
Abstract
Abstract
Background: Fractures of the mandible can be studied and described in anatomic terms, functional considerations, treatment strategies, and outcome measures. The performance of any fixation system depends on multiple factors including plate adaptation, screw placement, bone quality, drilling conditions, and postoperative patient compliance. Bite force assesses masticatory muscle function under clinical and experimental conditions.
Method: 30 patients with isolated, noncomminuted mandibular fractures were randomly divided into two equal groups. Group 1 patients were treated using 3-dimensional locking miniplates and group 2 patients were treated with standard miniplates. The bite forces were recorded at definite time intervals: preoperatively, and second week, sixth week, third month, and sixth month postoperatively.
Result: At 6 weeks postoperative, 3 month postoperative, and 6 month postoperative, the mean bite force was found to be significantly higher among group 1 patients as compared to those in group 2 in all the sites. While at 2 week postoperative, the mean bite force was found to be significantly higher in Group 2 as compared to Group 1 at incisor region.
Conclusion: The overall results of the present study show better performance in bite force for the 3-dimensional locking miniplate when compared with standard miniplates.
Introduction
Mandible is the most common bone involved in facial trauma mainly due to road traffic accidents and assaults. The fixation techniques have evolved from external fixation to internal fixation. Continuously researches and advancements in the maxillofacial surgical techniques and armamentarium have made it possible to almost immobilize and orient any part of the facial skeletal. Various systems of osteosynthesis have been designed which have become smaller and more simple to handle, and help avoid extraoral procedures with the passage of time. 1
In 1973, Michlet et al introduced miniplate osteosynthesis, and Champy et al further developed it.2,3 Miniplates are a preferred method of fixation in craniomaxillofacial surgery because of obvious advantages over other plating systems: relatively smaller size, ease of adaptability and placement via intraoral approach, etc. 4 Farmand, in 1995, developed 3-dimensional (3D) plates which were designed in a quadrangular shape that was formed by joining two miniplates with interconnecting crossbars. 5 This 3D configuration was aimed at achieving the 3D stability and providing better resistance against torsional forces. The internal mini locking system was developed in 2003 to avoid loosening of hardware and for better adaptation. The purpose of the present study was to determine the maximum bite force following the treatment of mandibular fractures with 2 mm 3D locking miniplates and 2 mm standard miniplates.
Materials and Methods
The study was conducted on the patients diagnosed with isolated noncomminuted mandible fractures and reporting to the Department of Oral and Maxillofacial Surgery, SPPGIDMS, Lucknow. Clearance from institutional ethical committee was obtained and written informed consent was received from all the patients. The diagnosis was made based on the complete history, clinical examination, and radiographic interpretation. Routine blood investigations were performed. The surgical procedure and the postoperative follow-up done were explained to all the patients. Patients (American Society of Anaesthesiologist—Groups I and II) with isolated noncomminuted mandible fractures without pre-existing infection and sign of nerve injury were selected for the study. Patients with edentulous mandible, unwilling or medically unfit for open reduction and internal fixation, with comminuted fracture, or any other associated facial fractures, were excluded from the study.
30 patients were randomly assigned into 2 equal groups according to the type of plating system used in fracture fixation. Group 1 included patients whose fractures were fixed with 2 mm 3D locking miniplates, whereas group 2 consisted of patients whose fractures were fixed with 2 mm standard miniplates. No postoperative maxillomandibular fixation was done in any patient.
All bite force measurements were recorded using a bite sensor. Patients were informed about the experimental procedure and the subjects were seated comfortably on a chair in an upright position. A polythene sheet or a plastic wrapper was used to cover the biting sensor. It was placed on the incisal edge of the anterior teeth for measuring the anterior bite force (ABF), and then placed on the occlusal surface of the first molar on the right side for measuring the right posterior bite force (RBF). Further it was placed on the occlusal surface of the first molar on the left side for measuring the left posterior bite force (LBF). The patients were asked to bite hard on the sensor and the maximum bite force reading on the charge meter display was recorded. 5 such readings were taken and then alternated on each side, with an interval of 1 minute to avoid muscular fatigue. The measurements were recorded preoperatively, and second week, sixth week, third month, and sixth month postoperatively.
Data were entered into Microsoft Excel spreadsheet and then checked for any missing entries. It was analyzed using Statistical Package for Social Sciences (SPSS) version 21 (IBM Chicago). Bite force was summarized as mean and standard deviation. The intergroup comparison was done by independent student’s t-test. The level of statistical significance was set at 0.05.
Results
The fracture sites in both groups were stabilized successfully following open reduction internal fixation without any postoperative maxillomandibular fixation. There were no postoperative complications observed in any case.
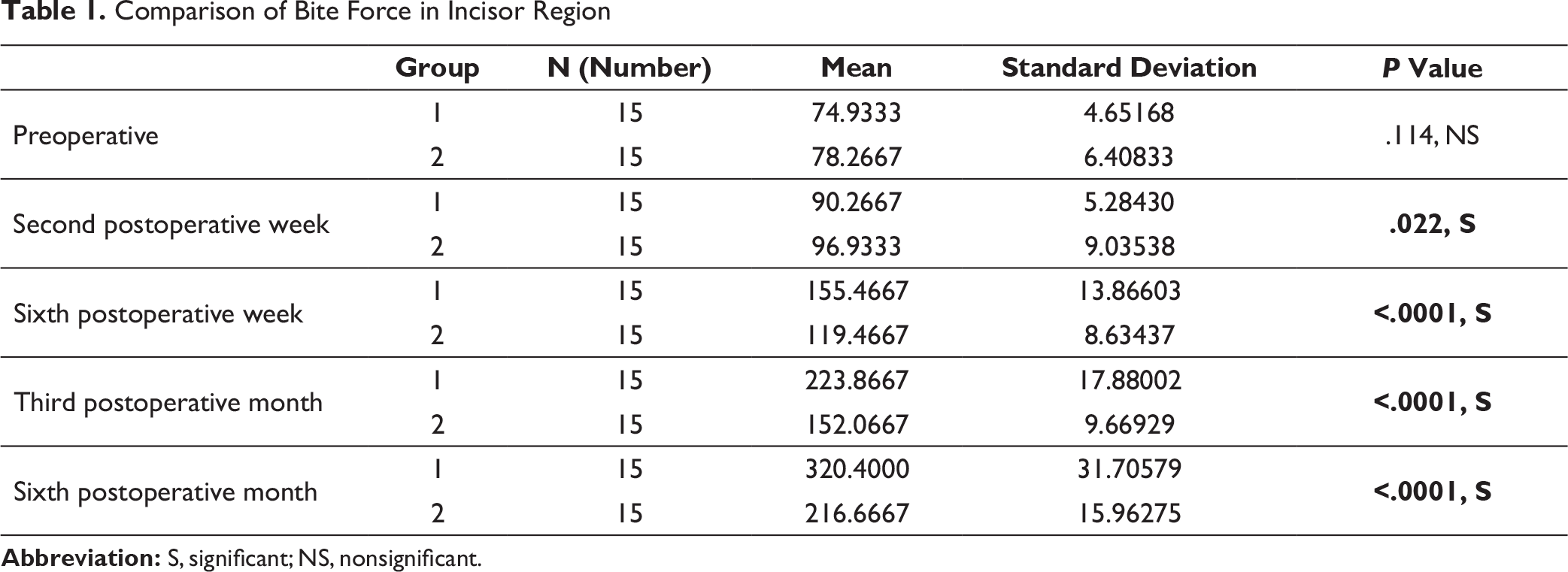
Comparison of Bite Force in Incisor Region
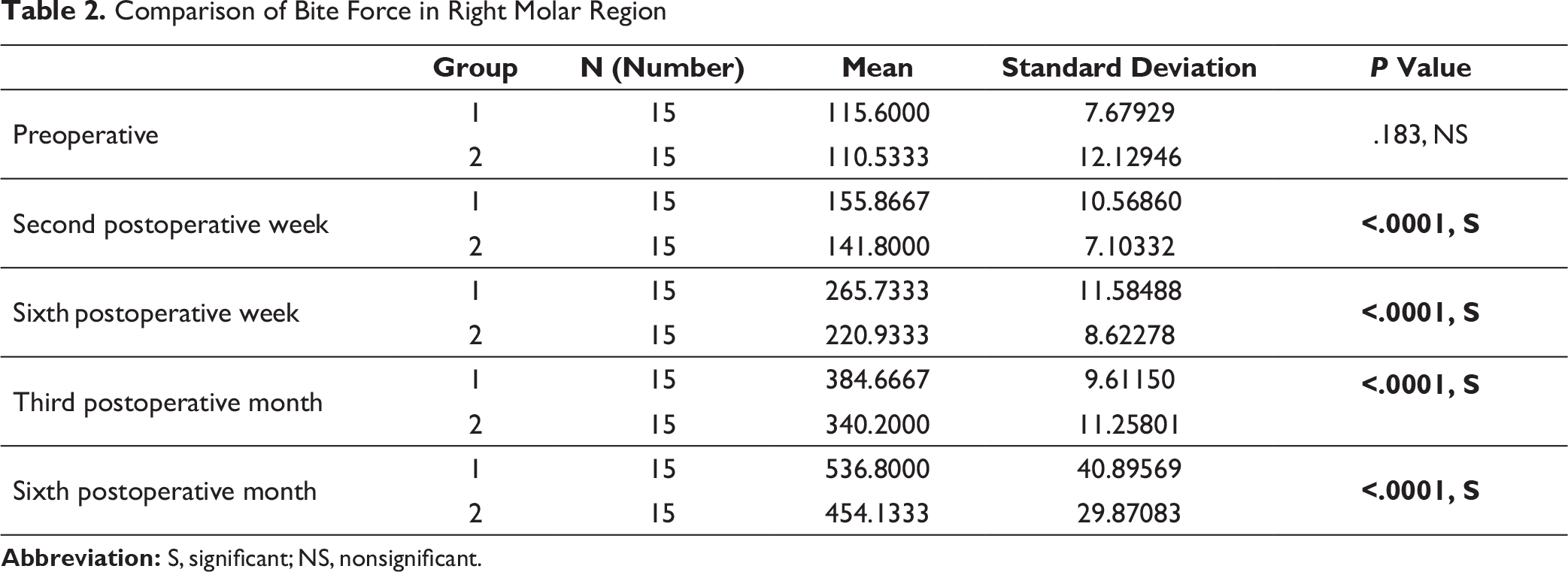
Comparison of Bite Force in Right Molar Region
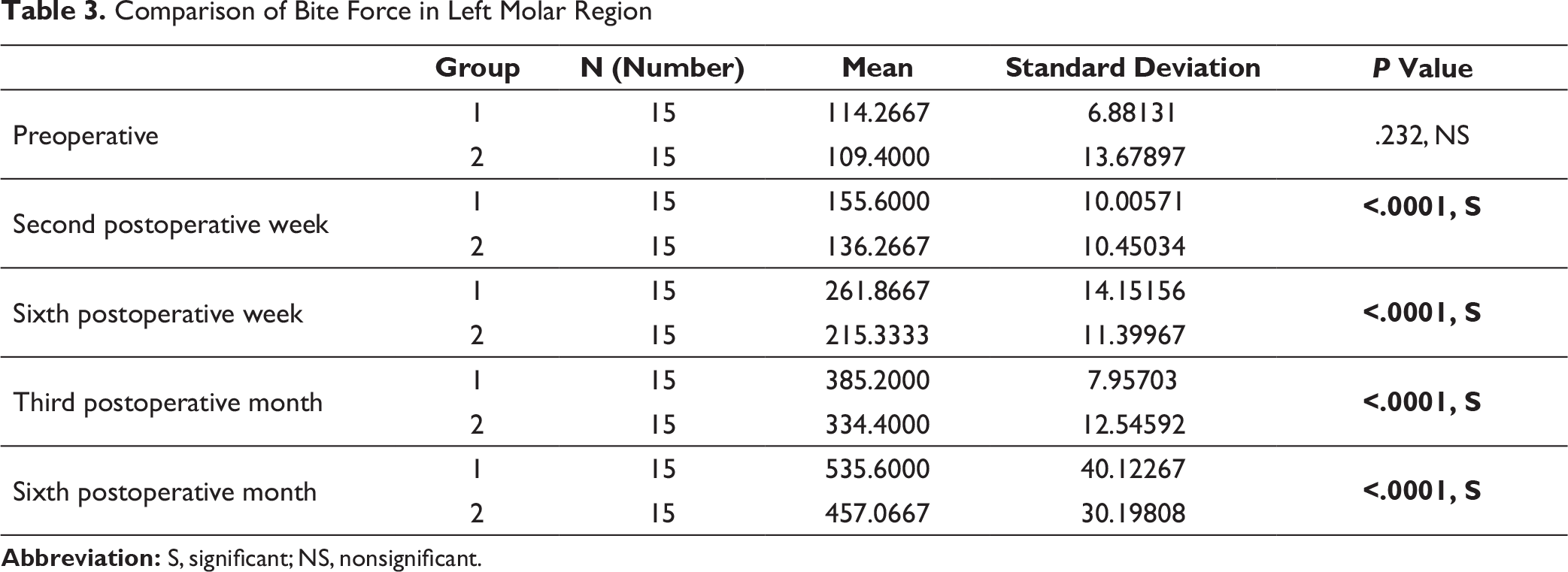
Comparison of Bite Force in Left Molar Region
Discussion
The mandible is the second most commonly fractured bone of the maxillofacial skeleton because of its location and prominence. The pattern and site of the fracture are mainly decided by the mechanism of injury and the direction of the vector of the impact. In addition to this, the patient’s age, the status of dentition, and the physical properties of the causing agent also have a direct impact on the pattern of the resulting injury. 6
Conventionally, the plate must be adapted perfectly to the underlying bone to avoid any alterations in anatomically reduced fragments. There have also been incidents of loosening of one or more screws during the convalescence period, resulting in changes in occlusal relationship. This problem, to an extent, has been overcome by the advent of locking plate/screw systems where the screw locks not only the bone but also the plate, and serves as a mini-internal fixator. It is assumed that this relationship of a plate and a screw will reduce the number of fixation screws per osseous fragment, and thus, minimal hardware can achieve the same fixation objectives as with bulkier plating systems. 7
Barde et al compared the efficacy of 3D plates over Champy’s miniplates in mandibular anterior fractures and finally concluded that the fixation of fracture segments in the anterior region of the mandible with 3D plates provided better 3D stability probably because of its geometric design, and had lesser rates of postoperative complications in terms of infection and morbidity. 8
Agrawal et al 9 performed a randomized clinical trial comparing the efficacy of 2-mm locking miniplates and 2-mm standard miniplates in the management of mandibular fractures. They concluded that locking miniplates were comparatively more efficacious in terms of better plate adaptation, stability, and minimal compromise of the periosteal blood supply. Increased postoperative bite force was an additional advantage of locking a miniplate over a standard miniplate. 9 Similar results were observed in an in vitro trial by Gutwald et al, who found that the stability of the locking screw plate system was 3 times higher than conventional miniplates. 10
Bite forces reduce significantly following trauma to the mandible or operative procedure because of the protective neuromuscular mechanisms of the masticatory system. Another major factor is the patient’s willingness to bite, which is related to mental attitude. There is a gradual increase in the bite force from the second postoperative week. The reason for this event is the regeneration of the inferior alveolar nerve and the reinnervation of periosteum.11,12
Improvement in the bite force is a direct indicator of an improved function. In the present study there was no significant difference between the groups in terms of preoperative bite forces. The observation revealed significant improvement in the bite force in each patient of both the groups following fixation at every follow-up, which aptly favors the open treatment over close treatment of mandible fractures as early restoration of adequate function is one of the main goals of any fracture management.
In the present study, the preoperative mean bite force among group 1 and group 2 patients in the incisor region, left molar region, and right molar region was not found to be significantly different (Tables 1–3). At 6 weeks postoperative, 3 months postoperative, and 6 months postoperative, the mean bite force was found to be significantly higher among group 1 patients as compared to group 2 patients in all the sites (Tables 1–3). The findings suggest early restoration of improved function in terms of bite force in group 1 patients.
We observed a contradictory finding at 2 weeks postoperative follow-up when the mean bite force was found to be significantly higher among group 2 patients as compared to group 1 patients at the incisor region (Table 1). The possible explanation could be the increased inflammation and postoperative discomfort in group 1 patients, preventing them to bite harder due to pain or in anticipation of pain.
On comparison of the mean of ABF, RBF, and LBF, the bite force in the anterior and posterior regions were significantly increased from the sixth week postoperative to the end of the sixth month postoperative in every patient.
The selection of a suitable fixation device is one of the important factors that govern the successful outcome of the fracture management. Early restoration of function and improvement in the bite force is directly related to the type of fixation device used. The use of 3D locking miniplates resulted in significant improvement of the bite force at the incisor and right and left molar regions. Apart from significant improvement in the bite force, the other added advantages of locking miniplates (increased stability, better adaptation, and decreased chances of screw loosening) favor its use over standard miniplates.9,13
Conclusion
The bite force estimation is a useful parameter for judging the postoperative healing and efficacy of the masticatory system and thus a useful indicator of the treatment outcome. When compared with standard miniplates, 3D locking miniplates resulted in significant improvement in the bite force during the postoperative healing period.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.