
Abstract
Introduction:
Facial fractures in children account for 15% of all facial fractures in the general population. Children are more likely to have mandibular fractures than midface fractures, with condylar fractures being the most prevalent, followed by parasymphysis, angle, and body fractures. The low prevalence of mandibular fractures in children can be linked to the safe environment they are provided with as well as their unique growing patterns. Pediatric patients present a unique challenge to maxillofacial surgeons in terms of their treatment planning and in their functional needs.
Materials and Methods:
A prospective analysis of pediatric patients with mandibular symphysis/parasymphysis/body fractures operated from January 2016 to October 2021 was performed. Clinical photographs and orthopantomogram assessment at the time of presentation, after treatment, and at 6 months postoperatively were evaluated.
Result:
All 17 patients were followed up until the period of 6 months, and none of them had any major complications. Postoperatively, there was satisfactory healing and union of fracture fragments in all the patients. Only 1 patient developed an infection in the submental region. In each case, the surgical splint was removed during 15 to 21 postoperative days. The 6-month follow-up showed good occlusion, without interference in teeth eruption, and no signs of temporomandibular joint problems.
Conclusions:
In our study, because of the sheer ease of fabrication, maintenance of periodontal tissue integrity, patient compliance, and convenience of measuring the occlusion following reduction, we chose an acrylic cap splint followed by circummandibular wiring.
Introduction
When children are young, their impulsive temperament and adventurous spirit combine to urge them to engage in harmful physical activities with little regard for the long-term effects. This usually results in facial injuries; nevertheless, facial injuries in children are far less prevalent than they are in adults. Fractures in children might be difficult to see. Facial fractures, especially mandibular fractures, can present subtly, with minimal discomfort or edema. The great potential for healing in the shortest time feasible and the intrinsic ability to adjust to new surroundings that we see in children differ substantially from what we see in adults. Regardless of the patient's age, the fundamentals involved in the treatment of facial injuries remain the same. Surgical procedures in children, on the other hand, must be adapted to anatomical, physiological, and psychological aspects.
Facial fractures in children account for 15% of all facial fractures in the general population.1, 2 Children are more likely to have mandibular fractures than midface fractures, with condylar fractures being the most prevalent, followed by parasymphysis, angle, and body fractures. The low prevalence of mandibular fractures in children can be linked to the safe environment they are provided with as well as their unique growing patterns.1, 3 Other causes, such as preventive legislation (speed limits, helmet use, airbags, and so forth), have also contributed to their low frequency. Road traffic accidents, falls, sports, and birth trauma are among the etiologies listed in the literature, as well as those seen in our series.4, 5
The anatomical complexity of the developing mandible, notably the existence of dental buds, deciduous tooth eruption, and permanent tooth eruption, dictate treatment planning in children. Traditional techniques of fracture reduction and fixation used in adults, such as open reduction and internal fixation, are ineffective in children. Splinting a broken pediatric mandible with an acrylic cap splint and circummandibular wire is a simple, time-tested, and successful treatment option for a range of pediatric facial injuries.
Here, we will be discussing our experience for placement of acrylic cap splint using circum-mandibular wiring for the treatment of pediatric mandibular fractures.
Material and Methods
A total of 17 pediatric patients reported to the Department of Oral and Maxillofacial Surgery were included in our study. Patients with mixed dentition and having symphysis, parasymphysis, and body of mandible fractures were included in the study. Angle, condylar, and other mandibular fractures associated with pan facial fractures were excluded. The diagnosis was made by clinical and radiographic findings.
Procedure
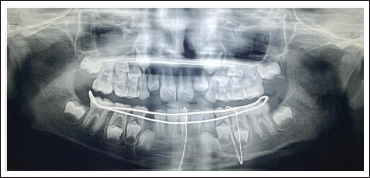
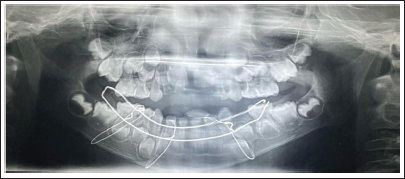
Upper and lower arch alginate impressions and stone casts were made, and the occlusal acrylic splint was fabricated. Any previous photograph of the patient smiling or earlier dental treatment records are always helpful in the execution of mock surgery on casts (Figures 1 and 2). Following mock surgery, cast segments were reduced and occluded with a maxillary cast; later, acrylic splints with an open occlusal surface were created in each case containing lingual and buccal flanges (Figures 3 and 4). Under general anesthesia, stab incisions were placed in the submandibular and submental regions to facilitate passage of mandibular bone awl (Kelsey–Fry), which was then used to enter lingually along the body of the mandible through stab incision and piercing lingual mucosa. A 26 gauge stainless steel wire was passed through the eye of the awl and secured. It was then passed through the same stab incision along the body of the mandible to again enter intraorally through the buccal vestibule. Care should be taken to keep the mandibular awl as close as possible to the surface of the mandible to minimize soft tissue injury. At least 1 wire was passed on either side of the fracture, taking care not to injure the mental neurovascular bundle. Again, the mandible was held in occlusion with the splint in position; both buccal and lingual ends of wires were held together, and the splint was stabilized by twisting the wire in a clockwise direction in the respective regions. Finally, occlusion was rechecked, and the stability of the splint was verified.



Result
The age of patients included in the study group ranged from 1 to 15 years, mean age being 10.9 years. Of these 17 patients 10 were females, 7 males. On the whole, 7 patients were males and 10 were females, and the mean age of the patients was 10.9 years (range, 1–15 years; median, 12; standard deviation, 3.8). Data of the 17 patients with mandibular symphysis/parasymphysis/body fractures treated with cap splint followed by circummandibular wiring from January 2016 to October 2021 records were retrieved and evaluated. All 17 patients had a follow-up period of 6 months, and none of them had any major complications (malunion, malocclusion, temporomandibular joint pain). Postoperatively, there was satisfactory healing and union of fracture fragments in all patients. In each case, the surgical splint was removed during 15 to 21 postoperative days (Figures 7 and 8). With regard to wire placement and removal, none of the patients had any obvious swellings postoperatively. The 6-month follow-up showed good occlusion, without interference in teeth eruption, and no signs of temporomandibular joint problems.


Discussion
Approximately 5% of all facial fractures occur in children. 4 Male predilection is seen in all age groups. Falls and sports accidents are the most common causes of mandibular fractures in youngsters. Because the type and frequency of fractures received by children varies from those sustained by adults, pediatric patients provide a particular challenge to the maxillofacial surgeon. Because of anatomic variations, rapid healing, patient cooperation, and the possibility of changes in mandibular development, the management of fractures in children differs from that of adults.6, 7
Acrylic splints, circum-mandibular wire, arch bar, or gunning splints can be used to accomplish closed reduction and stability. 8 These approaches give a good decreased position, periosteal sleeve continuity, and soft tissue preservation, resulting in a favorable environment for accelerated osteogenesis and remodeling processes, as well as the prevention of nonfibrous union. 8 Although open reduction and fixation with resorbable osteosynthesis plates and screws is becoming more popular in pediatric patients, these systems are not beyond problems, such as poor mechanical properties and difficulty in managing these resorbable implants.9, 10
Because of children’s stronger osteogenic potential, faster healing time, and less frequent need for open reduction and internal fixation, complications are uncommon in pediatric trauma. 4 Nonunion of the mandible can occur as a result of a variety of causes, including poor patient compliance with postoperative instructions, metabolic problems, and systemic diseases, all of which can result in insufficient bone repair. Vaithilingam et al 11 encountered tears in the floor of mouth resulting in hematoma in 3 out of 22 (13.6%) pediatric patients; however, in our study, none of the patients developed a postoperative hematoma. Vaithilingam et al 11 noticed postoperative swelling at average of 5.85 mm in 22 pediatric patients, whereas in this study the average of postoperative swelling was 5.83 mm. We found no evidence of occlusal problems when closed therapy was used. According to the research conducted by Kaban et al, this finding is correct. 12 Cap splints are an excellent alternative for pediatric fracture management. Circummandibular wires are introduced using Kelsey–Fry awl. The fracture segments are properly secured in the splinted mandible, which helps to reduce pain and discomfort during daily activities for children. 8
Conclusion
Facial fractures amongst children are a prevalent form of injury in pediatric trauma patients. Understanding the link between oral injuries and maxillofacial fractures plays a crucial step in preventing them. The majority of these fractures are resolved with conservative measures. Causes and patterns of facial fractures vary from one case to another with age.
In our study, because of the sheer ease of fabrication, maintenance of periodontal tissue integrity, patient compliance, and convenience of measuring the occlusion following reduction, we chose an acrylic cap splint followed by circummandibular wiring. Although this procedure is a time-tested and oldest surgical intervention for the management of pediatric mandibular fractures, a few studies have shown that its success rate is not 100%. With this study, we hope to explain the surgical method that will result in 100% success rate while minimizing the risks connected with this technique.
Other surgical interventions, such as bone plating with stainless steel or titanium plates, can obstruct the eruption of the permanent dentition or harm the permanent dentition's tooth bud. A resorbable plating system is another alternative; however, it is a technique-dependent and cost-effective technology. Furthermore, both these procedures necessitated a wide vestibular incision, which could result in a sublingual hematoma, postoperative edema, or harm to the mental or facial neurovascular bundle. The incision line also took roughly 10 days to heal, and it led to vestibular fibrosis.
As a result, in pediatric children with mixed dentition, the treatment method described in this article is the preferred option. To conclude, the use of an acrylic cap splint with circum-mandibular wiring in pediatric mandibular fractures is a novel and simple technique with minimal or no problems, according to the study.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Necessary ethical clearances and informed consent was received and obtained respectively before initiating the study from all participants.