
Abstract
Reconstruction of maxillofacial defects is a big challenge for an oral and maxillofacial surgeon. The defects of the floor of oral cavity are difficult to treat in particular. Various techniques are being used to treat these defects with variable success. The purpose of this case report is to present the use of a lingual mucoperiosteal flap for the closure of a defect of the oral cavity.
Introduction
The reconstruction of the defects of the floor of mouth poses a great challenge as faulty treatment can interfere with tongue movements. The primary reason for the reconstruction of these defects is to separate the oral cavity from the neck. The method of reconstruction should not interfere with swallowing and speech patterns. Various available options range from local flaps such as nasolabial, submental, infrahyoid, and facial artery myomucosal flap. 1 The purpose of this case report is to present the use of lingual mucoperiosteal flap for the closure of the defect of the oral cavity.
Case Report
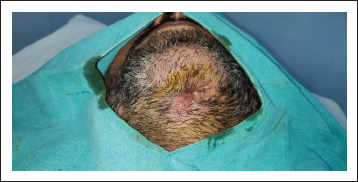
A patient presented to our Department of Oral and Maxillofacial Surgery with facial injuries involving chin and floor of the oral cavity. There was a history of trauma to the chin area with a sharp object a few days back. The sharp object entered the oral cavity by perforating through the floor of the oral cavity. The soft tissue injury was managed at a local health care center by primary closure of intraoral and extraoral wounds. Unfortunately, there was wound infection leading to dehiscence of a wound leading to drooling of saliva from chin region via the defect of the floor of the oral cavity. The patient was then presented to our department for definitive management. On clinical examination, there was an extraoral wound in relation to chin with evidence of infection (Figure 1). Intraorally, the defect of the floor of the oral cavity was evident along with a few vicryl sutures indicating the failure of primary closure (Figure 2). A comprehensive treatment plan was formulated, and it was planned to manage the infection prior to any definitive repair. Antibiotic therapy was started to control the infection. The wound care was done regularly by intraoral irrigation and extraoral dressings. The meticulous wound care resulted in wonderful healing of extraoral wound by secondary intention. Unfortunately, a very minute pinpoint sinus tract remains at chin region, leading to drooling of a small amount of saliva extraorally (Figure 3), and the intraoral defect did not heal completely (Figure 4). As the infection was under control, definitive closure of the defect was planned. The extraoral sinus tract was excised, and the opening was closed by Z-plasty technique (Figure 5). The intraoral defect of the floor of the oral cavity was occluded or covered by mobilizing the lingual gingival mucoperiosteal flap toward the defect and secured with resorbable vicryl sutures. The lingual cortex that was exposed because of migration of the flap was covered by White’s Head Varnish gauze dressing secured with the help of interdental sutures (Figure 6). The nasogastric tube was placed for feeding to avoid intraoral wound contamination by stagnation of food. The patient was reviewed regularly to look for healing. After one week, the intraoral pack and extraoral sutures were removed. Thereafter, the patient was reviewed weekly for six weeks. There was excellent healing in relation to extraoral (Figure 7) and the floor of the oral cavity defect along with adequate granulation tissue formation to cover the lingual cortex of mandible (Figure 8).
Preoperative Photograph Showing Extraoral Wound.

Preoperative Photograph Showing Intraoral Wound.

Preoperative Photograph Showing Extraoral Sinus Tract.

Preoperative Photograph Showing Intraoral Defect of Floor of Oral Cavity.

Intraoperative Photograph Showing Extraoral Sinus Tract Excision and Primary Closure by Z-Plasty Technique.

Intraoperative Photograph Showing Intraoral Pack to Cover Lingual Cortex of Mandible.

Postoperative Photograph Showing Healed Extraoral Sinus Tract.
Postoperative Photograph Showing Healed Intraoral Defect of Floor of Oral Cavity.

Discussion
The reconstruction of defects of the floor of the mouth possesses a great challenge as faulty treatment can interfere with tongue movements. The primary reason for the reconstruction of these defects is to separate the oral cavity from the neck. The method of reconstruction should not interfere with swallowing and speech patterns. Various available options range from local flaps such as nasolabial, submental, infrahyoid, and facial artery myomucosal flap. 1 Smaller defects of the oral cavity can be managed by primary closure, use of local flaps, or by secondary healing from mucosalisation or by use of split-thickness skin grafts. 2 To the best of our knowledge, the use of a mucoperiosteal flap was not reported by any author as a viable option to cover small defects of the floor of the oral cavity. The idea for the use of this technique comes from Tarnow’s technique to cover root surfaces in patients with gingival recession. 3 In this technique, a semilunar incision was given over the labial mucoperiosteal tissues, and a small split-thickness flap was mobilized coronally to cover the root surfaces. The small raw area is created apically, which heals by secondary intention. Here, we have done exactly the opposite of it. The lingual mucoperiosteal tissue in relation to teeth is reflected and is mobilized apically (toward the floor of the oral cavity defect) to cover the defect primarily. This leads to the creation of raw or denuded area coronally, which healed by secondary intention. We advocate to explore this simple technique for smaller defects of the floor of the oral cavity before opting for complex flaps.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Necessary ethical clearances and informed consent was received and obtained respectively before initiating the study from all participants.