
Abstract
Objective
To analyse the epidemiology of mandibular fractures and the correlation between combined fractures during a 10-year period in central Taiwan.
Methods
This retrospective study analysed data collected from the medical records of patients that had mandibular fractures between January 2007 and October 2017. Data on age, sex, cause of injury, anatomical site of fracture, treatment and complications were obtained and analysed.
Results
A total of 265 patients who received treatment were included in the study. The mean ± SD age was 30.08 ± 13.47 years (range, 6–70 years) and the 21–30 years age group showed the highest incidence of mandibular fractures. The male-to-female ratio was 1.25:1. Road traffic accidents were the most common cause of fracture (206 of 265; 77.74%). The symphysis and parasymphysis area was the most common fracture site (169 of 420; 39.29%). Single-site fracture represented slightly more than 50% of the total 420 fractures. The most frequent combination of two fractures was an angle fracture combined with a symphysis and parasymphysis fracture (29 of 106 double fracture patients [27.36%]). There was a weak positive association between several combinations of fractures.
Conclusions
A better understanding of the influence of age and sex on the mechanism of injury is of great clinical importance in the assessment and diagnosis of fractures.
Introduction
The epidemiology of maxillofacial fractures varies between populations, locations and time periods. 1 Moreover, the mandible is the most frequently fractured adult facial bone because of its prominent and unprotected position. 2 In a 15-year Taiwanese retrospective study, the mandible was the second most common fracture site (24.7%). 3 Furthermore, in a Malaysian study, it was also the most frequently involved bone in maxillofacial fractures. 4
The cause of mandibular fractures, population distribution and fracture site vary among studies,5,6which can be explained by varying economic and social conditions, local patterns of behaviour and laws. 5 A previous study reported that assault was the most common cause in patients in the US, whereas motor vehicle accidents were the most common cause in Turkish patients. 6 The most common site of mandibular fracture in the US was the angle, whereas in Turkey, it was the body. 6 Road traffic accidents (RTAs) were a common cause in Taiwan, 3 especially motorcycle accidents; and it was shown that the condylar neck and head were the most common sites (32.0%), followed by the parasymphysis (21.7%) and symphysis (19.5%). 7
Mandibular fractures can simultaneously involve multiple anatomical subsites. 8 This study aimed to analyse the epidemiology of mandibular fractures and the correlation between combined fractures during a 10-year period by reviewing patient records.
Patients and methods
Patient population
This retrospective study was conducted on data from consecutive patients that had mandibular fractures treated at the Department of Oral and Maxillofacial Surgery, Chung Shan Medical University Hospital, Taichung City between January 2007 and October 2017 using codes of the International Classification of Diseases, Ninth Revision (802.21 to 802.39). Patients with incomplete registered data were excluded from this study.
This study was approved by the institutional review board of Chung Shan Medical University Hospital (approval number: CS19024). All sensitive patient information was removed before analysis. Informed consent was not required according to the institutional review board and this prevented the skewing of the epidemiological data.
Data collection
Clinical characteristics including age, sex, cause of injury, anatomical site of fracture, treatment, duration of hospitalization and complications based on medical charts and images including panoramic radiography and computed tomography were recorded. The causes of the mandibular fractures were classified as RTAs, falls and direct impact by another person or foreign object (assault). Anatomically, mandibular fractures were classified into seven regions: symphysis and parasymphysis, body, angle, coronoid process, subcondyle, condyle neck and condylar head.
Statistical analyses
All statistical analyses were performed using PASW Statistics for Windows, Version 18.0 (SPSS Inc., Chicago, IL, USA). Data are presented as mean ± SD or n of patients (%). The collected data were analysed using χ2-test and contingency coefficient tests. A P-value < 0.05 was considered statistically significant.
Results
A total of 265 patients with mandibular fractures were included in the study. There were 118 female and 147 male patients (male:female ratio, 1.25:1). The mean ± SD age was 30.08 ± 13.47 years (range, 6–70 years). For these 265 patients, 420 fractures were recorded from the medical records and radiography. The highest occurrence of trauma was in the 21–30 years age group, followed by the 11–20 years age group (Figure 1). Of the study patients, 65.28% (173 of 265 patients) were aged ≤30 years.

Distribution of patients (n = 265) with mandibular fractures stratified according to their age groups in a study that aimed to analyse the epidemiology of mandibular fractures in a 10-year period.
Based on an analysis of the cause of mandibular fractures, RTAs were the cause in 206 patients (77.74%), falls in 36 (13.58%) and assaults in 23 (8.68%). Moreover, the details of the RTAs by mechanism of injury are shown in Figure 2. The χ2-test showed a significant association between sex and causes (χ2-test = 8.016, P = 0.0182) (Figure 3).
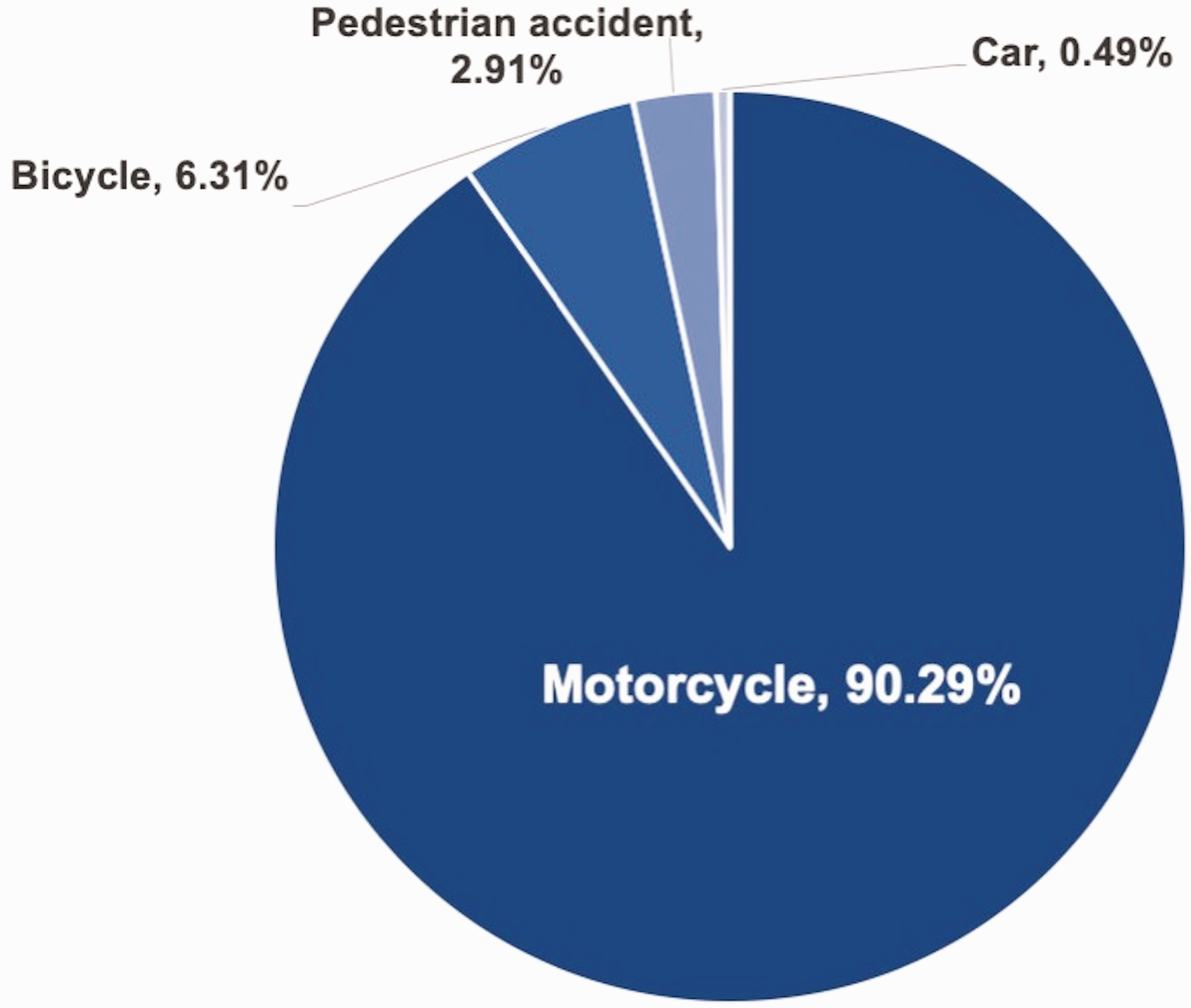
Details of the cause of road traffic accidents in patients (n = 206) with mandibular fractures in a study that aimed to analyse the epidemiology of mandibular fractures in a 10-year period. Motorcycle, 186 (90.29%); bicycle, 13 (6.31%); pedestrian accident, 6 (2.91%); car, 1 (0.49%).

Distribution of patients (n = 265) with mandibular fractures stratified according to their sex and cause of injury in a study that aimed to analyse the epidemiology of mandibular fractures in a 10-year period. The colour version of this figure is available at: http://imr.sagepub.com.
The patients were divided into two subgroups based on the mean age of the cohort with the cut-off being 30 years. The χ2-test showed a significant association between age groups and causes (χ2-test = 9.249, P = 0.0092) (Figure 4).
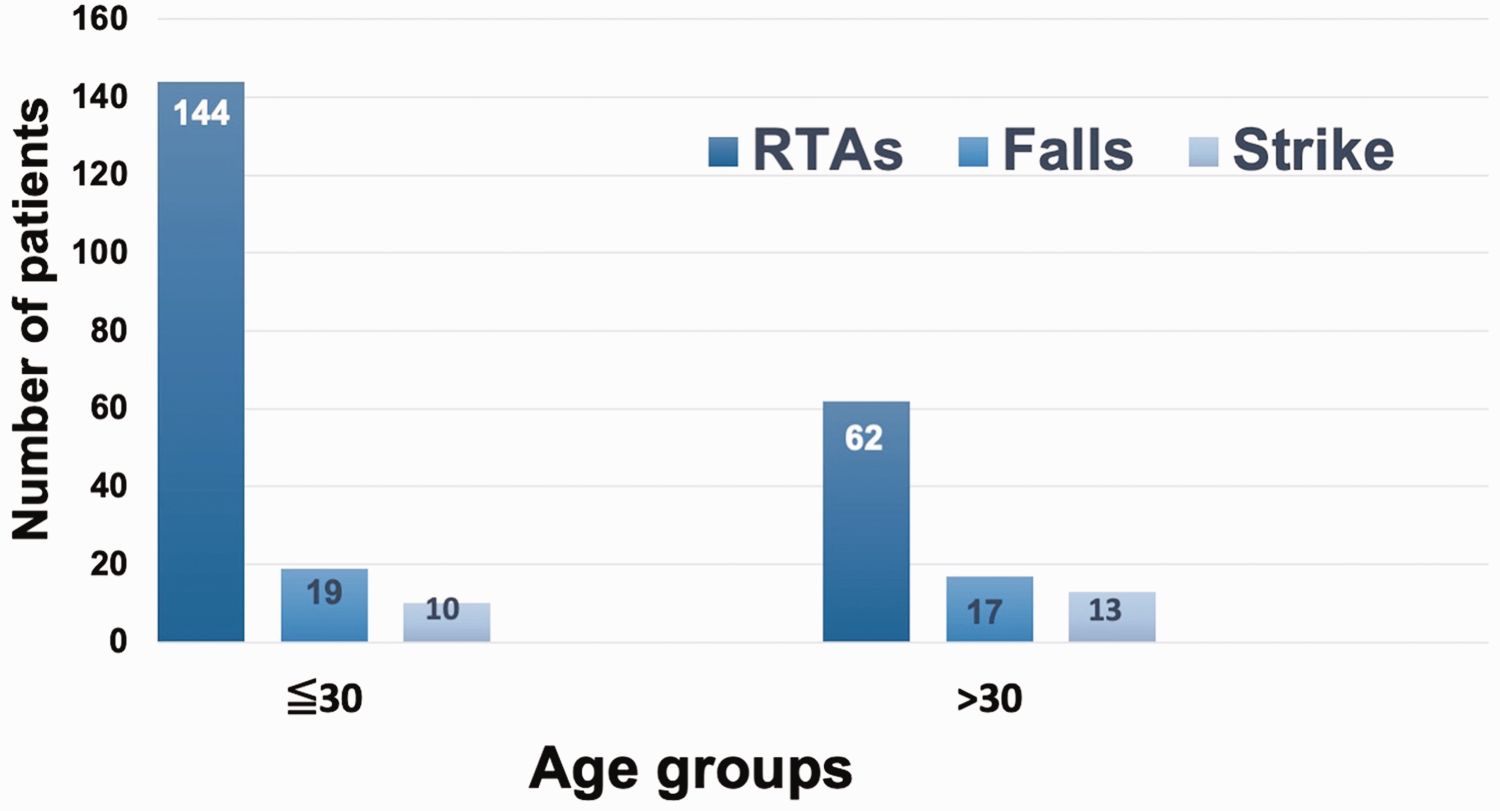
Distribution of patients (n = 265) with mandibular fractures stratified according to their age group and cause of injury in a study that aimed to analyse the epidemiology of mandibular fractures in a 10-year period. The cut-off for the age groups was the mean age of 30 years. The colour version of this figure is available at: http://imr.sagepub.com.
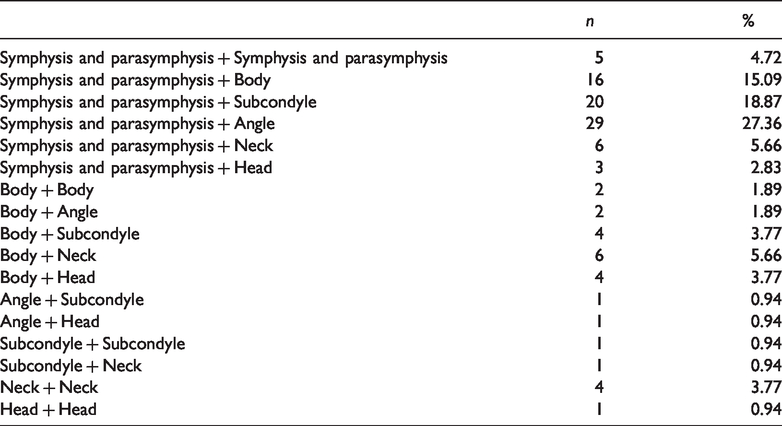
In the total of 420 mandibular fractures, the symphysis and parasymphysis was the most common location (165 of 420 [39.29%]), followed by the mandibular angle (56 of 420 [13.33%]) (Figure 5). A total of 136 of 265 patients (51.32%) had a single mandibular fracture, which was most frequently located in the symphysis and parasymphysis (Figure 6); while 106 of 265 patients (40.00%) had double mandibular fractures. Fracture combinations in these cases are shown in Table 1. There were 17 different combinations of double mandibular fractures. The most frequent combination was an angle fracture combined with a symphysis and parasymphysis fracture (29 of 106 [27.36%]).

Distribution of the location of the mandibular fractures (n = 420) in patients (n = 265) that participated in a study that aimed to analyse the epidemiology of mandibular fractures in a 10-year period. Symphysis/parasymphysis (165 of 420 [39.29%]); body (54 of 420 [12.86%]; mandibular angle (56 of 420 [13.33%]); ramus (52 of 420 [12.38%]); neck (52 of 420 [12.38%]); head (38 of 420 [9.05%]); coronoid process (3 of 420 [0.71%]).

Distribution of patients (n = 136) with a single mandibular fracture stratified according to the location of the mandibular fracture in a study that aimed to analyse the epidemiology of mandibular fractures in a 10-year period.
Distribution of patients (n = 106) with double mandibular fractures stratified according to the combination of two sites in a study that aimed to analyse the epidemiology of mandibular fractures in a 10-year period.
The correlation coefficient was analysed to determine the relationship between two different fractures in the entire study cohort (Table 2). A statistically significant low correlation coefficient was found between the symphysis/parasymphysis and body (r = 0.226), symphysis/parasymphysis and neck (r = 0.197), symphysis/parasymphysis and head (r = 0.243), body and angle (r = 0.183), body and subcondyle (r =0.133), angle and subcondyle (r = 0.214), angle and neck (r = 0.199), angle and head (r = 0.158), subcondyle and head (r = 0.169) and neck and head (r = 0.127) (P < 0.05 for all correlations).
Correlation coefficients between two different fractures in patients (n = 265) in a study that aimed to analyse the epidemiology of mandibular fractures in a 10-year period.

*P < 0.05.
The duration of hospitalization of these patients varied from 2 to 38 consecutive days with a mean ± SD of 5.23 ± 3.34 days. There were 88 patients that underwent maxillomandibular fixation or closed reduction. Moreover, 227 fractures were treated with open reduction and internal fixation (ORIF). Complications were noted in 15 (5.66%) of 265 patients. All patients had at least a 6-month postoperative follow-up period. Of the 15 patients with complications, 12 (80.00%) developed an infection around the fracture line at 6 weeks. One (6.67%) patient had screw loosening and poor healing at 3 months and underwent revision ORIF. One (6.67%) patient had postoperative wound bleeding after 2 days and one (6.67%) patient had partial facial nerve palsy at the operated side.
Discussion
The geographic area, socioeconomic status of the population, dates of injury and mobility of the population vary and affect the results of mandibular fractures. 9 This current study investigated the epidemiology and correlation between mandibular fractures in patients treated at Chung Shan Medical University Hospital over a 10-year period. The epidemiological results were similar to those of previous Taiwanese studies.7,10 Moreover, this current study presented the correlation coefficient between two fracture sites.
In the present study, patients aged 21–30 years (n = 101) had the highest incidence of mandibular fracture. A previous study evaluated mandibular fracture cases in the Department of Maxillofacial Surgery of Lanzhou University between 2011 and 2015 and demonstrated that patients in the third decade of life yielded a high incidence of injury. 11 Similarly, another study reported that the highest incidence of mandibular fractures (49.3%) occurred in the 21–30 years age group. 12
This current study demonstrated that 77.74% (206 of 265 patients) of the mandibular fractures were caused by RTAs, followed by falls and assaults, which were similar to the results of previous studies.11,13 The most frequent cause was motorcycle accidents (186 of 206 [90.29%]). Motorcycle-related RTA was also the major cause of facial injuries in a Tanzanian study. 14 Motorcycles are the primary mode of private transportation in Taiwan. 10 Of a population of 23 million in Taiwan, there are > 14 million motorcycles on the road. 15 There were 1695 motorcyclists killed and 351682 wounded in 2019 alone as recorded in the registry of the Ministry of Transportation and Communications. 16 A previous study reported that wearing partial-coverage helmet for convenience may be the major reason in Taiwan although helmet use is mandatory for motorcyclists. 10
In this current study, the symphysis and parasymphysis was the most common location for fracturs, followed by the mandibular angle. There is a wide variation in the common locations of mandibular fractures.5,6,12,17,18 This may be related to ethnic and socioeconomic differences between countries. Motorcycle accident-related mandibular fractures are mainly observed in the symphysis and parasymphysis regions.11,19 Assault was the most common cause of mandibular fractures in developed countries20–22 and the mandibular angle was the most common site. 22
The most frequent two-fracture combination in this current study was an angle fracture and a symphysis and parasymphysis fracture. A previous study reported that the most common location combination was the body and parasymphysis (22.1%). 8 A specific association between different locations of fractures is an important consideration when performing a clinical assessment of a patient with mandibular fracture. The current correlation analysis of 420 mandibular fractures demonstrated that several combinations showed statistically significant correlations, but all of the correlations were weak. The combination of symphysis/parasymphysis and condylar head fractures showed the highest correlation (r = 0.243) in the current study. Limited data on the correlation between two fractures are available in the literature. For example, condyle fractures were most frequently associated with concomitant symphysis (51.9%), followed by the mandibular body (27.4%). 24 Luhr classes I and II of edentulous atrophic mandibular fractures were also associated with condylar fractures,25,26 as demonstrated in a retrospective study in 12 European departments of oral and maxillofacial surgery; whereas mandibles rated as Luhr class III were associated with body and parasymphyseal fractures. 26 The authors showed that a correlation exists between mandibular condyle and symphysis fractures. 26 This anatomical association is to be expected when a force that is applied to the chin results in a fracture of the mandibular symphysis or parasymphysis and is then transmitted to the condylar region.
This current study had several limitations. First, it was a retrospective study using data extracted from a single institutional database. Secondly, the sample size was modest because there were incomplete medical charts that resulted in patient exclusion. This was because some patients with mandibular fractures had incomplete charts because of the law on medical record storage. Generally, paper-based medical records are kept for at least 7 years according to the law in Taiwan. However, each hospital is allowed to make its own decision regarding keeping a certain type of record for several years based on the requirements of teaching, education and the health insurance system involved. Thirdly, there was no detailed information regarding the presence or absence of a helmet, helmet type and primary sites of force.
In conclusion, this current study demonstrated that RTAs were the most common cause of mandibular fractures and these mainly consisted of motorcycle accidents. The symphysis and parasymphysis was the most common fracture site. The most significant association was observed between the symphysis/parasymphysis and condylar head. To the best of our knowledge, studies on the association between fractures at multiple sites using correlation coefficient analysis are rare and this study has presented the correlation strength. Understanding the epidemiology of mandibular fractures will strengthen the preventive efforts to reduce their incidence.
Footnotes
Authors’ contributions
Study conception and design: Yi-Tzu Chen; acquisition of data: Yi-Tzu Chen, Yu-Wei Chiu; analysis and interpretation of data: Yu-Wei Chiu, Yu-Chao Chang; drafting and revising the manuscript: Yu-Chao Chang, Chiao-Wen Lin. All authors have read and approved the manuscript.
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.