
Abstract
Frontal bone is fractured following high-velocity injuries such as road traffic injuries or assaults. At times, the intervention can get delayed to avoid grave intracranial injuries resulting in malunion of the fracture which may later become an aesthetic concern to the patient. Many alloplastic materials and autogenous grafts can be used to reconstruct the defect to replace lost and damaged anatomical bone structures, to renew their original function, and at the same time, to restore the aesthetics. We opted to go for an autogenous graft secured with a titanium mesh which gave us a better outcome.
Introduction
The frontal bone is the most frequently fractured cranial bone in craniofacial trauma patients and accounts for 37% of cranial fractures. Isolated Le Fort 1 fractures have significant association with frontal bone fracture. 1 The frontal bone consists of 3 parts, the squamous part which is the largest and forms majority of the forehead, supraorbital margins, and the superciliary arch. The frontal bone is more protected from traumatic events due to the prominence of the nasal pyramid which protects the naso-orbital region as well. It can withstand around 800 to 1,600 pounds of force, thus conferring resistance against most forms of traumatic injury. 2 Most common causes of frontal bone fractures are road traffic accidents followed by physical assaults and sports-related injuries. There are various modalities available for reconstruction of frontal bone defects. We report a case of malunited depressed frontal bone fracture managed with onlay corticocancellous anterior iliac crest graft bone with titanium mesh.
Case Discussion
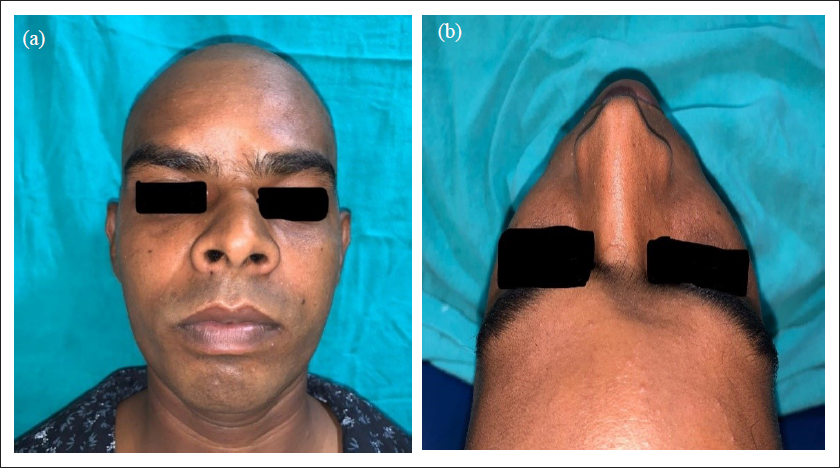
A 35-year-old male patient reported to the outpatient department of the Unit of Oral and Maxillofacial Surgery of our Institute with complaints of depression over forehead for more than 2 months (Figure 1A). He gave history of road traffic accident that took place 2 months back. Patient was admitted under neurosurgery and was treated conservatively without any surgical intervention. His medical history was noncontributory. On examination, he had a defect measuring about 4×3×2 cm over his glabella region without any visible pulsations (Figure 1B).
Preoperative Frontal and Worm’s Eye View Showing Depressed Frontal Bone Fracture.
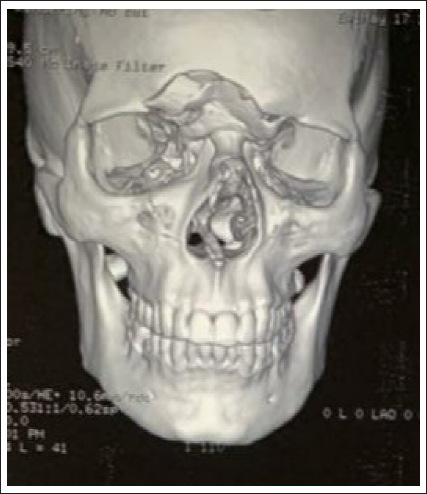
On palpation, it had well-defined smooth margins without any crepitus and tenderness at present. Preoperative computed tomography (CT) was advised and it showed frontal bone fracture with outer table involved (Figure 2). Neurosurgery clearance was done and patient was planned to camouflage the defect with autogenous onlay corticocancellous iliac crest graft stabilized with 1.5 mm titanium mesh under general anesthesia. X-ray pelvis was advised to rule any metabolic previous fracture or osteomyelitis at the donor site.
Preoperative 3D CT Scan Showing Comminuted Frontal Bone Fracture.
Surgical Procedure
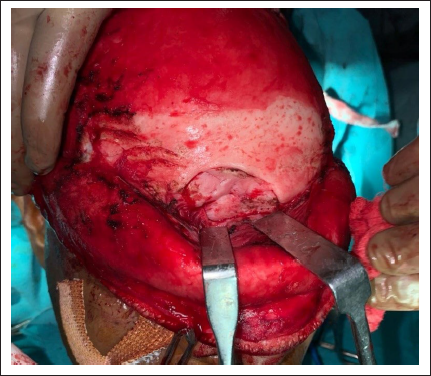
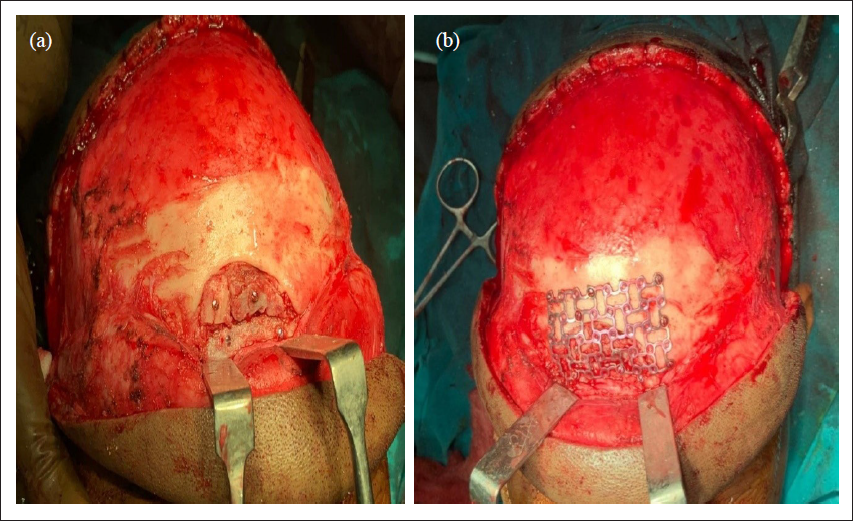
Patient was operated under general anesthesia. After proper scrubbing of operating field and draping, 2% lignocaine with 1:2,00,000 adrenaline was infiltrated in the area to achieve vasoconstriction. Surgical site was exposed through Bicoronal approach (Figure 3). After proper exposure of defect site, it was reconstructed with autogenous iliac crest graft. Anterior corticocancellous iliac graft was harvested by trap door approach technique (Figure 4). The harvested graft was contoured in the defect site and stabilized with 1.5 mm titanium mesh (Figure 5). The surgical site was irrigated and drain was placed and closure done in layers with 3-0 vicryl and 3-0 nylon. Immediate postoperative result was satisfactory. Postoperative 3-month follow-up was satisfactory and uneventful (Figure 6).
Exposure of Fracture Site Through Bicoronal Approach.
Showing Harvesting of Corticocancellous Iliac Crest Graft.

Autogenous Graft Contoured in the Defect Site and Fixed With 1.5 mm Titanium Mesh.
Postoperative 3 Months Follow-up.

Discussion
Cranioplasty is primarily performed for esthetic purposes. Along with esthetic result for patient psychology, cranioplasty decreases the chances of epilepsy as per literature. 3 Ideal waiting period is 3 to 6 months or till 1 year if surgical site is infected. 4 This ensures that the patient is neurologically stable, thus reduces the chances of graft site infection.
Various autografts such as cranium, scapula, fascia, sternum, ileum, tibia, and costochondral grafts are used which are protected previously by boiling in water, 5 autoclaving, freezing, and covering in abdominal fat. Allografts was first used by Morestein in 1915 6 but was not popular due to higher infectivity rates and graft rejection. Nonmetal alloplasts used are celluloids, methyl-methacrylate, hydroxyapatite, polyethylene, silicon, chorale, ceramic, and CortossTM. Titanium, gold, silver, platinum, tantalum and vitallium alloys. Among them titanium is the most biocompatible and widely used.
The ideal properties of cranioplasty materials are as follows
7
:
It must fit the defect and achieve complete closure Radiolucency Resistance to infections Not dilated with heat Strong to biomechanical processes Easy to shape Not expensive Ready to use
Not a single material satisfies all the given criteria.
In our institution, the preferred graft is anterior iliac corticocancellous graft.
The cortical cancellous iliac graft is more porous in nature, more rapidly revascularized but at the same time has more chances to get resorbed. The autografts having higher chances of resorption when combined with alloplastic mesh retains the contour of the bone even in case of complete resorption of autograft, which is the most important advantage of combination of autograft and alloplast.
Technique of harvesting the iliac crest graft is classified as follows
8
:
Trapdoor technique Splitting technique (Wolfe Kawamoto) Window technique Trephine technique
Among these, window technique allows for a stable graft with little quality of manipulation and is generally contoured to fit the desired special defect.
Disadvantage of iliac graft is its porous nature and high vascularity which causes early resorption. 8 Methyl-methacrylate is the most commonly used material for cranioplasties because of its adaptation, good radiates less heat, and adherence to dura with no reaction to underlying layers 9 but it needs structural support to prevent breakage. Hydroxyapatite and chorale increase the bone repair 10 but it is very brittle and needs protection from trauma till osseointegration is complete. Polyethylene easy shapeable build with heat made this material popular.11, 12 CortossTM (Orthovita®) is a new synthetic bone void filler that contains bis-glycidyl-methyl-methacrylate, bisphenol (a polyethylene glycol diether dimethyl acrylate), triethylene glycol dimethyl acrylate monomer, and bioactive glass ceramic. Cortoss has lower rate of inflammation but no direct vascular invasion. Noble metals are outdated because of their high cost, tantalum due to headaches caused by high heat conduction ability. 13 Titanium is hard to shape, but relatively cheaper, bio acceptable, and radiolucent after mixing with other metals. 13
The frontal bone is the most frequently fractured cranial bone in craniofacial trauma patients and accounts for 37% of cranial fractures. Prevalence of frontal bone injuries based on injury mechanism road traffic accident (RTA) (65.1%) being most common, fall (18.8%), sports (4.7), fight (6.04%), work related (1.34%), and other (4%). Motor vehicle accidents are the most common cause followed by assaults and sports-related injuries. Depressed skull fractures are indicated for elevation if the defect is more than 10 mm and in the presence of brain injury. Frontal bone contour defects result in marked facial deformity which becomes an esthetic concern.
Amongst various classifications of frontal bones fractures, 2 most important are as follows
13
:
Based on vertical and horizontal lines Type 1 fractures are isolated to the frontal sinus without a vertical trajectory (34.2%). Type 2 fractures are vertically oriented and extend into the orbit but not the frontal sinus (15.4%). Type 3 fractures are vertically oriented and extend into the frontal sinus but not the orbit (6%). Type 4 fractures are vertically oriented and extend into ipsilateral frontal sinus and orbit (18.8%). Type 5 fractures extend into the frontal sinus and into the orbit on both sides of the face or the contralateral side of the face (25.5%). Based on depth of penetration of fracture line within skull base. Depth A fractures involve the anterior table of the frontal bone with or without posterior table involvement and do not extend into the anterior cranial fossa (9.4%). Depth B fractures involve the floor of the anterior cranial fossa (44.3%). Depth C fractures involve the middle cranial fossa (22.82%). Depth D fractures extend into the posterior cranial fossa (23.49%).
Considering all these options, the anterior corticocancellous iliac crest graft by window technique was considered suitable for the type 5 depth A type of frontal defect with only esthetic concern.
Conclusion
With various treatment modalities available for management of depressed frontal bone fractures, we opted for onlay corticocancellous anterior iliac crest bone graft with titanium mesh, which gave satisfactory postoperative results. Key points to remember are meticulous preoperative planning, neurosurgery consultation, and proper follow-up.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.