
Abstract
Fractures of the lower jaw bone come with a unique set of challenges due to their effects on the overall health of the individual. An untreated jaw fracture can lead to malunion, which can ultimately affect the neuro-muscular-occlusal coordination of the masticatory unit. The fractures of the non-dentate regions of the mandible are difficult to manage conservatively, especially in the angle region, due to various muscular activities. The difficulty is coupled when the fracture is present bilaterally, and an exclusive treatment modality should be devised on a case-by-case basis. Bilateral angle fractures of the mandible are rare occurrences and are seldom reported compared to unilateral angle fractures. The difficulty in access and the presence of three unstable fragments and third molars in this region warrant the special attention of the surgeon in devising the treatment plan. For effective management of bilateral angle fractures, surgeons require in-depth knowledge of the biomechanics and anatomy of the jaw bones. This article reports a rare case of isolated bilateral angle fracture management post-road traffic accident in a young patient with rigid internal fixation using an intraoral and transbuccal approach.
Keywords
Introduction
The mandible is an atypical bone that is bent into a horse-shaped structure, with its strength concentrated over the symphysis region in the midline. This characteristic shape and its dynamic nature make it one of the versatile functional systems of the body associated with mastication. The attachments of various muscles in specific areas of the mandible encompass the clinician to study mandible biomechanics with its various micro-skeletal units. There is a high incidence of mandibular fractures among other fractures, accounting for 23.3%, and standing second to nasal fractures with a most common incidence of 58.6%. 1 The angle of the mandible is the junction of the ramus and corpus, making it an area of multidirectional vectors that are in equilibrium for effective function. The disruption to such a state is seen in cases of fractures involving the angle of the mandible. The proximal location, less accessibility, strong musculature, and presence of an erupting third molar in the angle region make the reduction more challenging than fractures in the dentate areas of the mandible. 2 The fractures involving the angle of the mandible also have a high incidence among mandibular fractures, with a 27%–30% incidence. 1 Though a rare occurrence, bilateral angle fractures come with a unique set of challenges, with a frequency of 2.1%, as evidenced by Cillo and Ellis in a study. 3 There is a considerable change in the biomechanics when there is a bilateral angle fracture. The most important factor is the loss of shielding effect against the displacement by the contralateral angle. There are very few studies reported on bilateral angle fractures due to its rare isolated occurrence.3–7 Here we present a case of an isolated bilateral angle fracture along with a brief discussion on its possible biomechanics and management.
Case Report
A 17-year-old male reported to our department OPD with a history of road traffic accidents and sustained injuries to his chin. The patient presented with a chin laceration and oral bleed. On examination patient had an open bite with contact only in the molars and increased lower facial height. There was no neurosensory deficit along the distribution of inferior alveolar nerves bilaterally (Figure 1).
Pre-operative Occlusion of the Patient. Generalized Open Bite with Posterior Gag of Occlusion is Appreciated.

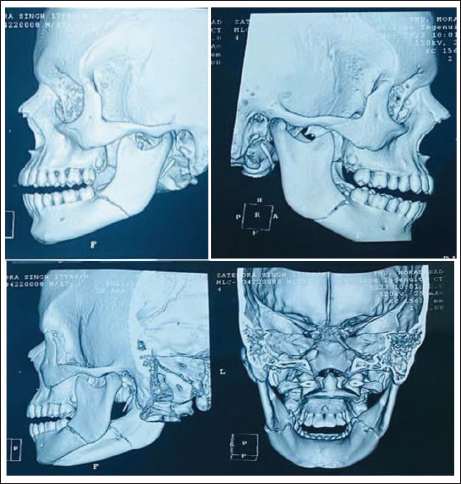
Preoperative CT revealed horizontally unfavorable fractures of the mandibular angle bilaterally and fracture lines were traced along the sockets of the third molar tooth (Figure 2).
3D Reconstruction of Patient’s CT Reveals Bilateral Mandibular Angle Fracture. Both the Fracture Lines Can Be Seen to Traverse in an Unfavorable Path.
The patient was taken under general anesthesia and intermaxillary fixation was done. After exposing the fracture site, the left angle fracture was found to be more displaced, and therefore single miniplate fixation on the superior border was found to be inadequate for absolute stability. Hence a transbuccal approach was employed along with the intraoral approach. A 3D miniplate was used for fixation using trochar. Whereas for right angle fracture, an intraoral approach was used and the fracture was fixed with a miniplate on the superior border (Figure 3). After wound closure, IMF was released and occlusion was checked passively. The third molars were decided to be retained as the root formation was not completed and were expected for further eruption. The patient was kept under close observation postoperatively for three months and the healing was uneventful (Figure 4).
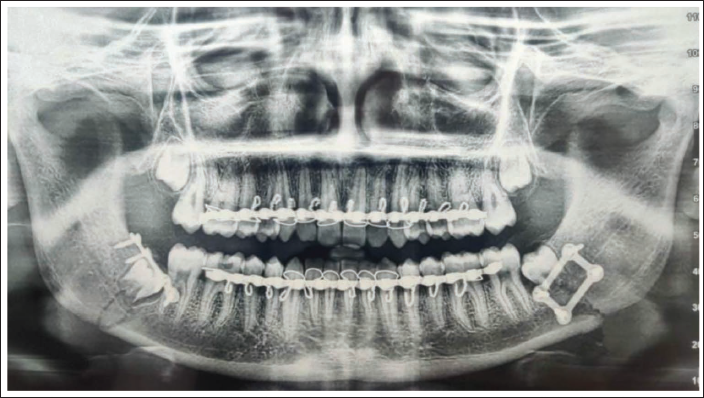
Post-operative OPG of the Patient Showing Fixation of Reduced Fracture Segments with a Four-hole with Gap Miniplate (Right) and a 3D Plate (Left). A Decision of Not Extracting the Third Molars was Made.
Post-operative Occlusion of the Patient—Two Weeks Post-surgical Procedure.

Discussion
The occurrence of bilateral angle fractures is often overshadowed by the presence of other severe fractures of the facial skeleton and is considered wholly under the spectrum of pan-facial fracture management. There is a higher incidence in males than females with angle being one of the common areas of unilateral fracture (30%). 8 Road traffic accidents are the most common causes of mandibular fractures involving the facial skeleton (75.75%). 9 The prominence of the chin often makes it a site of first contact and thus mandible takes a major share of the blow to the face.
While considering the causative factors of unilateral angle fractures, assault or interpersonal violence takes the upper hand. Such fractures are caused by high impact force on the corpus region leading to fracture of the contralateral angle indirectly along with the corpus. In contrast, bilateral angle fractures usually depict a result of centrally placed severe impact force as seen in cases of bilateral condylar fractures. 7
The mandibular angle region being the junction of the ramus and corpus is subject to the influence of various muscles. The fracture of this region leads to disruption of the balanced function of the mandible. In the case of bilateral angle fractures, the mandible is split into three segments, that is, two proximal and one distal corpus segment. The Ramal segments are influenced by the superior pull from the temporalis, masseter, pterygomasseteric sling, and medial pterygoid resulting in a superior vector. Whereas the corpus is under the influence of suprahyoid muscles which results in a downward vector. Together this creates a “Force couple” resulting in an unopposed interfragmentary movement causing gaping. This change in the biomechanics of the mandible results in more fracture displacement tendencies in both pre-fixation and post-fixation periods. Such a unique phenomenon is a major prerequisite for using rigid internal fixation in the management of bilateral angle fractures for superior results.
The presence of a third molar in the angle region contributes to its innate weakness and predisposes it to fractures especially when they are partially impacted in the bone. There are still ongoing debates regarding its removal or retention and a generalized consensus for removal in case of vertical tooth fractures, infections, and hindrances in achieving effective reduction is seen. 10
There are several studies on the management of unilateral angle fractures whereas bilateral fractures are a rarity and thus reported less. The occurrence of malunion and non-union is high in angle fractures due to the dynamicity between the fragments. The chances of poor outcomes are manyfold when bilateral angles are involved. Therefore early and pragmatic management is imperative for superior results.
Conclusion
Bilateral angle fractures of the mandible come with a unique change in biomechanics of the mandible and therefore warrant special consideration in management. Fractures of the jaw bone have a severe impact on a person’s nutritional intake, facial esthetics, and social life. The clinician should therefore make early efforts in establishing premorbid occlusion. The fact that every fracture of the jaw bones depending on its location behaves differently should be acknowledged. A thorough understanding of biomechanical principles is an obligation for better reduction and fixation, thus preventing postoperative complications.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Necessary ethical clearances and informed consent was received and obtained respectively before initiating the study from all participants.