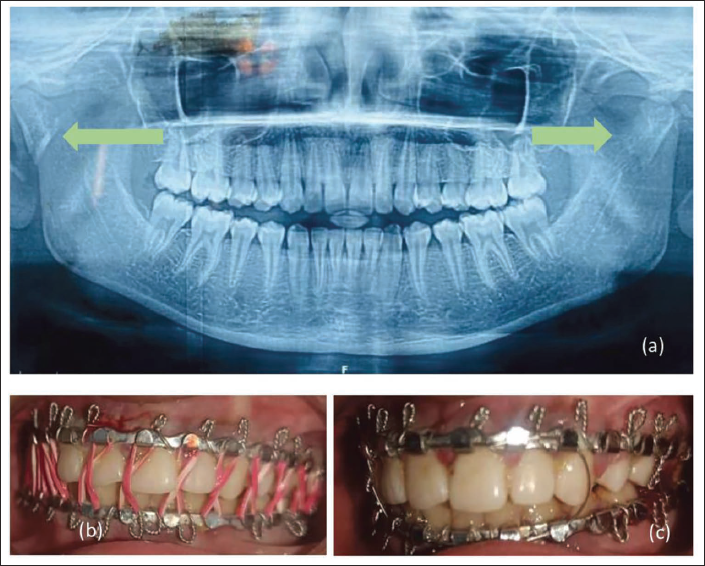
A 12-year-old girl reported to our department with a 2-day-old history of fall while playing at home and sustained a mandibular fracture in the subcondylar region bilaterally (Figure 2a). On examination, the patient had an anterior open bite with difficulty in opening the mouth due to pain in the bilateral preauricular region. Since the patient had all her permanent teeth erupted, we planned for closed reduction with IMF using elastic traction with Erich’s arch bar for 5 days. On follow-up, elastics were removed after achieving satisfactory occlusion, and IMF was done with 26-gauge stainless steel wire for 9 days (Figure 2b and c). The patient was advised to do active mouth- opening exercises post-IMF release.
A 12-year-old Female with a History of Fall. (a) Pre-op OPG of Patient Reveals Bilateral Subcondylar Fracture of the Mandible. (b) Closed Reduction with IMF (Erich Arch Bar) done Under LA, Occlusion Achieved, Patient kept on Elastics for 5 Days. (c) Elastics Replaced with 26-Guage Stainless Steel Wire of Next 9 Days.
Case 3
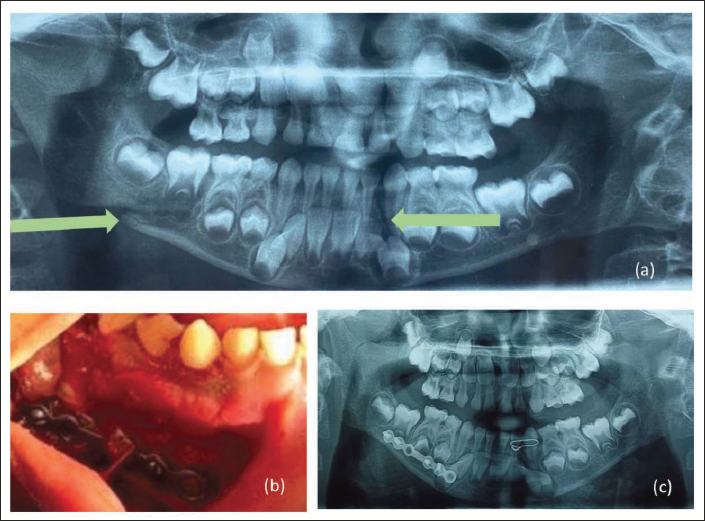
A 7-year-old girl reported to our department with a 1-day history of RTA and a sustained fracture of the mandible in the right body and left parasymphysis region (Figure 3a). On examination, the patient had an anterior open bite. Although there is consensus for closed reduction modalities in the management of pediatric fractures, we chose open reduction and internal fixation for the right mandibular body fracture. The left parasymphysis fracture was stabilized with bridle wiring between the primary lateral and canine. Due to mixed dentition, the stability of interdental wiring and arch bars were doubtful. We could not plan for cap splints due to the posterior tracing of the right body fracture and the possible instability of the proximal segment with such a modality. The miniplate fixation was removed after 3 months for uninterrupted growth of the mandible.
A 7-year-old Girl with a History of RTA. (a) Pre-op OPG of Patient Reveals Left Parasymphysis and Right Mandibular Body Fractures. (b) Intraoperative Fracture Reduced and Fixed with a 2.0 mm Miniplate. (c) Post-op OPG of the Patient.
Discussion
Pediatric fractures have a lower incidence than adult fractures due to various reasons. The most important reason is the protective environment they are kept in. The inorganic-to-organic ratio in pediatric bone is lower as compared to adult bone, and therefore it takes a considerable amount of force to fracture the bone to communition. 4 The underdeveloped paranasal sinuses of the pediatric facial bone further strengthen it against external forces. Therefore, we tend to mostly observe greenstick fractures in children. The occurrence of trap door fractures of the orbital floor is a good example of this phenomenon.
Midface fractures are a rare entity in pediatric facial fractures due to their retruded position in the maxillofacial skeleton. 4 The second most common fracture in the pediatric age group is the mandibular fracture after the nasal fracture. 1 This is due to its prominent position in the facial region. The mandible houses the permanent tooth buds, which dictate the growth of its alveolar process. Since the mandible is the last bone to attain maturity in the facial skeleton, any trauma to this bone can cause significant facial deformities for the child.
The importance of the management of facial fractures stems from the idea that this period is crucial for the psychosocial development of a child. A traumatic facial disproportion in a child’s face can have a debilitating effect on his or her self-esteem. Clinicians should therefore enable themselves to approach pediatric cases in such a way as to support the child both physically and emotionally. The goal of the treatment must therefore be focused as much as possible on rapid wound healing, ideal functional reestablishment, and superior esthetic results. The rapid healing nature of the child’s system will support the clinicians in achieving good results, but it also depends on the ability of the surgeon, timing of intervention, duration of intervention, and follow-up care.
While designing the treatment protocol for pediatric fractures, certain absolute criteria are to be considered, such as age, the status of the dentition, the general health status of the child, and socioeconomic background. Most pediatric undisplaced fractures don’t require active intervention and just need supportive care. Rigid internal fixation is often avoided to avoid growth interruption, and a conservative approach is usually contemplated. 5 In modern practice, the use of dental wiring and its derived methods are often applied to stabilize pediatric fractures. It helps maintain tissue integrity as compared to open reduction. The case selection for close reduction protocols depends on factors such as dentition, age, and so on. The anatomy of primary dentition is less favorable for the retention of wires and therefore results in treatment failure. A child with a full complement of permanent teeth can be an ideal candidate for close reduction with dental wiring or even arch bars. In the case of a primary or mixed dentition, it is always better to use prefabricated occlusal splints stabilized by circummandibular wiring or cementation. 6 The use of IVCS in place of a bone awl considerably reduces the entry/exit wound size and associated soft tissue injuries. 7
The use of occlusal splints depends on their ability to stabilize the fracture after reduction. 8 A fracture that traces much posteriorly toward the angle region is less favorable for such a modality. In such cases, an open reduction with miniplate internal fixation is a better option. To avoid injuries to the permanent tooth buds, a detailed pre-radiographic assessment should be carried out. The implant should be placed by leaving a safety margin, and most often this is the lower border of the mandible. 9 The use of monocortical screws with micro or miniplates should be a consideration. Recent advances to avoid second-stage surgery for implant removal have included the incorporation of bioresorbable plates in pediatric trauma management. Its usage has been limited due to evidence of osteolytic changes caused by it during disintegration. 10
Most pediatric mandibular fractures can be treated conservatively, but there are clear indications for open reduction, and the clinician must always consider the risk versus benefit factor.
Conclusion
Despite best efforts, pediatric fractures are always a challenging entity for clinicians across the globe. Multimodal management always brings out the best results, and consideration of growth disturbance, psychosocial development, and rehabilitation of the pediatric population are of utmost importance.
Authors’ Contribution
Neelima Gehlot and D.S. Gupta − Operating surgeons, concept design, manuscript editing and review.
Sooraj S. Pillai and Snigdha Singh- Assisting surgeons, manuscript preparation, Literature search, data acquisition and analysis, article revision.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Statement of Informed Consent and Ethical Approval
This study was performed in line with the principles of the Declaration of Helsinki as revised in 2013.
This work involves human participants but no animal participants are involved.
Informed consents have been taken from each of the human participants for publications of this research work.
Patients reporting to the OPD of Oral and Maxillofacial department of Teerthanker Mahaveer Dental College and Research Centre are reported in this article.