
Abstract
Traumatic injuries are commonly happening in pediatric and adolescent age groups of which 20% present with dentoalveolar fractures. The most common cause of which is teeth luxations, intrusive luxations being the most severe form. The timely diagnosis, both clinical and radiological as well as swift treatment goes a long way in maintaining the form and function of the patients oral complex. This case report describes a case of dentoalveolar fracture of anterior maxilla because of intrusive luxation of maxillary anterior teeth, its diagnosis, and management.
Introduction
Traumatic injuries are commonly happening in pediatric and adolescent ages which usually result from accidents, fall from heights, contact sports, violence, etc. The most common type of injury considered as a dental emergency is dentoalveolar fractures. The most common cause is teeth luxations with a prevalence of 15% to 61%. 1 The incidence of trauma for maxillary anterior teeth ranges from 4% to 91%. 2 Traumatic intrusion is a luxation injury where the tooth is axially displaced into the alveolus. Intrusive luxation is more common in deciduous teeth, however, it is considered a rare occurrence in permanent teeth. 3 Intrusion is a severe form of injury and accounts for only 3% of all traumatic injuries in permanent dentition.
Although traumatic dentoalveolar injuries can be diagnosed clinically, a radiographic evidence is still required to confirm the diagnosis and rule out any other associated injuries or facial fractures. As traumatic injuries are a challenge to treat, the correct diagnosis must be made followed by painless prompt treatment and the patient must be kept on a follow-up to assess the success of the treatment. 4
Many case reports have been published describing the treatment of avulsed permanent incisors but the treatment following multiple avulsions/intrusive luxations along with dentoalveolar fractures has been rarely found in the literature. This case report describes the management of anterior maxillary dentoalveolar fracture following traumatic intrusion of maxillary anterior teeth and a review of the literature regarding it.
Case Report
A 9-year-old male patient reported to the Trauma Unit of our Department of Oral and Maxillofacial Surgery in a trauma center, King George Medical University, Lucknow following severe dentoalveolar trauma because of a fall from the height. The parents reported that the child while playing on the terrace of his house fell down from one story height and injured his face leading to the traumatic intrusion of certain teeth and avulsion of a single tooth. Because of unawareness of oral health in villages, the single avulsed tooth was left abandoned on the road while the parents rushed the child to the nearest Primary Health Centre where he was managed conservatively and referred to King George's Medical University, Lucknow. The patient had one episode of vomiting and a history of oral bleeding at the time of the traumatic injury. There was no history of loss of consciousness, seizures, and bleeding from ear and nose.
Preop OPG

Preop picture
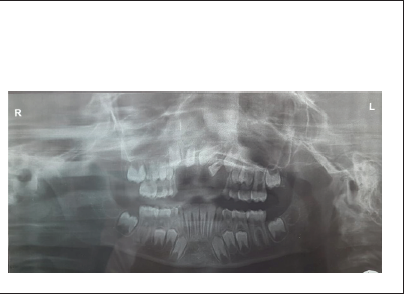
The patient reported to Trauma Centre, King George's Medical University 12 h after the incident where a primary survey was done followed by a CT head to rule out any head injury. After getting clearance from the trauma surgery, neurosurgery, and orthopedic trauma units, the patient was referred to the Trauma OMFS unit where he was examined, evaluated, investigated, and diagnosed as a case of maxillary anterior dentoalveolar fracture with the traumatic intrusion of maxillary central incisors and left lateral incisor (11, 21, 22) with avulsion of the right lateral incisor (12).
On extra-oral examination, the face was apparently symmetrical with diffuse swelling in the upper lip. Mouth opening was restricted because of pain and tenderness on palpation was present with respect to the upper lip region.
Intraoral examination revealed an open maxillary anterior alveolus packed with grime, dirt, pus, and blood clot. The mouth opening was initially restricted because of pain and sutures were present on the lower labial vestibule region. Multiple bruises were also visible on both upper and lower lips. The teeth numbers 12, 11, 21, 22 were not visible in the oral cavity. However, there was a bulge on the labial aspect of the anterior maxilla hinting at the fracture of that dentoalveolar segment with the intrusion of the missing teeth. This was confirmed by an orthopantomogram which showed intruded 11, 21, 22 and an avulsed 12 along with other mixed dentitions.
An informed verbal and written consent was taken from the parents. The parents were informed about the upside, downside, and prognosis of the proposed treatment. The patient was taken to the operating theatre of the Trauma OMFS unit for the treatment under local anesthesia. The mouth rinsing was done with 2% betadine solution before the procedure. Bilateral infraorbital and nasopalatine nerve blocks were given and after adequate anesthesia was achieved the procedure was started. A full-thickness mucoperiosteum flap was raised from 13 to 23 regions along with releasing incisions. It revealed a fractured labial cortex still adhering to the periosteum and intruded 11, 21, and 22. All the grime, dirt, and blood clots were removed by copious irrigation and the teeth were repositioned in their correct places and arch form. The labial cortex, which was viable because of its adherence to the periosteum, was replaced over the repositioned teeth and helped in place by suturing of the mucoperiosteum to the palatal gingiva via vertical mattress sutures.
Immediate Postop Picture

The teeth were secured in their corrected places by composite resin and wire splinting technique.
Oral hygiene instructions were given to the patient and his parents and a chlorohexidine mouthwash was given for rinsing. Amoxicillin with clavulanic acid (375 mg t.i.d.), combiflam (250 mg b.d.), vitamin b complex (1 cap o.d.) was prescribed as discharge medicine. The patient was advised to take a soft diet for 2 weeks.
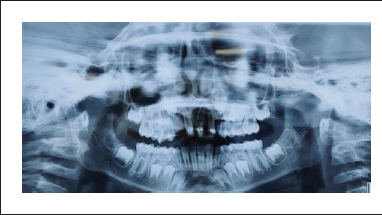
1-month follow-up OPG
2-month follow-up OPG
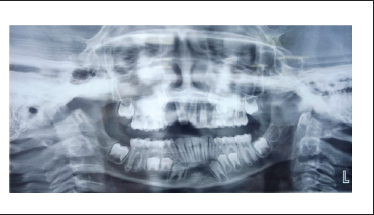
After 7 days, satisfactory postoperative healing was seen on follow-up and the sutures were removed. The patient was followed for 2, 4, and 8 weeks. After 4 weeks, the splint was removed as per the Guidelines of the International Association of Dental Traumatology (Revised in June 2020) 5 and the American Associations of Endodontists. 6 Teeth numbers 11, 21, 22 were asymptomatic clinically as well as radiographically with intact lamina dura and the patient was advised to revisit in case he felt any discomfort of any sort.
Discussion
Trauma to a child can be emotional to him/her as well as increases their and the parent’s apprehension toward its treatment. However, extensive trauma to dentoalveolar parts requires prompt intervention and treatment to secure the child’s physical and emotional integrity. 7 The usually encountered dental emergency is dentoalveolar fractures. Dentoalveolar injuries are quite frequently associated with facial fractures, with studies showing that about 20% of patients with facial fractures also have dentoalveolar fractures. 8 The most common teeth involved in dental trauma are maxillary incisors as compared to mandibular incisors because any blow to the mandibular teeth are dissipated because of the nonrigid connection of the mandible to the base of the cranial cavity. 9
In the early era of Hippocrates, some of the documented cases of dentoalveolar fractures were treated by splinting the teeth via bridle wires with the principle being that fixation of loose teeth or bony segments allow for hard and soft tissue healing. Today, too this principle is followed though with more refined techniques and armamentarium.
According to various studies, boys suffer more traumatic injuries than girls which are usually attributed to the behavioral difference as boys tend to be more energetic and inclined toward outdoor activities and contact sports. 10 According to P. Juneja et al., who conducted a study of 4000 students of 8-15 years of age in 60 schools of Indore city, India, there is a 10.2% incidence of traumatic dental injury of which 68.38% were boys which were approximately twice as higher in females being 31.62%.
The time elapsed because the injury is of paramount importance as it influences the choice of treatment. 11 According to Andreasen et al, 1 repositioning of the dislocated teeth becomes more challenging after 48 h of the injury. However, in the present case, the repositioning was performed around 12 h after the injury, so treatment was possible and the results were successful.
According to Dewhurst et al, intrusive luxation is the most serious form of luxation and it can either be allowed to erupt spontaneously (within 2 to 3 months) if it's an immature tooth or it requires surgical/orthodontic extrusion if its a permanent tooth. In this case, because these were permanent teeth, surgical intervention was thought to be the best approach for extrusion.
Necrosis of pulp is also one of the important consequences of luxation injuries and it depends on the type of luxation and state of root development. It is more common in mature teeth as compared to immature ones. 12 In cases where the tooth/teeth become nonvital or start showing root resorption, pulpectomy or RCT is advised.12, 13 According to Cvek, if permanent teeth after luxation injuries start showing external root resorption, it is advocated to treat such teeth by calcium hydroxide cement which ceases the progression of inflammatory external root resorption, the resorptive lacunae get filled with newly formed bone, and periapical radiolucencies get healed.
In our case, the patient was put on a strict follow-up to detect any signs of root resorption or inflammation which would have been addressed immediately, however, the healing was uneventful so no further intervention was needed.
After a traumatic luxation of teeth, it is of paramount importance to reposition them in their anatomically correct position and stabilize them by splinting for the proper healing of periodontal ligament and neurovascular supply while maintaining their function and aesthetics. The ideal splinting time ranges from 4 to 8 weeks, 8 weeks being in cases where there is a lack of periodontal support and marginal bone breakdown.
The use of composite resin and orthodontic wire to splint is a type of nonrigid splinting which has the advantages of permitting physiologic tooth mobility and easy cleansing, preventing ankylosis and biofilm accumulation from happening respectively.
In this case, however, because the labial alveolar bone plate was preserved, the teeth were vital and the periodontal ligament was intact, the teeth were not subjected to root canal treatment and splinting was done for 4 weeks followed by a follow-up which showed uneventful healing.
Conclusion
Preventing accidents from happening which might result in pediatrics dental trauma is not possible, but their associated complications can be prevented by prompt treatment and follow-up. Awareness regarding pediatrics dental trauma, teeth storage medium should be instilled in parents, school teachers, and common people so that they can contribute to a better prognosis of the treatment. Also, the importance of early and skilled care following any pediatrics dental trauma should be made to understand to any and everyone who deals with children of pediatrics age group in any way because as its correctly said—“A stitch in time, saves nine.”
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Necessary ethical clearances and informed consent was received and obtained respectively before initiating the study from all participants.