
Abstract
Management of airway is the most important concern in critically injured patient with life-threatening injuries for an anesthesiologist as well as primary caregiver as it may distort airway anatomy as well as destabilize the cervical spine. These patients are potentially difficult candidates for mask ventilation and endotracheal intubation. Additionally, these patients are prone to regurgitation as they may have full stomach condition. The requirement of maxillofacial surgery is free access to the oral cavity; thus, securing alternate methods to maintain a safe airway is the primary priority. To improve the clinical outcome of these patients, there should be mutual cooperation between the anesthesiologist, maxillofacial surgeon, and ENT surgeon (for emergency tracheostomy, if needed). In this review, we are discussing primary management in emergency, relevant anatomy, difficulty in securing patent airway, and possible approach for airway management in maxillofacial trauma patients.
Keywords
Introduction
Maxillofacial trauma is big concern for an anesthesiologist due to expected involvement of the airway. Most of the patients presenting with multiple trauma may require coordination between different specialties. The first aim in managing a trauma patient is airway maintenance and cervical spine stability according to advanced trauma life support. Airway management-related problem may lead to grave morbidity and mortality in maxillofacial trauma patient during primary management as well as during elective surgical management. It has been found that failure to secure airway or intubate was the most common cause of patient mortality in facial trauma patients. During airway, management anesthesiologist has to consider the following:
Form of injury and possible involvement of airway Difficult bag and mask ventilation and endotracheal intubation Cervical spine involvement Risk of aspiration of gastric content Bleeding that may occlude view of oral cavity
The time available for deciding our plan and its implementation for securing airway under a particular scenario is short as a patient’s condition can deteriorate quickly.
Relevant Anatomy
The human skull is divided into the following:
Calvaria—enclose and protect the brain Facial skeleton, which is further divided into Upper face (upper one-third)—cranium, frontal bone, and frontozygomatic process Middle face (middle one-third)—maxilla, zygomatic, and ethmoid bone Lower face (lower one-third)—mandible and temporomandibular joint
Classification
Maxillofacial trauma involves bone as well as soft tissue. Bony fracture is classified according to the part of face involved:
Upper face fracture (upper 1/3): Involves frontal bone and sinuses. A total of 33% of these patients may have associated dural tear.
1
Mid facial fracture (mid 1/3): Involves nasal bone, orbital fracture, nasoethmoid, zygomatic arch, and maxilla. Lower face fracture (lower 1/3): Involves mandible fracture (third most common fractured facial bone)
2
which may be unilateral, bilateral, or comminuted. Bilateral and comminuted are unstable while unilateral is relatively stable fracture. Pan facial fracture: Involves upper, mid, as well as lower face.
Le Fort Classification of Maxillary Fracture
Le fort classify patterns of maxillary fracture into the following (Figure 1).
3
Le Fort 1: Horizontal maxillary fracture, separate teeth from the upper face. The fracture line passes through the alveolar ridge, lateral nose, and inferior wall of maxillary sinus. Also known as Guerin fracture. Le Fort 2: Pyramidal fracture, with teeth at the pyramid base, and nasofrontal suture at its apex. Fracture arch passes through the posterior alveolar ridge, lateral wall of maxillary sinus, inferior orbital rim, and nasal bone. The uppermost fracture line can pass through the nasofrontal junction of the frontal process of the maxilla. Le Fort 3: Craniofacial disjunction or “Dish face” deformity.
4
Transverse fracture line passes through nasofrontal suture, maxillofrontal suture, orbital wall, and zygomatic arch/zygomaticofrontal suture. Because of the involvement of the zygomatic arch, there is a risk of the temporalis muscle impingement. Unsurprisingly, type III fractures have the highest rate of cerebrospinal fluid (CSF) leak due to high chance of damage to cribriform plate, skull fracture, and dural tear.
Le Forte Classification of Maxillary Fractures.
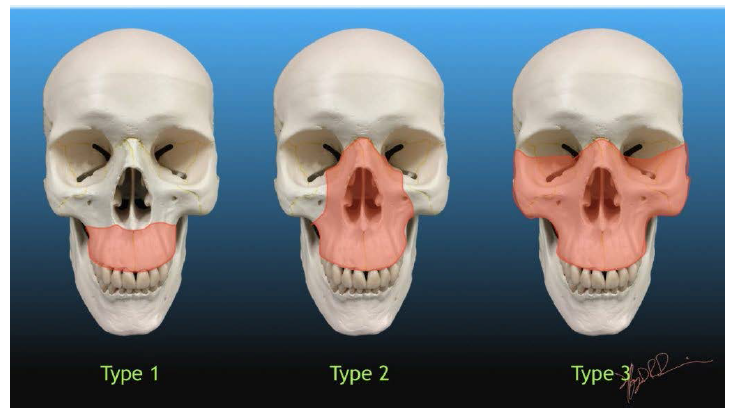
A memory aid is:
Le Fort I is a floating palate (horizontal) Le Fort II is a floating maxilla (pyramidal) Le Fort III is a floating face (transverse)
Any combination is possible. For example, there may be type 2 on one side and contralateral type 3, or there may be unilateral type 1 and 2 fractures. It should be noted that Le Fort fractures are often associated with other facial fractures, neuromuscular injury, and dental avulsions.
Presentation
Edema, subcutaneous emphysema. Mobility and paresthesia of involved region. Le Fort 2 and 3 may present with associated CSF rhinorrhea and epistaxis. Lower 1/3 fracture may cause malocclusion of teeth and airway compromise because of posteroinferior displacement of fractured segment.
Complication
Airway obstruction Cervical spine injury with instability Hemorrhage Esophageal injury Pneumocephalus and pneumomediastinum Subcutaneous emphysema
Maxillofacial Trauma and Airway Injury
According to Hutchison et al,
5
different situations can adversely affect the airway associated with maxillofacial trauma:
Posteroinferior displacement of maxilla may block the nasopharyngeal airway. Bilateral fracture of mandible with fractured symphysis may cause tongue to displace posteriorly and occlude the oropharynx in supine position. Fractured bony segment, teeth, any secretion, or blood or gastric content may occlude airway from anywhere between oropharynx and larynx. Hemorrhage from any wound or nasal bleeding may obstruct the airway. Soft tissue and swelling may cause delayed airway compromise.
Emergency Management
Initial Assessment
All patients should be triage first, and a thorough and fast airway evaluation should be performed. Any life-threatening injury should be identified and managed accordingly on a priority basis. Advanced trauma and life support protocol must be followed for primary survey of patients, which includes,
6
Airway management along with cervical spine stability. Breathing assessment and ensure ventilation. Circulation and hemorrhage control, if any. Disability delineation and neurological status assessment. Expose and shift the patient from harmful environment that may cause secondary injury.
Subsequently, a secondary survey should be conducted to rule out any associated traumatic brain injury as there is significant association between maxillofacial trauma and head injury (25%-37%). 7 For airway management, we cannot apply the same technique to all patients universally. We should be careful for any iatrogenic injury during maintaining airway patency.
Airway Assessment
Verbal response: If a verbal response is present, no airway compromise is suspected. 8
Mouth and pharynx: For any bleeding or foreign body, all debris or secretion or blood should be removed.
Cervical spine: All patients should be suspected for cervical spine injury unless proven. 9 Cervical spine should be stabilized by cervical collar or spine board.
Re-examination of the airway to prevent delayed airway compromise due to soft tissue edema or any blood from an oozing source. 10
A high flow of oxygen should be given to all trauma patients. 11
Airway Management and Related Problems
Maxillofacial injury makes airway management a difficult task due to deranged anatomy, soft tissue edema, hemorrhage, and a possible full stomach condition. In midfacial injury, high chances of hemorrhage may be present due to high vascularity of that region. 12 A patent airway can be maintained by putting patient in lateral position and open mouth by applying pressure on temporomandibular joint so that blood and secretion are allowed to drain out of mouth/oropharynx. A suction with adequate pressure must be arranged. 13 According to DuCanto et al, 14 a soiled airway should be managed by suction-assisted laryngoscopy and airway decontamination approach. In the abovementioned approach, a rigid suction catheter should be placed in esophagus upper part for suction of gastric content contaminating oropharynx while intubating. 14
Sniffing position and head tilt should be avoided in patient with suspected cervical spine injury to prevent any further neurological injury. 10 Chin lift and jaw thrust are not a good option due to distorted anatomy. The oropharyngeal airway should be used with caution as it may induce vomiting or laryngospasm in patient with intact gag reflex which may further deteriorate the patient condition. The nasopharyngeal airway is a better option in such patients but it should not be used in patient with skull base fracture. Preoxygenation must be done in these patients to increase oxygen reserve and prevent hypoxemia during apneic period. 15
Bag mask ventilation should be done along with the help of an assistant,one holding the mask tightly fitted to mouth while other operating the bag. 16 Positive pressure ventilation may further compromise airway as the fractured segment may displace and occlude airway. At the time of securing the airway in difficult airway scenario, patients should have spontaneous ventilation.10, 17
For securing airway, the available options are
Orotracheal intubation Nasotracheal intubation Surgical intervention Cricothyroidotomy (surgical or needle) Tracheostomy (surgical or percutaneous)
If mouth opening is adequate then direct laryngoscopy and orotracheal intubation using rapid sequence intubation and manual inline stabilization are the most preferred and rapid methods. 18 However, in a patient with limited mouth opening, blind or fiberoptic bronchoscope-guided nasotracheal intubation should be performed. For nasotracheal intubation, skull base fracture must be ruled out. McCoy laryngoscope should be used in adequate mouth opening patients as it may improve visualization of laryngeal view with minimal movement of cervical spine.
Airway Management Devices
Indirect View of Vocal Cord
Video Laryngoscope: Glideslope, C-MAC including hyperangulated D blade, King Vision, McGrath, and Airtraq are a few devices for the indirect vision of vocal cord and epiglottis in a patient with disturbed normal anatomy and soft tissue edema. However, these devices are not frequently present in the emergency department. Bullard laryngoscope: It is a rigid fiber optic laryngoscope. Its blade curvature is designed according to the curvature of the oral cavity which allows minimal manipulation of head position or neck movement. For intubation by a Bullard laryngoscope, 6 mm mouth opening is sufficient.
19
Fiber optic bronchoscope: Fiberoptic bronchoscope-guided intubation is a recommended method for difficult intubation, but it is difficult in trauma patients due to noncooperation of patients.
20
Due to presence of blood and secretions in the nasal and oral cavity the local anesthetic gets diluted and therefore inadequate effect may be achieved. Fiber optic bronchoscope with good suction can offer better result.
21
Blind Airway Devices
Supraglottic airway device: Supraglottic airway devices are useful when mask ventilation and intubation both are difficult. Laryngeal mask airway and intubating laryngeal mask airway (ILMA/fast track) can be used. They are useful to ventilate the patient until a definite airway is maintained. ILMA can be used for blind intubation with minimum cervical movement. In second generation devices, LMA ProSeal, i-gel and LMA Supreme are better as they have a separate gastric channel which is helpful in full stomach condition and minimize chances of aspiration. Thus, second generation devices are better than first generation because of the separate gastric and respiratory port.
22
Third generation devices provide the additional benefit of sealing mechanism.
23
Double lumen laryngeal devices (Combitube): Combitube can be used in a prehospital setting even by paramedics even at the site of the incident. It is dual lumen double cuff tube; It is a dual lumen double cuff tube, where the distal tube enters the esophagus & distal cuff is inflated to prevent regurgitation of gastric contents and the proximal cuff is inflated to seal of oropharynx. Perforation is present between these two cuffs which ventilate lungs. Placement of combi tube becomes difficult in distorted anatomy due to injury. Direct laryngoscopy and intubation can be performed even when combi tube is in situ. Some complications that can occur are vocal cord edema, tracheal injury, esophageal injury, and tongue edema.
24
Limitation of Blind Airway Devices
These devices are unable to protect airway from aspiration risk. These devices can displace due to patient movement or patient transportation. Due to trauma patient, mouth opening minimizes and it becomes difficult to use these devices. Thus, we may conclude that these devices can be used only as temporary measures. A definitive airway should be maintained as soon as possible.
Surgical Airway Management
It is a procedure of choice when all other measures fail to secure patent airway.
Cricothyroidotomy
Cricothyroid membrane can be located easily and it is less vascular with low complication rate; thus, it is the site of choice for emergent airway management.
25
Needle cricothyroidotomy: For needle cricothyroidotomy, we have to insert a wide bore cannula (14 gauge) in the trachea through the cricothyroid membrane. Oxygen is delivered by tri way at a high flow rate (12-15 L/min). The inspiration to expiration ratio should be 1:4. Other port of tri way may be used to attach the EtCO2 probe. Oxygen flow should be reduced to 2-4 L/min in upper airway obstruction to avoid barotrauma to lungs. The jet ventilator attached to cannula is the other option which works on the same principle. Some complications of cricothyroidotomy are:
Lung hyperinflation Hypercapnia Subcutaneous emphysema Oxygenation for limited period Surgical cricothyroidotomy: It is the best choice for emergency airway control.
26
According to Difficult Airway Society 2015 in “cannot ventilate and cannot intubate” situation, it is the fastest and most reliable method to secure airway.
27
Scalpel cricothyroidotomy is considered to be better than needle cricothyroidotomy as it allows cuffed endotracheal tube introduction in trachea which is more advantageous in:
Protection from aspiration Allows EtCO2 monitoring Patent route for exhalation Allows intermittent positive-pressure ventilation
Tracheostomy can be performed when patient becomes hemodynamically stable to prevent subglottic stenosis. Tracheostomy is not a good choice for acute management of airway in this scenario as it is time consuming and difficult to perform in the maxillofacial trauma patient. 11
Airway Management in Definitive Surgery
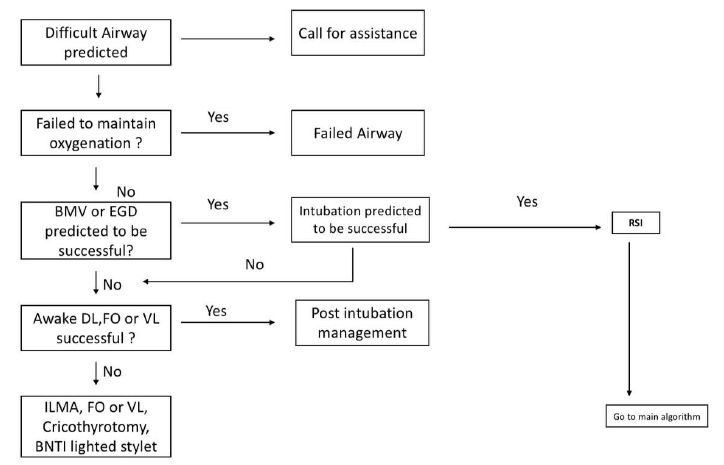
We should go for early definitive management of patient for maxillofacial injury after stabilizing life-threatening condition as delay may result in malunion or other complication (Figure 2).
Preop Evaluation
It includes inspection of:
Mallampati grading Mouth opening Nasal patency Edema and dentition Any neurological abnormality to rule out head injury Radiological investigation to rule out flail chest, cervical spine injury, or head injury Any comorbid condition Relevant investigation according to patient age and general condition
Preop Preparation
An accurate airway management plan should be prepared in maxillofacial trauma patients as there are high chances of complications related to the airway in the perioperative period. A fully equipped trolley for difficult airway cart should be ready including cricothyroidotomy and tracheostomy. A discussion with the surgeon and his team is necessary regarding the route of intubation, surgery, and surgical plan.
Option for Securing Airway
Awake intubation Direct laryngoscopic intubation Videolaryngoscopic intubation Fiber optic-guided intubation Retrograde intubation Surgical airway
Awake Intubation
Upper airway should be anesthetized properly for awake intubation. Awake intubation may be considered in patients with anticipated difficult airway or cervical spine injuries. Upper airway should be adequately anesthetized using local anesthetics & Intubation should be under fiber optic guidance. It should be fiber optic guided or may be blind nasal in restricted mouth opening.
Awake intubation may lead to a limited success rate in blind intubation and may also cause further trauma to the airway.
Intubation after General Anesthesia
It should be considered in uncooperative patients with no restriction of mouth opening. Oral or nasal intubation is preferred on the basis of requirement of surgery. Video laryngoscopy is better than direct laryngoscopy as video laryngoscopy requires minimal manipulation of the neck and better outcome in patients with cervical injury.
Nasal intubation is preferred in maxillofacial trauma patients 29 but it is contraindicated in the basal skull fracture or fracture of the nasal bone.
Option When Oral and Nasal Intubation Not Feasible
Retromolar Intubation
It is indicated when oral and nasal intubation is not a good option as in Le Fort 2 fracture. 30 After orotracheal intubation, tube is pushed toward retromolar space and fixed at the angle of mouth. The patient should be assessed preoperatively for retro molar intubation by asking to close the mouth with his index finger is placed in retro molar space. Retro molar intubation has minimal interference with surgical field. It can also be used in postop ventilation, if required.
Submental Intubation
In this technique, first perform orotracheal intubation by armor tube then make a small incision in submental region little bit medial to lower border of mandible and try to make a narrow tunnel by blunt dissection. Once the tunnel is formed, pull the tube through this tunnel from the oral end and fix the tube with stitches. Submental intubation is not a good option for postoperative elective ventilation. It is not a very good option for maxillofacial trauma patient with restricted mouth opening. 31
Retrograde Intubation
It causes minimal neck manipulation but is not a good option for maxillofacial trauma patients as passing guide wire from trachea to oral or nasal cavity may cause difficulty due to distorted anatomy. 32
Postoperative Management
In postoperative patients of maxillofacial trauma, extubation may be difficult. Extubation should be planned by considering duration of surgery, possible airway edema, maxillomandibular fixation, any comorbidity, preoperative general condition of the patient, and perioperative hemodynamic stability. Extubate patient only after fully awake condition, and following commands. Ensure that the throat pack has been removed before extubation. A nasopharyngeal airway is a good option for airway patency in postoperative patient. A cuff-leak test should be done before extubation if suspecting laryngeal edema. Wirecutter should be present at the bed side of patient in case of any emergency.
Conclusion
A successful airway management in maxillofacial trauma patients requires a skilled anesthesiologist with fully prepared difficult airway cart familiar to anesthesiologist. There should be a good communication between surgeon and anesthesiologist regarding anesthetic plan as well as surgical plan for better outcome of patient. Backup plan should be ready.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Necessary ethical clearances and informed consent was received and obtained respectively before initiating the study from all participants.