
Abstract
Introduction
The management of facial trauma is one of the most challenging aspects for maxillofacial surgeons. The prominent position and configuration of the mandible make it one of the most frequent facial bones to be fractured. Open reduction and internal fixation are the preferred treatment methods for mandibular fractures.
Objective
To compare the effect of three-dimensional (3D) plates and conventional miniplates for internal fixation of anterior mandibular fractures.
Material and Method
This was a controlled and randomized clinical trial. A total of 14 patients aged between 21 and 50 years, who had symphyseal or parasymphyseal mandibular fractures, were randomly selected for this study from the outpatient clinic of the Oral and Maxillofacial Surgery Department. In this study, open reduction and internal fixation were performed for mandibular symphyseal and parasymphyseal region fractures using 3D plates in 7 patients as the study group and miniplates in 7 patients as the control group. Patients were followed for a period of 3 months at the interval of 1 week, 2 weeks, 4 weeks, 8 weeks, and 3 months for wound dehiscence, infection segmental mobility, postoperative occlusion, significant postoperative complications, and radiological evaluation of reduction, and fixation was done with a postoperative orthopantamogram (OPG) and 6 months postop computed tomography scan.
Result
There was no statistical difference between the 2 groups regarding pain, sensory response, operating time, occlusion, postoperative infection, wound dehiscence, mobility of fracture segment, and bone healing.
Introduction
Several treatment modalities for the treatment of mandibular fractures have evolved significantly over the period of time. From the time of Hippocrates, different techniques for treating mandibular fractures have evolved, the principle of which has always been the same conventional repositioning and immobilization of the bony fragments. However, during the past 50 years, advancement in the fields of anesthetics and radiography, introduction of antibiotics, specially designed instruments, and advances in biomaterials have allowed maxillofacial surgeons to improve outcomes of the treatment of mandibular fractures while reducing morbidity.1, 2
Traffic accidents, violence, sports accidents, and so on have had an alarming increase in the past few decades and is a cause of grave concern. Maxillofacial trauma is very common in all these unforeseen events and the unique position of the mandible on the face makes it vulnerable. It is, therefore, one of the most commonly fractured facial bones. 3 Over the years, the management of trauma has evolved from various forms of splinting to circummandibular wiring, extra oral pins, and semirigid fixation with transosseus wiring followed by rigid fixation technique, which has lately given way to semirigid fixation with miniplate (Champy et al). The currently used conventional miniplate techniques require maxillomandibular fixation for a short period and are unable to render three-dimensional (3D) stability at fracture site.
The treatment of symphyseal and parasymphyseal mandibular fractures has evolved significantly over the past few years. Historically, mandibular fractures were treated with closed reduction with indirect fixation and in case it involved open reduction, fixation used to be done with wire osteosynthesis. Wire osteosynthesis was subsequently supplanted by open reduction and internal fixation with titanium hardware including lag screws and plates as the preferred treatment of fractures. The approach to rigid plate fixation has likewise been modified with progressively smaller plates and less reliance on compression in the treatment of these fractures. The work of Champy and others has allowed for reliable fixation along lines of osteosynthesis through transoral approaches. 4 Champy’s method of semirigid fixation uses easily bendable mono cortical miniplate along an “ideal osteosynthesis line.” The developing forces are neutralized by masticatory force that produces a natural strain of compression along the lower border of the mandible. Both the techniques are associated with disadvantages, of which semirigid fixation is a doubt whether this fixation is sufficiently stable for fractures that cannot be adequately reduced.5, 6, 7
The 3D miniplates consist of 2-hole miniplates with a gap, which are interconnected by vertical cross struts. 3D titanium plates and screws were developed and were reported first by Farmand and Dupoirieux.5-7 Unlike compression and reconstruction plates, their stability is not derived from the thickness of the plate. In the combination with the screws monocortically or bicortically fixed to outer cortical plate, the rectangular plates form a cuboid, which possesses 3D stability. The 3D plating system is based upon the principle of obtaining support through geometrically stable configuration. The quadrangle geometry of plates assures good stability in 3 dimensions of the fracture site because it offers good resistance against torque forces.
The proposed biomechanical and technical advantages of 3D miniplate systems over 2D miniplates system triggered interest for validating the facts, and hence, the current study to compare the efficacy of the 3D and 2D miniplates as a viable treatment modality in the osteosynthesis of mandibular parasymphysis and symphysis fractures was conducted.
Methodology
14 patients were selected in the age range of 21 to 50 years and were equally divided into 2 groups of 7 patients each. Group A patients received treatment with 3D miniplate and Group B patients received treatment with 2D Champy’s miniplates. The cause of fracture was road traffic accident in 13 patients and fall in 1 patient and region of fracture was found to be symphysis in 1 (7%) patient and parasymphysis in 13 (93%) patients.
A standard intraoral surgical technique was followed in both groups to expose and reduce the fractures. Intraoral vestibular incision was taken from mandibular canine to canine or in some cases from a canine to the first premolar for the ease of exposure depending upon the location of the fracture site, with a number 15 blade or a monopolar cautery tip, and at this point, the time was noted; in some cases, skeletonization of the mental nerve was done after injecting with local anesthesia and a curvellinear incision was given in the anterior subapical mandibular region leaving a height of 5 to 7 mm from the free gingival margin. After incising the mucosa with the help of a number 15 blade, the mentalis muscle was sharply incised in an oblique manner till the bone was encountered; once the bone was visible, care was taken to leave ample amount of muscle for holding deep sutures. Subperiosteal dissection was done and the mentalis muscle was dissected in a subperiosteal plane, retraction of the labial tissues was facilitated by stripping them off the inferior border of the mandible, and the fracture line was completely exposed.
Fixation was done using either 3D 2-mm stainless steel, 4 holes plates (Group A) or a standard miniplate of 2 mm and 2.5 mm stainless steel, 4 holes with gap plates (Group B) using Champy’s principle of osteosynthesis. 3D plates were adapted across the fracture line in such a way that the horizontal crossbars were perpendicular to and the vertical struts were parallel to the fracture line. The time at which the plates were adapted in both groups was noted. In cases with oblique fracture, the plates were placed parallel to the lower border of the mandible. In symphyseal/parasymphyseal fractures, the upper crossbar was placed in subapical position. Champy plates in symphyseal/parasymphyseal fractures, 2 plates, were placed to overcome the torsional forces. About 2.5 mm 4 holes with gap plates were placed at the lower border and 2 mm plates were placed at the upper border, either 2 holes with gap or 4 holes with gap. In the parasymphysis fracture site, 2 plates were placed below the mental foramina. The lower plate was placed first, followed by the plate above, to prevent the development of diathesis at the lower border because of the action of masticatory muscles. In both types of platting, 2.5 × 8 mm or 2.5 × 10 mm stainless steel screws were used to stabilize the plates in the lower border for 2D plates, for 3D plates the sizes of the screws were 2 × 8 mm or 2 × 10 mm, and for the upper border 2 × 6 mm screws were used for both plating system. Drill bits of size 1.5 mm for a screw of 2.0 mm diameter and 2.0 mm for screws of diameter 2.5 mm were used to make holes. The entire process was accomplished under copious irrigation with cooled normal saline and time taken from plate adaptation to last screw placed were recorded.
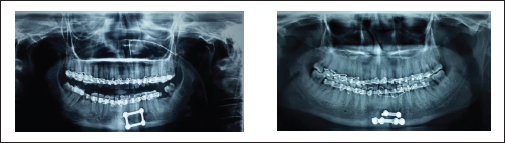
A watertight wound closure was done with resorbable 3.0 vicryl suture, and the total time taken for the surgical procedure, ie, from the time of placement of incision to the last suture placed was noted and a pressure dressing was placed. Soft diet was recommended for 1 to 4 weeks postoperatively depending upon the type of fracture and other associated fractures of the mandible. Patients were followed for a period of 3 months at the intervals of 1 week, 2 weeks, 4 weeks, 8 weeks, and 3 months for wound dehiscence, infection segmental mobility, postoperative occlusion, significant postoperative complications, and radiological evaluation of reduction, and fixation was done with a postoperative orthopantamogram (OPG) and 6 months postop CT scan.
Vestibular Approach (Intraoral)

Exposure of Fracture Line

ORIF Using 3D Miniplate

ORIF Using 2D Plate

Water Tight Closure

Pressure Dressing

OPG Showing Postop Reduction in GROUP A and GROUP B
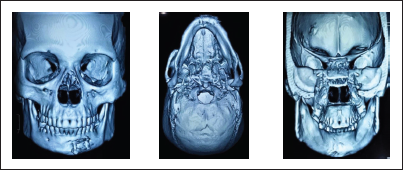
3D CT Face Showing all 3 Cortices of mandible A) Buccal B) Inferior C) lingual
The RUST scale to assess the radiographic union of mandibular fractures was used.
Observations
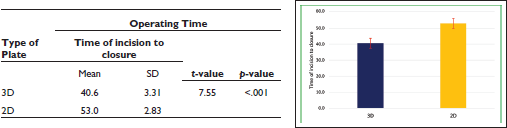
Comparison of Operating Time (Time of Incision to Closure) Status Between the Groups
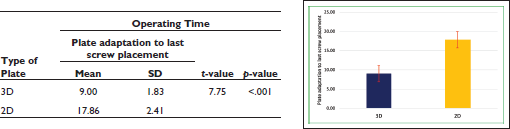
Comparison of Operating Time (Plate Adaptation to Last Screw Placement) Status Between the Groups
Occlusion was achieved in all the cases in both the groups. On comparing the postoperative occlusion that was checked within 24 h postoperatively, it was found that satisfactory occlusion was achieved in all patients in both groups.
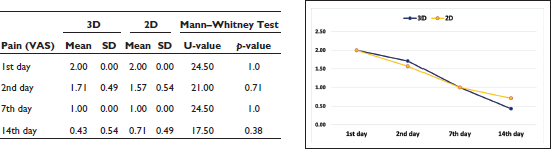
The difference in the VAS score between the groups was not found to be significant (P = .383; Table 3, Graph 3).
Comparison of Pain Status Between the Groups
On comparing the infection status between the groups, it was found that the infection was absent in all the cases of both the groups at the first week, second week, fourth week, and eighth week.
On comparing the wound dehiscence status between the groups, it was found that the wound dehiscence was absent in all the cases of both the groups at the first week, second week, fourth week, and eighth week postoperatively (Table 5, Graph 5).
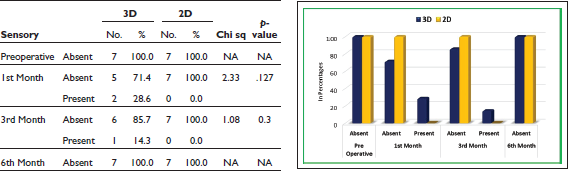
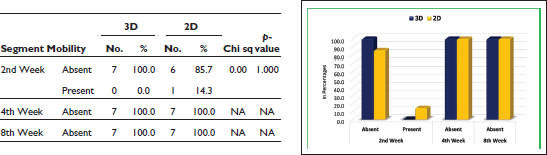
In the sixth month, sensory deficit was absent in all the cases of both the groups (Table 4, Graph 4). The difference in the proportion of segment mobility between the groups was not found to be significant (P = 1.000). It was absent on the fourth and eighth weeks (Table 5, Graph 5).
Comparison of Sensory Status Between the Groups
Comparison of Segment Mobility Status Between the Groups
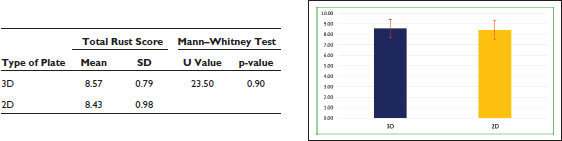
The difference in the total rust score between the groups was not found to be significant (P = .903; Table 6, Graph 6).
Comparison of Total Rust Score Between the Groups
Discussion
Operative Time
On the basis of our observation the cause of such significant difference was because of the fact that Champy’s 2D miniplates are linear plates and 2 plates are required for fixation at parasymphysis or symphysis region because these reasons required higher time. On the other hand, 3D plates are geometrically configured plates that consist of 2 horizontal bars interconnected with 2 vertical bars. So single 3D plate stabilized the fracture both at the superior and inferior border at a time, hence time is saved in plate fixation. In cases of oblique fracture or the fracture running through the mental foramina, more time was required in the placement of a 3D plate. In such cases, the plate was placed either inferior or superior to the foramina, and care was taken while placing the plate superior to the foramina; as the roots of the teeth are present at such place, the screws are placed between the roots. Because of its 3D configuration and bulky shape, it was difficult to place the plate at the fracture passing the mental foramina and, hence, Champy’s plates have advantage over the 3D plates in such cases.
According to the studies by Feledy et al 8 and Zix et al 9 on a 3D plate with similar parameters as our study, reduced average operating time was reported (55 min) for the 3D group.
The evaluation of operative time is a totally operator-dependent parameter. Following the same surgical and instrumentation protocol and given the severity and favorability of the fracture if all these parameters remain the same, the difference in operating time can only depend upon the skill and experience of the operator. We are in no position to evaluate the difference in the operator skills and the efficiency behind all the studies. However, what came to light while comparing 3D and 2D plating groups was that 3D plating takes less time irrespective of the operator, surgical procedure, and severity and favorability of fracture. The difference in all the cases in all studies concluded that 3D plating takes less time than 2D plating and it is supported statistically. Our study is coherent with all studies comparing operating time.
Occlusion
Our study is coherent with the studies done by El Nakeeb et al. 10 With regard to their study postoperatively, no occlusal difference was reported between both the groups, and this is further in agreement with the study of Agrawal et al 11 who reported that no malocclusion was noted in both conventional and 3D miniplates groups.
When compared, the results of our study were coherent with both the above-mentioned studies in terms of occlusion.
Pain
The comparatively high pain score in postoperative day 1 might probably be because of inflammation due to surgical trauma to the tissues for the fixation of both types of plates, but the pain score was showing a positive decrease in all the patients irrespective of whichever group they were from. The cause of this decrease may be because of the aggressive and robust follow-up and maintenance of a good aseptic condition by the surgical team which further helped and benefited other aspects in the process of healing such as the absence of infection and wound dehiscence, which was evident in our study.
Kumar et al 12 in their study found out that the higher pain scores on day 1 were perhaps because of the wide surgical exposure required for adaptation and manipulation of Champy’s miniplate and that more working time is required for the surgical procedure. The higher pain scores on 2 weeks for 2D plate group as compared to 3D plating system were because of higher incidence of infection and mobility at the fractured segments.
The results of all the studies mentioned above with respect to severity of postoperative pain were similar to our study.
Infection
With the use of open reduction and internal fixation, the reported incidence of infection ranged from 3% to 32%. There were many studies that were coherent with this rate, in some cases the infection rate was also found to be 0%. In a study by El Nakeeb et al, 10 none of the patients in both the groups developed infection except one case in 2D plating group which was managed with another course of antibiotics and was totally resolved. Also, Agrawal et al 13 recorded temporary infection in 2 cases and reported that the difference was not statistically significant.
Thus, taking into consideration the small number of patients treated in our study, the infection rate of 0% is very favorable.
Wound Dehiscence
Siddiqui et al 14 in their study on 20 patients of mandibular fractures equally divided into 2 groups (one group treated with 2D and the other with 3D miniplates) reported no case of wound dehiscence postoperatively in any group, which is coherent to our study.
Kumar et al 12 conducted a study where anterior mandibular fractures were treated with 3D and 2D plates and found out the incidence of postoperative wound dehiscence to be equal in both groups with 1 among 10 patients from each group; no studies evaluating wound dehiscence for the 2 plating system produced any statistically significant results.
Our study was found to be coherent with most studies evaluating wound dehiscence.
Sensory Response
Mittal et al 15 in a study of similar interest found the main cause of paresthesia to be either the compression of the nerve by the fractured segments preoperatively or the traction of mental nerve during the manipulation of the fracture segment. This agrees with another study on 3D plates by Guimond et al 16 who found that the main cause of sensory deficit in mandibular angle fractures was the trauma itself.
The results of our study were coherent with most of the studies done to evaluate similar parameters.
Segment Mobility
Farmand17, 18 reported a good stability against traction forces (90 N) and torsion forces (30 N) with 3D plating system.
Wittenberg et al 19 also reported that 3D plating system may provide adequate fixation for mandibular fractures.
In most of the studies comparing the 2 plating systems (3D and 2D), it was found that the 3D plate was considered a better option when considered in terms of stability, but on comparing on the basis of statistical proportions, the difference was not found to be statistically significant.
Bone Healing
Leow et al 20 have made a widely accepted and significant contribution in testing and implementing a reliable and quantifiable score which can be implemented in various clinical and research studies for assessing bone healing through radiographs.
The RUST scale stands for radiographic union scale for tibial fracture; it measures the bone healing after evaluating the appearance of callus and disappearance of fracture line for all the cortices of a long bone. In our study, the long bone was the mandible and the cortices assessed for the score were the buccal, lingual, and inferior cortex. A score was given for a minimum 1 and maximum 3 for each cortex; the highest added score for all the 3 cortices was 9 and bone healing was assessed proportionally to the score, ie, higher the score higher the bone healing. Although the difference did not prove to be statistically significant, it has given us the idea of using a score for evaluating the mandibular bone healing, namely, the RUSM scale, ie, the radiographic union scale in mandibular fractures.
Conclusion
As per the results of our study, the fixation of mandibular fractures with 3D plates provides 3D stability and carries low morbidity and infection rates. The only probable limitation of these plates may be excessive implant material because of the extra vertical bars incorporated for countering the torque forces, and in cases where the fracture line is passing through the mental foramina region there are increased chances of damage to the mental neurovascular bundle if proper care is not taken during the surgical process. However, to reach a definitive conclusion, the study needs to be done on a larger sample.
Footnotes
Statement of Informed Consent and Ethical Approval
Necessary ethical clearances and informed consent was received and obtained respectively before initiating the study from all participants.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.