
Abstract
Abstract
Background: This prospective study is done to assess weight loss due to maxillomandibular fixation (MMF) in patients who have undergone treatment for maxillofacial fractures. This fixation method is a closed reduction technique that can interfere with normal nutrition intake of solid and semisolid foods and thus can result in weight loss and malnutrition. Therefore, in this study we explain the degree and pattern of weight loss in patients treated with MMF.
Materials and Methods: We treated 300 patients for 4 to 6 weeks of MMF. We measured and compared the weight before and after MMF.
Results: The loss of weight was statistically significant (P < .001) with MMF treatment.
Conclusion: MMF caused mild to moderate malnutrition in some cases so protein diet was recommended to such patients post treatment.
Introduction
Maxillofacial fractures are caused by road traffic accidents, fall from height, interpersonal fights, and injuries during games.1–3 Mandible fractures can be treated by two methods. An incision is given to expose the fracture site in open reduction techniques and fractured segments are immoblized using screws and plates. The maxillomandibular fixation (MMF) is done in the closed method of reduction4–5 Although MMF can lead to malunion, non-union, and periodontitis, still it is a common method of treatment. 5 The period of MMF is 3 to 6 weeks.6, 7 During the period of MMF, the intake of food is decreased affecting the healing process of the body. 8 Advantages of MMF are that it is inexpensive and not technique-sensitive. But MMF is not risk-free as patients may vomit during MMF period. Patients with MMF may lose weight.5, 6, 14 Those with respiratory disorders such as asthma have been shown to have deterioration in their respiratory function. Patients also dislike MMF. They have difficulty in maintaining normal diet and oral hygiene.4, 7 There are possible temporomandibular joint sequelae, muscular atrophy and stiffness, denervation of muscles due to alterations in fiber types, irreversible loss of bite force, weight loss, and risk of inflicting injuries to operators manipulating wires.8–11
Methods and Materials
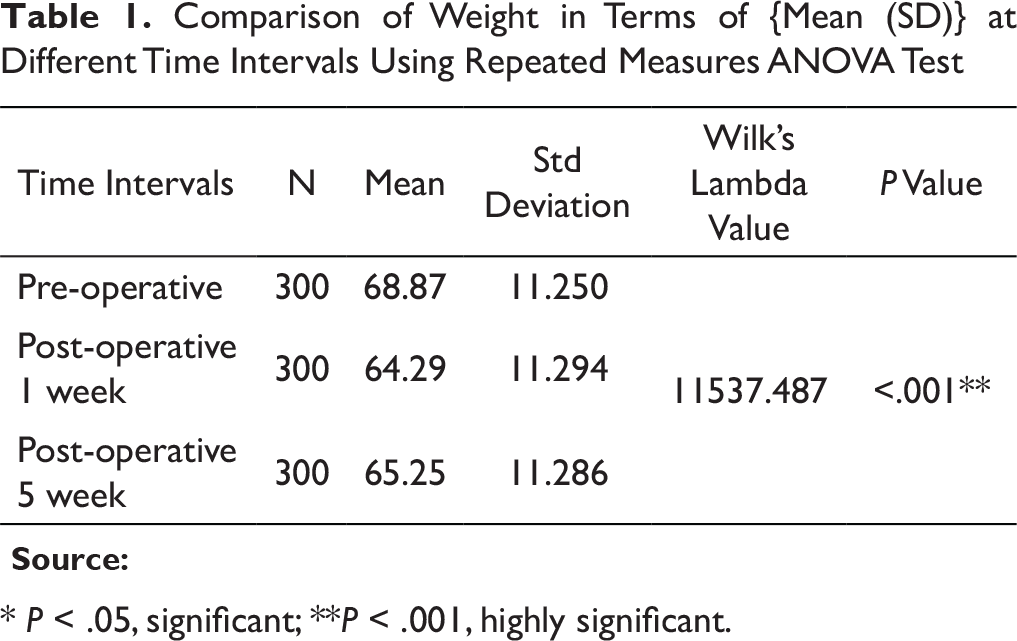
This prospective study was performed in Oral and Maxillofacial Surgery (OMFS) Department, Indira Gandhi Government Dental College (IGGDC), Jammu. We treated 300 patients of mandibular fractures. Among these patients, 270 patients were males and 30 females, age ranging from 15 to 50 years. The pre-operative weight ranged from 45 to 89 kilogram (kg). All patients were treated with MMF for 5 to 6 weeks. Weight of the patients was noted pre-operatively, first week post-operatively, and fifth week post-operatively. The net weight loss observed was 5.5 kg at the end of the first week post-operatively and 5 kg in the fifth week post-operatively when compared with their weights before MMF. Within the limitations of this study, significant weight loss was observed at the first week post-operatively among all patients. At the release of MMF, the weight measurements were done again.
Results
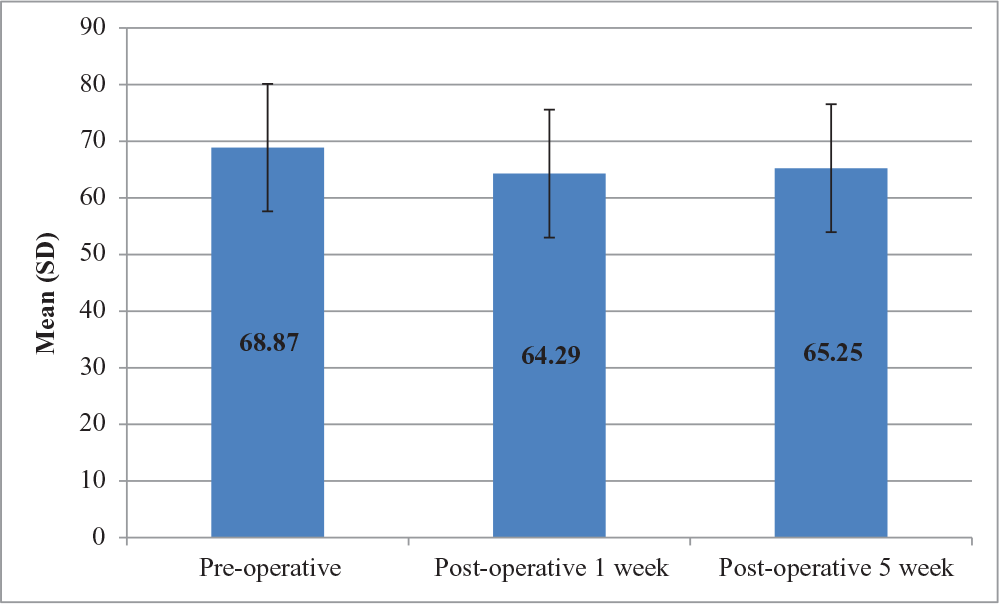
Comparison of Weight in Terms of {Mean (SD)} at Different Time Intervals Using Repeated Measures ANOVA Test
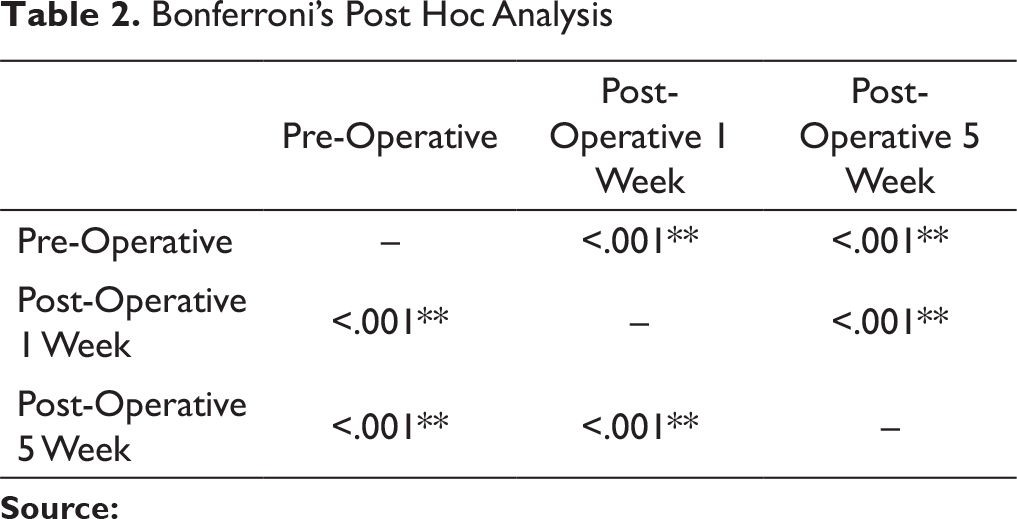
Bonferroni’s Post Hoc Analysis
Comparison of Weight in Terms of {Mean (SD)} at Different Time Intervals
Discussion
Treatment like MMF decrease patients’ ability to eat during the early days or first 24 to 48 hours but after that they are able to resume a normal liquid diet.4–6 Patients with fractured mandible find it difficult to take normal diet for 6 to 8 weeks.10, 12, 13 Surgery and anesthesia disrupt the metabolic steady state initiating a catabolic process which is intensified by periods of limited nutritional intake. A normal adult requires 1800 to 2000 calories per day. Some studies have demonstrated how MMF reduces body weight and other indexes like BMI. Muscle is catabolized for glucose production (gluconeogenesis) early in this phase, with additional protein breakdown from the metabolically active tissues that have been wounded surgically. 14
In this study, the net loss of weight was 5.5 kg at first week post-operatively due to decrease in carbohydrate and protein intake. All patients in this study had mandibular fractures and were treated with MMF alone. Patients had difficulty in maintaining nutrition intake during the first week post-operatively but soon adjusted to liquid diet after one week.
In this study, only weight of the patient was noted irrespective of their nutritional diet, socioeconomic status, healing, and post-operative complications. The overall weight loss in this study is 5 kg which is in comparison with the study done by Worrall in which total weight loss was 4.6 kg. 14 Further, more patient started to gain weight by the fourth post-operative week. 4 In other similar studies, no significant weight loss was observed after 4 to 6 weeks of intermaxillary fixation (IMF). Another study in which IMF was used to control obesity also showed that prolonged use of IMF had no significant effect on the weight of the patient.15–17
The weight of patients were calculated and analyzed for results using Bonferronis Post Hoc Analysis (Table 2). Similar studies confirmed our results of average loss of 5.4 Kg. 18 but Ellis observed 4.5 kg loss in weight of patient during 6 weeks of treatment 19 , and Luhr et al confirmed weight loss of 4.1 kg after 3.5 weeks. 20 In another study of 2004, MMF done in obesity showed an average weight of 7.4 kg. 21 The loss of weight in this study was less compared to other such studies. A weight loss of more than 10% of the body weight is a sign of malnutrition. 22 Because weight loss did not reach 10% in this study, like most of the studies, we can assume that treatment with MMF for 5 to 6 weeks did not result in malnutrition as patients adapted to liquid diet after a brief period of a few days.
Conclusion
In conclusion, this study shows that the decrease in nutritional intake after MMF will result in mild malnutrition. So protein supplement should be added in liquid form as MMF restricts solid and semisolid diet.
Footnotes
Acknowledgment
The authors thank and acknowledge the efforts of Ayera Bashir, Zain ul Aarifeen, Ayesha Nisar, and Maryam for their support in formulating and tabulating the results.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.