
Abstract
Introduction
Zygomatic bone and its surrounding bony anatomy are essential for maintaining facial contour—cheek prominence and orbital integrity. Management of the zygomatic complex (ZMC) fractures are important in the maintenance of function and facial integrity.
Aim and Objectives
To analyze the incidence, aetiology, surgical management, and complications encountered in the treatment of ZMC fractures in our super-specialty hospital, and to compare the number and location of fixation points and surgical access in our patient cohort with the literature.
Materials and Method
Retrospective analysis of all operative cases (Open Reduction and Internal Fixation) of ZMC fractures over a 3-year period (2017-2021) were reviewed. Craniofacial maxillofacial trauma patient’s medical records were collected and out which only the ZMC fracture cases were reviewed. Only the medical records from the period from 2017 to 2021 were included. The parameters such as etiology, site of the ZMC fracture, type of fracture, associated injuries, clinical findings, treated with conservative or surgical intervention, type of incisions used, number of fixation used, and any complications encountered were reviewed and analyzed.
Results
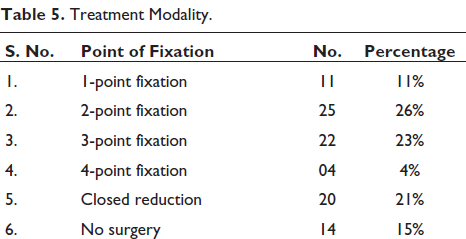
Out of 428 cases of craniofacial injury, 96 cases were ZMC fractures, isolated ZMC fractures accounted for 43%, 33% with associated injuries, 13% isolated arch, while 11% accounted isolated infraorbital rim fracture. Most common clinical findings were subconjunctival ecchymosis (71%), flattening of cheek (39%), malocclusion (22%), and so on. Buccal sulcus incision (66%) was mainly used, followed by upper blepharoplasty incision (59%). Depending on degree of displacement of fracture 1-point fixation (8%), 2-point fixation (30%), or 3-point fixation (27%) was performed. About 33% of cases were conservatively managed and followed up on regular intervals. Lymph edema, infra orbital paresthesia, temporary blindness, diplopia, hemianopsia were some of the complications encountered which were managed successfully and followed up.
Conclusion
ZMC fractures are most commonly occurring midface fractures with variable etiologies. The most common ZMC fracture pattern was tripod type of fracture. Greater portion of the patient were treated with 2-point fixation. Most of the complications were due to the impact and velocity of trauma.
Introduction
The zygoma is the paired irregular bone that plays an important role in facial contour and esthetics of the face in the human body. It plays a major role in influencing the width of face and major buttress of midface between maxilla and cranium. 1 Zygomatic bone forms the major coupling in the midface and forms lateral orbital wall and remarkable portion of floor of the orbit. The prominence of this bone makes it more vulnerable for it to get injuries. It accounts for second most common mid face fractures next to nasal bone and 13% of all craniofacial fractures. Etiologies being road traffic accidents, assaults, animal attacks, fall, and so on, frequency of each varies from one country to another world-wide. Displaced fractures will lead to disturbance in vision, with restriction of eye mobility, compression of the coronoid leading trismus, deranged occlusion, and so on leading to functional and esthetic deformity. A timely and planned intervention is essential for functional and esthetic outcome, as camouflage surgeries have suboptimal results as compared to surgeries done within 2 weeks of injury. Appropriate exposure and mobilization of the fracture fragments are essential for pertinent anatomical and functional reduction. Management of ZMC fractures cause a frequent challenge as there are many literatures supporting 1-point, 2-point, and 3-point fixation.
The aim of this study was to analyze the parameters namely, type of fracture, type of incisions used, treatment methods, and complications occurred in our case series.
Materials and Methods
A descriptive retrospective hospital-based study was carried out in patients suffering from craniomaxillofacial injury which were treated in Aaraikye super-specialty hospital, Davangere, over the period of 3 years (2017-2020) were included. Craniofacial maxillofacial trauma patient’s medical records were collected and out which only the zygomatic complex (ZMC) fractures cases were reviewed. Parameters such as etiology, site of the ZMC fracture, type of fracture, associated injuries, clinical findings, treated with conservative or surgical intervention, type of incisions used, number of fixation used, and any complications encountered were reviewed and analyzed. Bilateral ZMC fractures were considered as separate fractures. All ZMC fractures are classified according to Zing et al. 2 The information was collected from the medical records, computed tomography (CT) findings. Follow-up was established post- 1 year operatively. Any complications if occurred were recorded till the last day of follow-up. Since it is a retrospective study, no ethical clearance was taken for the study.
Results
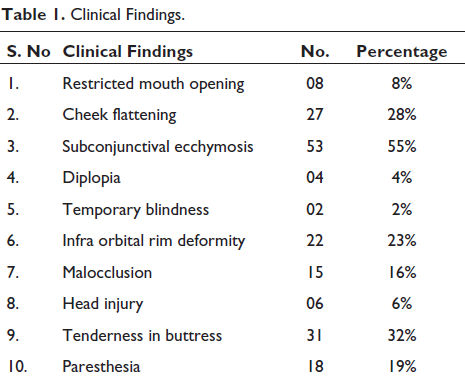
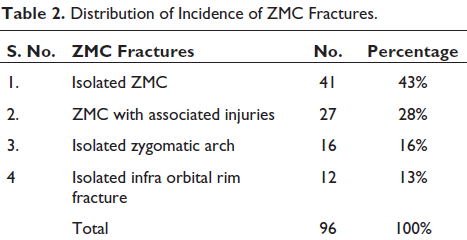
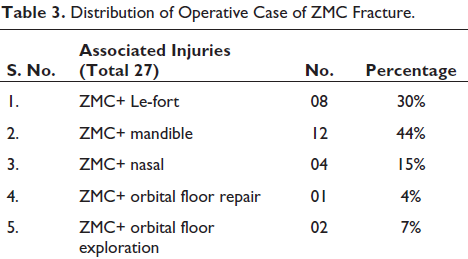
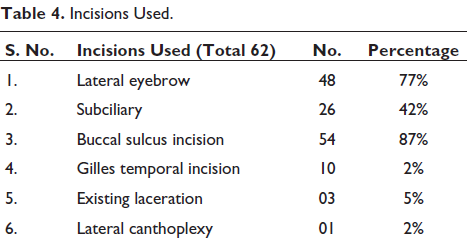
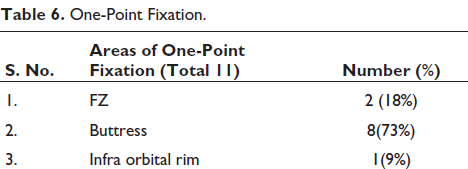
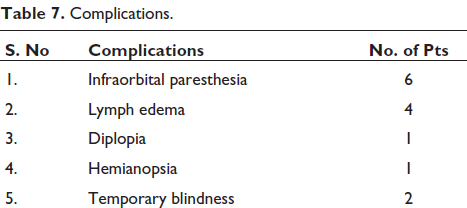
In the course of 4 years (2017-2021) we found 428 patients had craniofacial injury out of which 96 patients were ZMC fractures, out of which 73% were males and 27% were females with age range from 16 to 68 years. Road traffic accidents (85%) account as the most common etiology followed by assault (14%) and animal attack (bear maul injury) (1%). All patients had preoperative CT scans. Subconjunctival ecchymosis (55%) was the most common clinical findings, cheek flattening (28%) second, next was tenderness in buttress (32%), and also infra orbital rim deformity (23%) presented in our cases (Table 1). Table 2 illustrates the distribution of incidence of ZMC fractures, which reveals that isolated ZMC fractures were most prevalent (43%) in our cases. ZMC fractures associated with other fractures have been categorized in Table 3. ZMC fracture along with mandible fracture was mainly associated with bone (44%). Table 4 shows various approaches used for exposure of the fracture fragments. Buccal sulcus incision (87%) and lateral eyebrow incision (77%) was most commonly used. Table 5 illustrates the treatment modality; 2-point fixation (26%) was sufficed in majority of cases. One-point fixation was used in 11% cases of which 73% were fixed on the buttress as shown in Table 6. Table 7 illustrates complications encountered in our series. Figures 1 to 8 illustrate the case performed.
Clinical Findings.
Distribution of Incidence of ZMC Fractures.
Distribution of Operative Case of ZMC Fracture.
Incisions Used.
Treatment Modality.
One-Point Fixation.
Complications.
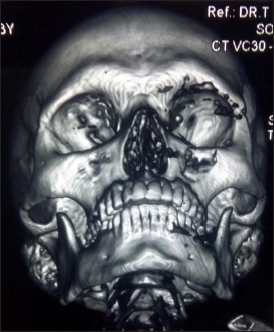
Scalp Avulsion With Lateral Displacement of ZMC.

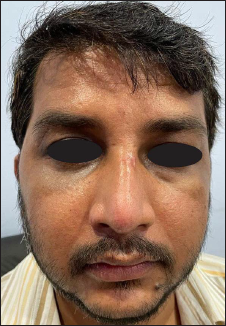
Clinical Features with Vertical Dystopia and Subconjunctival Ecchymosis.

Isolated Left ZMC Fracture.
ZMC Fracture Along with Other Bone Involvement.

Titanium Mesh Placement at Floor of Orbit

Two Point Fixation.

Post Op Subciliary and Lateral Eyebrow Incision on Right Side.
Post Op Edema in Infra Orbital Rim Incision.

Discussion
The architectural frame of zygomatic bone makes it possible to withstand impacts of greater forces without giving away. When the impact is too high it gets separated from the adjacent bones or nearby suture lines leading to ZMC fractures. Depending on the velocity of impact they are seen as isolated or in association with other facial fractures because of the complex anatomy of the midface. Restoration and maintenance of preinjury facial skeletal configuration should be the main moto for treating ZMC fractures. Effective and successful repair needs accurate diagnosis and precise surgical exposure and reduction to fabricate the complex 3-dimensional anatomy. This article provides an overview of the epidemiology, aetiology, presentation, and management of surgically treated cases of ZMC fractures at our major trauma center over a period of 3 years.
ZMC fractures were more common in males than females; our result suggest that males are more active in outward activities and any substance intoxication. The most common cause of injury in our series was road traffic accidents in India, in accordance with Patil et al 4 ; probably urbanization, not wearing protective gears, and alcohol abuse are the main reasons for the maxillofacial injury, mainly in developing countries as ours. Study conducted by Shapiro et al 5 concluded that incidence of morbidity and mortality, and frequency and severity of facial fractures have reduced after the use of protective devices such as helmet and seat belts. Animal attack by Bear was observed in one of our cases where an elderly women working in the field was attacked, leading to avulsion of scalp from forehead to occipital region causing lateral displacement of ZMC. Assault was second most common cause in our series, mainly seen in developed countries as disclosed in an analysis of Polish literature. 6 Falls, sports-related injuries, civilian warfare, and industrial and work related accidents were less common incidences which are the other causes for injuries. Etiology and incidence of ZMC fractures vary in severity, velocity of impact, type and cause depending on the socioeconomical, cultural, and environmental factors among the studied population and vary from country to another and even within the same country. 7 We are unable to comment on the significance of illicit drug use or alcohol use relating to injury due to inadequate documentation in the patient’s files.
The most common symptom in ZMC fractures was tear in the periosteum leading to subconjunctival ecchymosis (55%), tenderness in the buttress (32%), cheek flattening (28%), infra orbital rim deformity (23%), which was in accordance with other studies. 4 Head injury was seen in 6% of our cases; those having Glasgow Coma Scale (GCS) of less than 8 were held till the GCS improved and then they were treated for ZMC fractures. Temporary blindness was seen in 2% of cases which had frontal bone fracture along with Lefort II fracture; the vision was regained after about 6 months on steroid therapy. The infraorbital nerve involvement incidence was 69.6%. 8 In our study nerve involvement was seen in 16% of cases suggesting that the fracture line had crossed the infraorbital canal, which regained after about approximately 6 months. Diplopia was observed in 4% of case series which had orbital rim fracture or orbital floor fracture leading to entrapment of muscle. Exploration with release of the muscle and reducing the fracture and fixing the orbital rim addressed the issue.
Isolated ZMC fractures were observed in 43% of cases, predominantly tripod type of fracture as shown as 57% by Zingg et al, 2 54.35% by Ashwin et al, 8 and 28% of our cases were associated with other craniofacial bones of which 44% were along with mandible. This shows the intensity of impact of the injury.
Treatment modalities are influenced by various factors such as age of the patient, time of presentation, function loss, finances, esthetic concern, and any associated systemic diseases. The amount of degree of displacement, esthetic and functional deficit are the main deciding factors for the treatment of ZMC fractures. Hence, management may vary from simple observation for resolving oedema, diplopia, and paresthesia to very aggressive open reduction and internal fixation. The fractures of ZMC can be isolated, un-displaced, or single in low impact injury or can be rotated, displaced at one or more points around horizontal or vertical axis as seen in medium or heavy impact injuries leading to comminuted or dislocated unfavorable fracture. By assessing the status of the normal articulation of the ZMC with the craniofacial skeleton on CT we can check the amount of displacement of bones.
According to Edward et al, a general rule for minimally displaced or non-displaced fracture are usually treated conservatively and followed up regularly to check for any displacement at later intervals. 9 Closed reduction was considered in 16% of isolated zygomatic arch fractures, through indirect reduction using Gilles lift. Patients were asked to restrain from any untoward force on the side of reduction for at least 3 months. This was similar to a study in which 26 fractures of isolated arch fractures were managed by closed reduction. 10 Rotation or late displacement was not encountered in any of our cases during follow up. Carrol-Girard screw was used by Uda et al for closed reduction and internal fixation. 11
A criteria for selection of patients with surgical intervention of ZMC fractures was proposed by Pozatek et al. 12 Out of 96 cases in our series 64% were treated with open reduction and internal fixation. This was in accordance with Bradely et al. 10 ORIF was chosen by 81% of plastic surgeons, ENT, and 1600 OMFS according to the survey.28 ORIF was preferred in 84% of patients in a retrospective study of 210 cases of ZMC fractures while 16% as closed reduction. 7 Exposure for open reduction and internal fixation utilizes various approaches such as coronal, lateral eyebrow, upper eyelid, transconjunctival, subtarsal, and subciliary lower eyelid; and maxillary vestibular approaches have been well described in the literature. 13 With aesthetic and functional restoration of both face and orbit as the main aim of reducing zygomatic fractures, lateral eyebrow incision, subciliary incision, and intraoral vestibular incision were most commonly utilized for surgical exposure in our study. As for the zygomatic arch, Gillies temporal approach was preferred. These approaches provided best result with minimal complications such as pain and palpability of implants.
Buccal sulcus incision (87%) was most commonly used for the exposure of the fracture, which provides a stable zygomatic buttress without an external scar formation, other incisions being subciliary (42%) for exposure of infraorbital rim, lateral eyebrow (77%) for FZ area, and existing laceration (5%). No significant difference was found in the incidence of ectropion and entropion between subciliary and transconjunctival incisions in a study conducted by Momeni Roochi et al. 14 Waheed El-Anwar et al compared transconjunctival and subciliary approaches and found that lateral canthotomy was mostly needed in transconjunctival incision; transient postoperative edema was present with these cases and postoperative ectropion and sclera show were detected more with subciliary. 15 Subciliary incision has the disadvantage of causing transient ectropion formation; however, it can be prevented by preserving the preseptal portion of orbicularis oculi muscle. None of cases in our series experienced ectropion.
There are significant researches on efficacy of 1-point fixation, 2-point fixation, and 3-point fixation. To achieve an acceptable reduction not every articulation needs to be addressed; however, at least 1, 2, or 3 articulations out of 4 must be addressed intra operatively to reduce these fractured segments accurately. 8 Kim et al studied 29 patients who underwent 1-point fixation at zygomatic buttress and verified with 3D CT scan and found out that 1-point fixation at zygomatic buttress provides enough stability of ZMC without comminuted fractures of lateral orbital rim. 16 Theoretically single plate will stabilize the fractured segment for rotation and translation in the 2 axis perpendicular to the plane of the plate. In our series 73% of cases were fixed only in the buttress region, 18% in frontozygomatic, and 9% in infra orbital rim region depending on the degree of displacement. None of the cases had any degree of rotation or translation post operatively.
In this study, 2-point fixation (26%) of the ZMC at the frontozygomatic and the zygomatic buttress region was advocated after all the 3 points were exposed and evaluated for reduction of the fractured segments at the frontozygomatic, infraorbital, sphenozygomatic suture, and zygomatic buttress region. The zygomatic buttress and frontozygomatic are favored for rigid internal fixation because of the stability provided against rotation and correct alignment to pretraumatic state respectively as this approach has an esthetic outcome with scars well hidden within the eyebrow and intra orally and also preventing the problems of ectropion and neurological disturbance associate with infraorbital exploration. Chakranarayan A et 17 conducted a study on efficacy of 2-point fixation for treatment of ZMC fractures and found a stable fixation and immobilization of isolated ZMC fractures. Mittal et al in their study on pre and post operative values on vertical dystopia and malar height discrepancy showed a statistically significant increase in clinical parameters post operatively and concludes that 2-point fixation provides a stable fixation. 18 In our trauma center 2-point fixation was maximally used in 3 years. Acquiring an informed consent for performing infraorbital approach for reducing and fixing was bit tiresome as they were not prepared for scar below the eye as most of the patients were in young age group.
A systematic review of 2-point vs 3-point fixation revealed that 3-point fixation can be used as a standard treatment modality in effective management of ZMC fractures. 19 Widodo et al (2021) compared 2-point and 3-point fixation and found out that 3-point fixation had better outcome in the assessment of enophthalmos, vertical dystopia, malar height, malar projection, and maintaining postoperatively stability. 20 Surgical outcome was evaluated and compared with CT scans in 2- and 3-point fixation in 2 groups and found no significant difference in stability and they concluded that 2-point fixation was as good as 3-point fixation with respect to stability of fractures. 21 This was similar to the observation in the study conducted by Latif et al and found that post operative outcome relatively had the same mean values at 1 week, 3 week, and 6 weeks postoperatively compared with 2-point fixation. 22 Postoperatively follow up of minimum of 6 weeks is primarily important in achieving functional stability and appropriate esthetics. 23 Three-point fixation was performed in 23% of our case series effectively and were followed up for at least 1 year.
Orbital floor exploration was done in 2 cases and orbital repair in one case where there was a diplopia as presenting symptom along with ZMC fracture; once explored through subciliary incision and entrapment was released the symptoms were reduced and floor repair was carried out with titanium mesh. Post operatively patients were relived of complaints.
To enumerate the complications there were infra orbital paresthesia which was encountered in about 6 patients in our series which almost took 6 months to get into normalcy; this may be due muscle entrapment/manipulations of nerve during the reduction or pre-injury. Ashwin et 8 reported 16 patients with persistent infra orbital nerve paresthesia for 6 months follow up. Crosara et al compared the esthetic outcome of using subciliary, subtarsal, and infra orbital incisions for orbital rim and floor fracture and suggested the superiority of the subciliary and subtarsal incisions over infraorbital incision, since noticeable scars were seen in infra orbital incision then subciliary and subtarsal incisions and all 3 incisions had no statistically significant difference in ectropion, scleral show, or chronic edema rates. They also suggested use of a stepped skin-muscle flap or any other preventive measure, in order to prevent vertical shortening of the lower eyelid. 24 Lymphedema was seen in 4 patients, 3 cases with lateral extension of subciliary incision was used and 1 with existing laceration at the infra orbital region. It was observed during third post operative day and regressed almost after 8 days post operatively. Diplopia was seen in 1 of our patients which subsided by giving steroids for 15 days. Hemianopsia was seen in one of our patients who had suffered head injury and had recovered. Hemianopsia is a condition where lateral side of the vision is blurred. Opthamologist managed medically and the condition recovered after about 5 months. Temporary blindness was found in 2 of our cases where methyl prednisone 1 mg for 15 days was prescribed and slowly tapered for 15 days and patient recovered from the condition.
Retrospective study in our series clearly signifies that 2-point fixation as a first choice in managing ZMC fractures. Zygomatic buttress and fronto-zygomatic region are highly endorsed for fractures with moderate displacement. Drawback of this study was that there was no emphasis on the biomechanics for 2-point fixation.
Conclusion
The ultimate goal of treating ZMC fractures begins with accurate and precise diagnosis formulating a treatment plan that lays emphasis on proper reduction of bony segments and to restore facial form and aesthetics. A beneficial treatment plan within 2 weeks of injury will lead to accurate anatomic reduction and precise fixation. On the basis of our experience and the data from our study, various methods have been successfully followed to treat ZMC fracture and conclude that ZMC fractures rely mainly on the characteristic degree of displacement along with eye involvement and functional impairment, and open reduction and internal fixation along titanium miniplates serve as absolute reliable entity in providing 3-dimensional stability. Stable fixation can be achieved when fixation was done at fronto-zygomatic region and zygomatic buttress in isolated ZMC fractures. There is ongoing lack of consensus in aspects with regards to locations and number of fixation points used, orbital floor repair and exploration, surgeon’s training background, their experience, availability of resources, and preferences play a major role in contributing and maintaining the variety of surgical approaches to ZMC fractures. Nevertheless, further studies should be conducted to assess uniform parameters with bigger sample size, and research should also be conducted to guide the law and impose strict traffic legislation to help and prevent such accidents.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Necessary ethical clearances and informed consent was received and obtained respectively before initiating the study from all participants.