
Abstract
Background
Pectoralis major myocutaneous (PMMC) flap has been used in head and neck reconstruction since its initial description. Its reliability and versatility made it the workhorse flap until the widespread rise of the microvascular surgery. The vascular supply to the pectoralis major is based on branches of the axillary artery. The skin overlying the pectoralis major receives most of its blood supply from fasciocutaneous perforators. In the literature, the flap is also associated with a high incidence of complications in addition to its large bulk. This case report shows the reliability and indication of this flap in the reconstruction of the oral defects.
Case Report
A 42-year-old male patient reported with the chief complaint of increasing pain and nonhealing ulcer in his left lower posterior teeth region with reducing ability to open mouth. On clinical examination, an ulceroproliferative lesion was found on the left retromolar trigone region (RMT). Biopsy was performed which demonstrated squamous cell carcinoma of left RMT. Modified radical neck dissection type II was performed with hemimandibulectomy without disarticulation with reconstruction with the PMMC flap.
Conclusion
It can be concluded that the flap-related complications can be minimized by proper planning with regard to the length of the PMMC flap, the defect location, and the type of mandibular osteotomy. There are some situations in which pectoralis major still appears as a valuable option even in facilities performing free flaps and for patients in good general conditions.
Introduction
The pectoralis major myocutaneous (PMMC) flap is the most commonly used flap for head and neck reconstructive surgery, described by Ariyan1, 2 as a “work horse” of oral cavity reconstruction.1, 2 This flap has largely been taken over by free vascularized flaps including its proximity, the simplicity of harvesting, and alternative in case of microsurgical flap failure. This flap is a very effective one-stage reconstruction which is reliable and carries minimum donor site morbidity. The major disadvantages of the PMMC flap are neck mobility restriction and this vascular pedicle of the flap 180°. The second most common disadvantage of this flap is its thickness because of the amount of fat between the pectoralis muscle and the overlying skin paddle which causes reduced speech function and swallowing.
The harvesting of the PMMC flap is a simple and short time procedure. It is the ability to provide skin and muscle in its commonest form or muscle alone or in combination with the ribs. It is a reliable, single-stage procedure and provides an excellent volume to fill virtually all oral cavities and most cutaneous defects. Its length is adequate for all oral cavity lesions but being placed above a line over the zygomatic arches causes problems.
To reduce the thickness and bulkiness of the PMMC flap, a modification has been introduced for the reconstruction of hypo/oropharyngeal defects without the skin paddle overlying the muscle. 3 There are some major complications of the PMMC flap that are not to be ignored, and the rate of overall complications raised some concerns in the past.
Some possible indications are soft tissue defects of the oral cavity, hypopharynx, oropharynx and skin of the head and neck, coverage of the carotid artery especially after radical neck dissection with prior or anticipated radiotherapy, skull base coverage, alternative to free flaps in instances of free flap failure, and lack of availability of free flap reconstruction.
Case Report
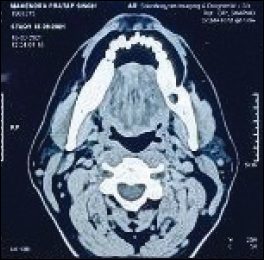
A 42-year-old male patient presented with the chief complaint of pain and nonhealing ulcer in his left lower posterior teeth region with reduced mouth opening (Figure 1). On clinical examination, ulceroproliferative lesion was found on the left RMT. The pain was dull, insidious in onset, and without aggravating and relieving factors. His mouth opening was about 12 mm. He gave tobacco chewing history as 5 to 6 times daily for more than 10 years. On general physical examination, he was well-built and well-nourished without any systemic illness. Intraorally ulceroproliferative growth was found. Superoinferiorly, it was extended from the level of occusal line to the lower border of the mandible. Anteroposteriorly, it extended from the mandibular second molar to the anterior border of the ramus. The growth was 2 × 3 cm in size. On palpation, all inspectory findings were confirmed. Submandibular lymph node was clinically palpable, and clinical impression was carcinoma of the left RMT. Biopsy was performed and demonstrated well-differentiated squamous cell carcinoma of the left RMT region. PET-CECT revealed ill-defined soft tissue lesion in the left retromolar region and left gingivo-buccal and gingivo-lingual sulcus (Figure 2).
Extraoral Photograph Showing Reduced Mouth Opening and Ulceroproliferative Lesion on Left RMT Region.

PET-CECT Showing ill Defined Soft Tissue Lesion in Left Retromolar Region and Left Gingivo-Buccal and Gingivo-Lingual Sulcus.
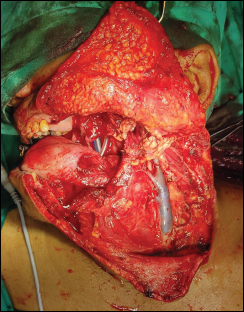
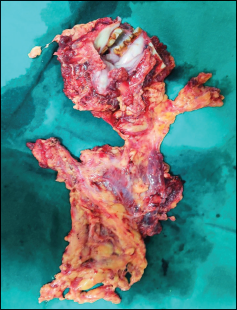
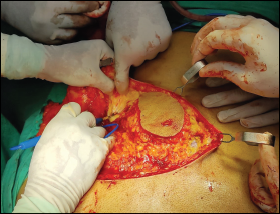
The treatment was planned: it included modified radical neck dissection type II with segmental mandibulectomy without disarticulation followed by reconstruction with PMMC flap (Figure 3). The histopathological examination reported no evidence of any metastasis (Figure 4). Wide local excision of the lesion was performed up to the RMT. The PMMC flap was raised on the left side to reconstruct the complete intraoral defect (Figure 5).
Modified Radical Neck Dissection Type II With Oropharangeal Defect With Hemimandibulectomy Without Disarticulation.
Resected Specimen.
Left Pectoralis Myocutaneous Flap Harvested for Reconstruction of Oro Pharangeal Defect.
Postoperatively, the patient was given care in the intensive care unit for 2 days He was extubated on the first postoperative day. The extraoral dressings were changed and the oral hygiene was maintained and monitored. The defect was dressed with betadine gauze till it got covered with healthy granulation tissue (Figure 6).
Well Healed Skin Paddle Covering Complete Oro Pharangeal Defect. There is Hair Growth From the Skin Paddle.

Discussion
The pectoralis major is a very broad and fan-shaped muscle which originates from the medial side of the clavicle, sternum and costal cartilage, and the external oblique muscular aponeurosis, and it inserts into the crest of the greater tubercle of the humerus. It acts as an adductor muscle, medial rotator muscle, and extensor of the arm. The basic principle of the flap is to harvest the muscle with an appropriate paddle of the skin. The muscle runs diagonally across the chest, receiving its blood circulation at its deep surface from the descending branch of the acromiothoracic artery. This vessel runs from beneath the midpoint of the clavicle and itself runs medially and inferiorly. The muscle provides a random pattern of perforators to the skin. Venous drainage of the PMMC flap is done by the vena comitantes of the supplying arteries. Innervation of the flap is done by the lateral and medial pectoral nerves. The clavicular head is supplied by the lateral pectoral nerve, and the sternocostal head is supplied by the medial pectoral nerve.
Because of atrophy after division of the motor nerves, 50% reduction of bulkiness of the PMMC flap was reported within 3 months. 4 The fifth rib segment can be provided in the flap, but in cases of postoperative radiotherapy, this is not recommended. 5 The use of an inframammary incision which is a C-shaped incision in females is described to minimize the distortion of the breast and also for the aesthetic reason. 6
Apart from good results, the complications are also high. The technique of the harvesting of the flap is easy, but the chances of postoperative complications should not be ignored. 7 Partial (4% to 14%) or complete (1% to 7%) necrosis of the flap is reported; other complications such as fistula formation, dehiscence, infection, and hematoma are also described. 8 McLean et al 9 described complications in patients treated with radiotherapy. Most common complications were donor site hematomas or seromas, donor site wound dehiscence or skin necrosis, pulmonary complications, surgical site infection, osteochondronecrosis of the ribs, wound dehiscence and plate exposure, masking of recurrent malignancy, distortion of breast tissue, orocutaneous fistulas, hair growth, and muscle atrophy.
Hsing et al 10 studied 491 patients treated for oral squamous cell carcinoma, 100 of which completed a quality-of-life questionnaire: no significant difference in the quality of life between patients with free flaps versus PMMC was noted. They did not find any differences regarding swallowing, activity, chewing, pain, appearance, or anxiety. They found significant differences between the free flap and PMMC flap patients in speech, shoulder mobility with good result with free flap.
Xiao et al observed 2 groups on oral squamous cell carcinoma: one group reconstructed with an anterolateral thigh (ALT) flap and the other with the PMMC. They found that there are no significant differences between both the groups for pain, activity, swallowing, chewing, and speech, but there were significant differences between the PMMC and the ALT groups for the shoulder mobility and appearance factor. 11
O’Neill et al 12 studied a comparison between the radial forearm free flaps and the PMMC flap in the reconstruction of oral and oropharyngeal malignancies. He concluded that there were no significant differences in deformity, diet, or socialization; only 22.2% of patients were reconstructed with the PMMC flap. Patients were satisfied with their speech in which reconstruction was done with the PMMC flap (22.2%) compared with 53.1% of patients reconstructed with the radial forearm free flaps.
The 2 utmost important factors of the flaps are functional results and morbidity. When comparing the free flap with the pectoralis major patients, the patients in poor health conditions were recommended pedicled flaps, which had short operative time, and technical ease and low morbidity.
Conclusion
The rate of complications related to the PMMC flap can be minimized by proper treatment planning, the defect location, and the type of mandibular osteotomy. Incorporation of enough perforators in the skin pedicle should be given special attention. Extensive electrocoagulation should be avoided. In the same way, the PMMC flap can be used to protect the carotid axis after salvage radical neck dissection following radiotherapy failure.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Necessary ethical clearances and informed consent was received and obtained respectively before initiating the study from all participants.