
Abstract
Hereditary gingival fibromatosis is a rare genetic disorder, also known as congenital familial fibromatosis or idiopathic fibromatosis. It may show as an isolated disease entity and is transmitted as an autosomal dominant trait. Hereditary gingival fibromatosis (HGF) may present as severe generalized and progressive gingival overgrowth involving attached gingiva, marginal gingiva, and interdental papilla. The conservative treatment includes removal of dental plaque and eliminating gingival inflammation. Surgically, it can be removed by gingivectomy.
Introduction
Hereditary gingival fibromatosis (HGF) is a gingival disease of genetic origin which is an uncommon condition and is characterized by benign, slow progressive, nonhemorrhagic, fibrous enlargement involving maxillary and mandibular gingiva.1-3 Other names for HGF are elephantiasis, congenital familial fibromatosis, and idiopathic fibromatosis. 4
It is an inherited autosomal dominant trait which does not exhibit until after eruption of permanent teeth and is commonly associated with permanent teeth. 5 This enlargement may interfere with mastication and lip closure causing difficulty in speech, and it may also cause diastema, teeth displacement, and retention of primary teeth. The hyperplastic gingiva appears firm and pink with exaggerated stippling.6, 7
It exists as an isolated abnormality which could be associated with multisystem syndromes such as Zimmermann-Laband syndrome, 8 Jones syndrome, 9 Ramon syndrome, 10 Juvenile hyaline fibromatosis, 11 and systemic infantile hyalinosis. 12
The pathogenesis for gingival fibromatosis (GF) is not very well known. Research consider that the pathogenesis is confined to the fibroblasts in gingiva. A considerable number of articles support an increase of fibroblasts in GF. 13 Decreased apoptosis along with increased proliferative activity in fibroblasts may contribute to fibrotic overgrowth of gingiva. 14 According to some studies, correlation between the amount of fibroblasts and collagen in all GF types is still controversial. Impaired production and degradation of collagen may also contribute to the disease. Studies at molecular level show abnormal expression of few molecules related to extracellular matrix metabolism, for example, transforming growth factor-β, which leads to increased extracellular matrix deposition that contributes to the pathogenesis. 15
With the development of molecular genetics, GF has been linked to the chromosome 2p21-p22 and 5q13-q22. A maturation in Son of Sevenless 1 (SOS-1) gene has been identified, which may be responsible for isolated GF. 16 Lately, a locus for autosomal dominant HGF has been indicated on chromosome. 4 According to the research, there are 2 separate loci present on the chromosome for this condition. 17
Histopathologically, the lesion shows hyperplasis of the epithelium with elongated rete ridges extending into the underlying dense connective tissue. 18 The connective tissue consists of increase in collagen with few fibroblasts and blood vessels. 17
This report presents the clinical features and the management of 40-year-old female with a HGF.
Case Report
A 40 years old female reported to the Department of Periodontics, Career Postgraduate Institute of Dental Sciences and Hospital, Lucknow, Uttar Pradesh with a chief complain of gingival swelling in the left lower posterior region of jaw since 1 year. The patient reported that the gingival enlargement was smaller in size earlier and increased gradually. The patient gave medical history of thyroid and was on the homeopathy medication for the same. There was no family history of GF.
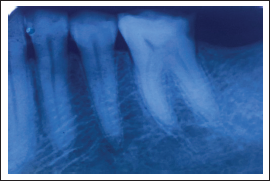
The intraoral examination revealed localized gingival overgrowth in the left mandibular first molar extending into the vestibular area which was pink, leathery consistency, and hard on palpation. The positions of teeth were not hampered with the swelling. The panoramic radiograph revealed normal bone height and tooth positioning. Routine blood investigations were done and values were found within normal range.
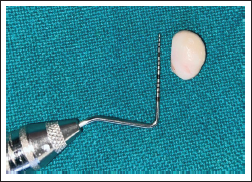
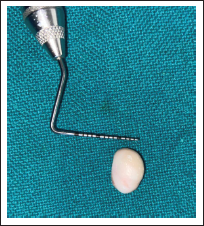
After administering local anesthesia (2% lignocaine hydrochloride with 1:80,000 epinephrine), external bevel gingivectomy with scalpel was performed to remove the growth in the mandibular arch. The excised tissue was 5 mm in length and 10 mm in width. The tissue was sent for biopsy for histopathological examination to confirm the diagnosis. Periodontal dressing was applied (Figures 1–5).
Gingival Overgrowth i.r.t. 36.

IOPAR i.r.t. 36.
Excision of the Overgrowth With Scalpel.

10-mm Width of the Excised Tissue.
5-mm Length of the Excised Tissue.
The patient was advised to rinse the mouth with 0.2% chlorhexidine gluconate for 2 weeks and asked to take analgesics (ibuprofen 400 mg twice daily for 5 days) and antibiotic (amoxicillin 500 mg thrice daily for 5 days) along with B-complex vitamins. Oral hygiene and postoperative instructions were given.
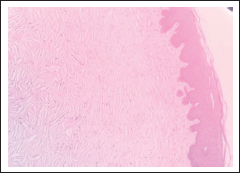
The histological evaluation revealed dense collagenous connective tissue with collagen bundles arranged in irregular manner. The connective tissue was avascular with minimal inflammatory cells infiltrate. The overlying epithelium was hyperplastic with enlarged rete ridges. The histopathological picture was suggestive of GF (Figure 6).
Histopathological Picture.
Postsurgical healing was uneventful. The patient was recalled after 1 week and periodontal dressing was removed and the area was irrigated with Betadine and normal saline. The patient was on follow-up for postsurgical evaluation. The patient was satisfied with the result.
Discussion
Enlargement of gingival tissue is a common feature of gingival disease. GF can be an isolated entity or part of a syndrome or chromosomal abnormality. 2 The genetic mechanism is not fully understood, therefore majority of research have accredited this condition related with hereditary factors. 19 Gingival enlargement can also be drug-induced, or caused by local factors like plaque and calculus, and associated with systemic factors, neoplastic, or idiopathic.
However, the present case can be considered of HGF not exhibiting any signs or symptoms relating to any syndrome. It was diagnosed on the basis of clinical presentation, family history, and histopathological features. In the present case, the patient reported that the gingival enlargement was smaller in size earlier and increased gradually and it did not affect the alignment of the teeth. Patient didn’t have any difficulty in speech and mastication. Also there was no association of plaque and calculus. The microscopic features of the present case were classic of GF. The tissue showed excess amount of collagen in an avascular corium with overlying parakeratinized epithelium. 7
Case reports by Majumder et al. 20 and Martelli-Junior et al. 21 have also performed treatment, where there was no periodontal destruction. The treatment included oral prophylaxis with 0.12% chlorhexidine mouthwash twice/day for 2 weeks, and external bevel gingivectomy with follow-up schedule. Others used fluoride gel to relieve dentinal hypersensitivity.
There are contradictory evidence in literature regarding the cellular and molecular mechanisms that led to GF. Some authors have reported an increase in the proliferation of gingival fibroblasts; whereas others have reported slower than normal growth. 22
HGF is generally associated with syndromic conditions, but in the present case, based on a thorough evaluation of the patient there was no association of HGF with any of the syndromes. Therefore, gingivectomy under local anesthesia was choice of treatment in the mandibular arch.
Conclusion
Keratinized gingival tissues overgrowth is a common condition and is described under variety of names. These enlargements can be caused by medications, hereditary, or local irritating factors. The present case exhibited the clinical features of a typical HGF which was treated with gingivectomy. Removal of hyperplastic gingival tissue eradicates difficulties in eating and speaking and also maintains oral hygiene. It also leads to aesthetic improvements. For diagnosis of recurrence, frequent recall visits and good oral hygiene maintenance are required.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Necessary ethical clearances and informed consent was received and obtained respectively before initiating the study from all participants.