
Abstract
Introduction
Global head and neck cancer has been reported at 57.5% in Asia, especially India. 1 Oral cavity squamous cell carcinoma (OCSCC) accounts for 10%–15% of all head and neck cancers. 2 To reduce this cancer burden, emphasis should be on prevention and speedy redressal for OCSCC without compromising the quality of treatment rendered. The gold standard for oral cavity and oropharyngeal defect reconstruction has been the Radial artery forearm flap (RAFF) together with the free Anterolateral thigh flap depending on the defect.3, 4 However, these free tissue transfers are not feasible in high-risk patients, socio-economically poor patients, rural areas where the cancer burden is relatively higher and healthcare facilities which are not equipped to perform free flap procedures. Therefore, our study aimed to revisit the infrahyoid flap (IHF) in this modern era of free flaps in head and neck rehabilitation as a workable substitute.
Materials and Methods
A retrospective analysis was done of 12 patients after resection of the primary tumor from the oral cavity. The subsites reconstructed were the tongue, floor of the mouth, mandibular gingivobuccal sulcus and soft tissue coverage of alveolar defects. All the cases were of squamous cell carcinoma, small to medium-sized anticipated defects who underwent infrahyoid flap as an alternative to the free flap option.
The study sample was derived from the population of patients who presented to the Tertiary Care Institute, Vaishali, Ghaziabad from March 2020 to May 2021 with a median follow-up of one year. Patients had given their informed consent for participation in the research study. The radiological examination included an MRI scan of the face and neck, a metastatic workup and a routine blood investigation was also done. The exclusion criteria were patients with T4 and N3 disease, recurrence cases, patients’ post-radiation or chemoradiation and those who did not consent to participate in the study.
Charts were reviewed for patients who underwent reconstruction with IHF by a single surgeon in the department. For the outcome, the patient was assessed for flap dimensions, length of hospital stay, pTNM, surgery performed, neck dissection, and complications like total flap loss, partial skin necrosis, hematoma and neck suture line gap.
Surgical Technique
In the harvesting of the infrahyoid flap, the modifications advocated by Dolivet et al. were used in all the cases. The flap was explicated for the first time by Wang in 1979 and technical modifications were later popularized by Dolivet et al. 5 First the margins of the flap were marked (Figure 1).
Surface Marking of the Infrahyoid Flap and Neck Incision.
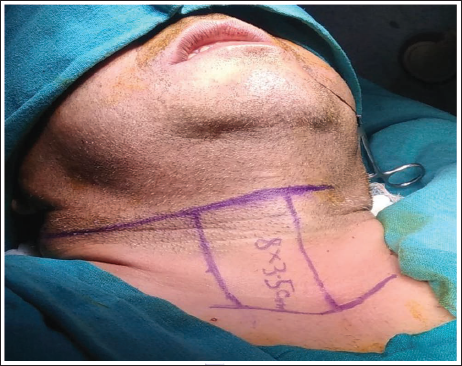
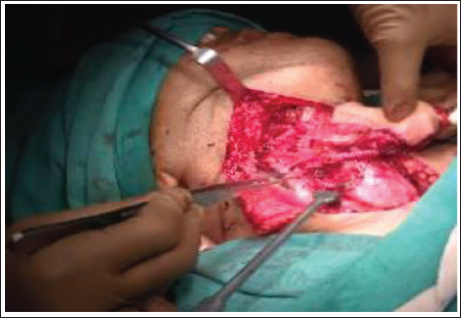
The medial margin was the midline of the neck with a maximum width of approximately 4 cm. The superior and inferior margins were delineated by the hyoid bone and manubrium respectively in the midline with another line laterally taken on the anterior border of the sternocleidomastoid maintaining a flap width of at least 3.5 cm. The flap harvest starts medially in the midline of the neck with a vertical incision deepened to the plane of the thyroid gland and the trachea. The inferior incision was then made just above the clavicular bone and the strap muscles were divided. The internal jugular vein and the omohyoid muscle lying on the lateral aspect were exposed and identified. The superior belly of the omohyoid muscle after division from the intermediate tendon was elevated to be included in the flap. Before elevating the flap from the bed, the strap muscles of the neck were sutured to the skin paddle to avoid shearing the flap. The flap was then raised in an avascular plane, which lies between the strap muscles and the thyroid gland and the cricothyroid membrane. As the flap was being elevated the posterior branch of the superior thyroid artery supplying the thyroid gland was ligated. Careful soft tissue dissection was done in the superolateral part of the flap to circumvent injury to the feeding vessels. As the flap elevation continued, the strap muscle was incised at the superior aspect. The integrity of the superior thyroid artery, vein and feeder vessels was assessed by preserving the anterior jugular veins and veins adjacent to the digastric belly (Figure 2). The flap was then mobilized and transferred to the oral cavity (medial to mandible) for defect reconstruction (Figures 3 & 4).
Harvested Infrahyoid Flap along with Pedicle.
Defect Created After Primary Tumor Resection.

In-setting of the Flap at the Defect Site.

Results
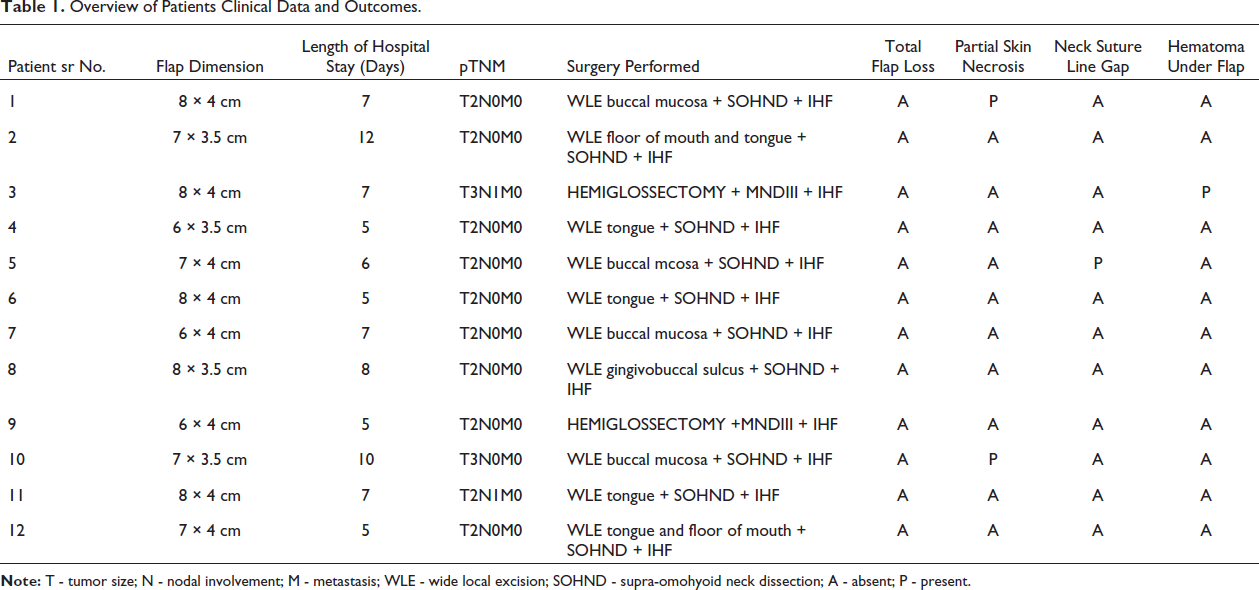
The maximum dimension of the IHF used was found to be 8 × 4 cm. Out of 12 patients, two patients developed partial flap necrosis (Figure 5).
Partial Necrosis of the Flap.

One developed a hematoma under the flap which gradually subsided after stopping anticoagulant drugs. One patient developed a neck suture gap due to tight closure (Z-plasty done for closure later) (Table 1).
Overview of Patients Clinical Data and Outcomes.
Although minor conservative procedures were done to manage these initial complications, the postoperative outcome of the flap in terms of esthetics and function was found to be noteworthy after one month in all the patients. The donor site healed with minimal post-operative scarring (Figure 6).
Post-operative Healing After Four Months.

Discussion
Reconstruction of oncologic defects of the oral cavity requires an advanced understanding of all available choices for reconstruction and a multidisciplinary team approach, as it is a diversified and challenging region. An optimal reconstruction enhances the residual function ensuring optimal speech, swallowing, and functionality of the preserved structures and restoration of form with acceptable aesthetic results. The decision regarding the type of reconstruction depends on the characteristics of the anticipated defect and patient-associated factors such as age, performance status, general co-morbidities and former treatments.
Microvascular free flaps have become the foremost widespread method employed in the reconstruction of head and neck cancer resections because of their versatility and reliability. The free flap most commonly used is the RAFF.6–9 In this retrospective study, we have considered the choice of using IHF instead of using free flaps. The idea of re-envisioning the IHF was because of having a long waiting list of patients awaiting treatment and at a larger picture as a developing country with a high cancer burden. Usually, head and neck cancer in a developing country is seen to affect mostly the underprivileged, the number of trained on cosurgeons in rural areas is quite sparse and healthcare facilities are usually not well equipped in these areas to perform a free flap procedure. Therefore, to cater to the long waiting list of patients just excising the tumor is not sufficient, but, also reconstructing with a flap which is analogous to the free flap thereby reducing the cost of surgery, faster recovery and providing an acceptable quality of life ensuring a faster return to resume their livelihood. We have shared our experience by evaluating its efficacy based on our observation of intraoperative and postoperative results.
The IHF, a pedicled myocutaneous flap, has been used in reconstructive procedures for small and medium-sized defects in the floor of the mouth, the tongue, buccal mucosa, patch pharyngoplasty and alveolar ridge. It has additionally been reported to be used for myofascial transposition, to close iatrogenic pharyngeal and esophageal fistulas following anterior cervical spine surgery and to recreate the base of the tongue if its attachment was not detached from the hyoid as it has been shown to provide a reasonable functional result. It has been used successfully even for lower lip reconstruction in one stage without the need for further correction.10–13
The advantages of the flap we noticed are simple surgical technique, shorter time for harvesting which offers good function and cosmesis, hairless region and does not require a change in the positioning of the patient. Since the infrahyoid flap was close to the recipient site there are no additional scars on the neck.11, 12, 14, 15 It was well accepted by the patients since the donor site was also in the vicinity of the recipient site.13, 16 The distress and recovery at the infrahyoid donor site were quite negligible when compared to free flaps as they can be closed by primary intention with Z-plasty as and when required. 17 An Adequate function was achieved in all the cases. In comparison with free flap, it has a shorter learning curve since the head and neck surgeons are familiar with the anatomical region, therefore, making reconstruction easier for a novice surgeon.15, 16 Neither is any microsurgical expertise or instruments nor a second team to harvest the flap required, also it is a one-step procedure all of these contributing drastically to cutting down the cost of surgery.13, 14 Deganello et al., in their study have also shown great economic benefits with neck flaps when compared to free flaps. 18 The mean discharge time in our study was just seven days post-surgery.
Muscle innervation to the infrahyoid flap is provided by the ansa cervicalis. By preserving the ansa cervicalis, it can be made into a sensate flap thereby offering more advantages like providing some movement to the neo-tongue which becomes particularly helpful during tongue reconstructions preventing fibrosis and atrophy, also when omohyoid muscle is suspended to tonsillar fossa it prevents aspiration.11, 19 In the study by Deganello and Leemans and Hell et al. IHF was used as the first alternative to FRFF in high-risk patients having severe general comorbidities.9, 11
The downside of this flap that we noticed was partial skin necrosis, which usually resolves without further surgical revision but may prolong the hospital stay and cause serious complications if a severe salivary leak occurs. 12 There are dimensional limitations and unreliability of the skin paddle. The IHF must always be aforethought and cannot represent a backup solution in case of other flap failures, since it cannot be used in a previously operated neck. 9 In a study by Deganello and Leemans and Minni et al., the frequency of complications was reported to be 0%–47%, with failures mainly related to partial skin necrosis and the rate of total flap necrosis was about 1%.9, 20 In our study complications were seen in 33.33% of cases, of which, partial skin necrosis complication was around 16.66%, however, no flap loss was detected. The other complications seen were hematoma under the flap and neck suture gaping which accounted for 8.3% of cases, respectively. According to our observation and study reported by Hongshi et al. and Saluja et al.,21, 22 the cause of skin paddle necrosis in IHF was noticed due to the insufficient venous return from the anterior jugular and superior thyroid vein. This complication can be managed by the preservation of the external or internal jugular vein with special attention on preserving the anterior jugular vein (AJV). Preserving these veins makes the neck dissection more meticulous and demanding. Also, we should ensure that the tunnel to transfer the flap intra-orally is sufficiently large to ensure there is no compression of the pedicle of the flap. In the study by L. Xiaoming et al., 23 they suggested the use of pre-operative 3D CT reconstruction of the AJV to visualize any anatomical variation and assess the venous drainage to plan the flap design accordingly, which will reduce the chances of damage to the AJV. For superior esthetic results, and for managing the postoperative scar in the neck, a Z-plasty can be performed as a secondary procedure.
Some of the contraindications for the use of these flaps mentioned in literature and based on our experience with the flap are prior neck surgery like thyroid surgery or neck dissection, prior neck irradiation, ligation of external carotid artery and branches, N3 & T4 lesion, simultaneous reconstruction with alloplastic material and peripheral vascular disease. There is a risk of injury to the external laryngeal nerve which can be prevented with meticulous dissection during harvesting of the flap.9, 8, 15, 24
Conclusion
In this limited series of patients in our study, we would like to conclude that in a developing country where the cancer burden is high, the IHF stands as a very reliable alternative due to the many benefits over the free flap in soft tissue reconstruction or for coverage of medium to small sized alveolar defects. It has shown promising results in terms of function, reliability, cost-effectiveness, faster recovery and in patients with multiple comorbidities. Henceforth, callow on cosurgeons should be trained and encouraged to use the IHF as a viable option in this era of free flap for a speedy treatment to ensure a robust and prosperous cancer-free nation.
Footnotes
Declaration of Conflict of Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Statement of Informed Consent and Ethical Approval
All procedures performed in this study involving human participants were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Written and informed consent was obtained from all individual participants included in this study.