
Abstract
Introduction
Post-traumatic headache (PTH) is a debilitating condition following traumatic brain injury (TBI), leading to chronic pain and a significant reduction in quality of life. Onabotulinumtoxin A (OnaBTX-A), widely approved for chronic migraine treatment, has shown potential in reducing headache frequency and intensity in PTH cases. Still, its efficacy remains less studied in this population.
Methods
This systematic review examines four case reports and series involving a variety of patient populations, including athletes, military personnel, gunshot survivors, and a patient with severe TBI. These studies collectively investigate the effectiveness of OnaBTX-A in reducing PTH symptoms.
Results
OnaBTX-A was consistently associated with symptom relief in patients with PTH. A 15-year-old athlete reported complete resolution of headaches and reduced reliance on pain medication after treatment. Three gunshot survivors with both PTH and cervical dystonia showed 70% to 100% improvement with sustained benefits over 90-day injection intervals. In a case series of 64 military personnel with mild TBI, 64% experienced symptom improvement, particularly in mixed headache types. A 62-year-old woman suffering from chronic PTH for 5 years post-TBI achieved full pain relief, with an associated resolution of the “iron band” sensation, significantly enhancing her quality of life.
Conclusion
OnaBTX-A demonstrates promise as an effective and well-tolerated treatment for chronic PTH across diverse populations. Further research is needed to refine treatment protocols, assess long-term effects, and explore its potential in complex cases, including those with persistent postconcussive symptoms or cervical dystonia.
This is a visual representation of the abstract.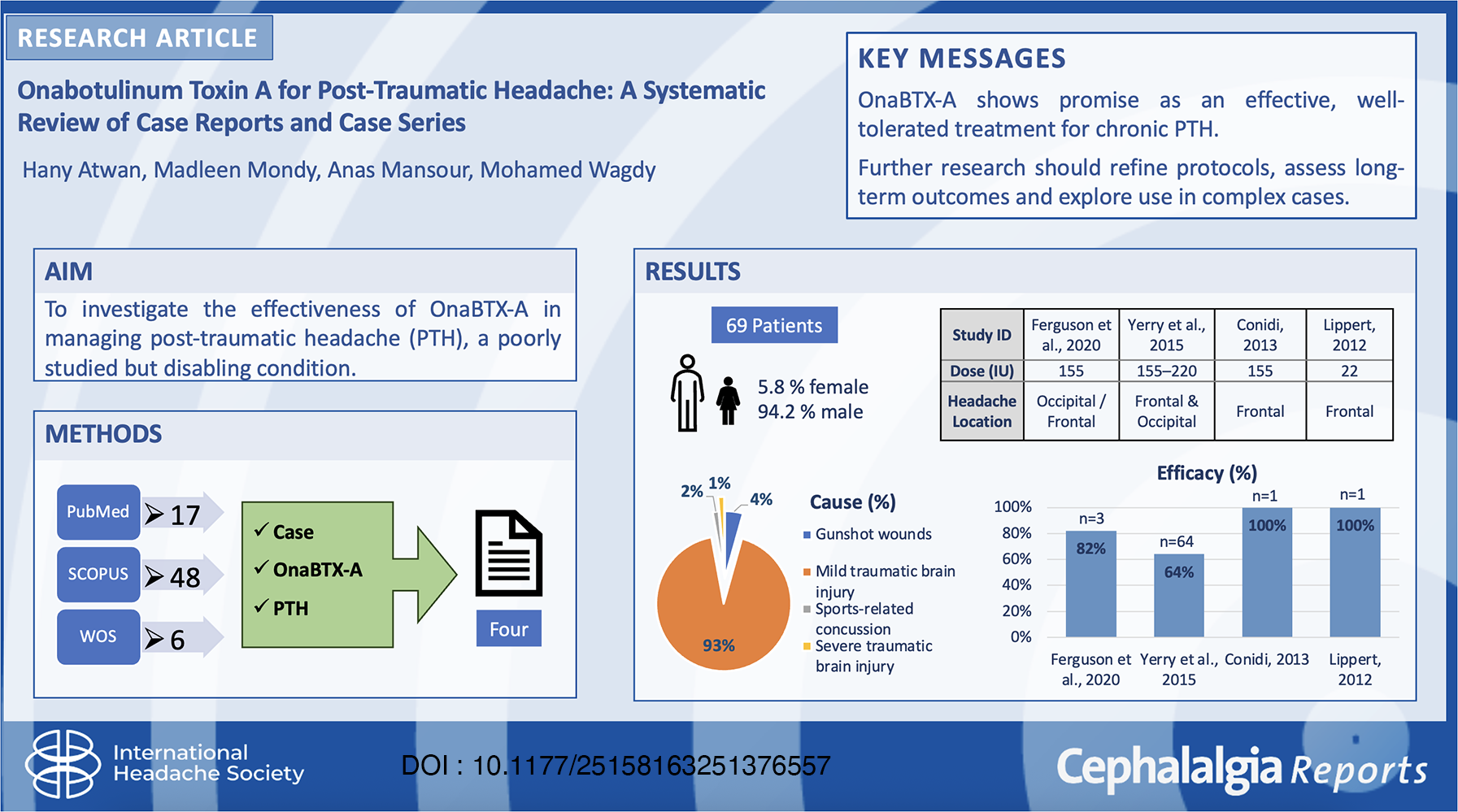
Introduction
Post-traumatic headache (PTH) is one of the most prevalent and debilitating sequelae following traumatic brain injury (TBI), affecting a significant portion of patients. Incidence rates of PTH range from 30% to 90% within the first year post-TBI, making it a major public health concern, particularly as TBIs continue to rise due to sporting accidents, traffic incidents, and military operations contributing to an annual global incidence of 42 million cases.1–5 PTH is highly variable in its presentation, often mimicking primary headache disorders such as migraines or tension-type headaches. 6 Chronic PTH, which persists beyond 1 year in up to 58% of individuals with acute PTH, can lead to significant impairment, mental distress, and reduced quality of life. 7
The pathophysiology of PTH remains incompletely understood, but several mechanisms have been proposed, including neurogenic inflammation, central sensitization, autonomic nervous system dysfunction, and neuroinflammation.2,8 Current treatment options primarily focus on symptomatic relief and include analgesics, antidepressants for comorbid mood disorders and chronic pain, antiepileptic medications to reduce neuronal hyperexcitability, and nonsteroidal anti-inflammatory drugs (NSAIDs) for acute pain. 3 However, these therapies often provide suboptimal outcomes due to limited efficacy, dose-limiting side effects such as sedation from antidepressants or gastrointestinal distress from NSAIDs, and a lack of standardized, PTH-specific treatment guidelines.3,8 Moreover, most available treatments aim to relieve symptoms rather than target the underlying neurological mechanisms contributing to chronic PTH.
Onabotulinumtoxin A (OnaBTX-A) has been used in headache disorders, primarily chronic migraine, but reports exist of its use in secondary headaches, including PTH.1,2 OnaBTX-A traditionally inhibits acetylcholine release at the neuromuscular junction, but it also affects neurotransmitters and neuropeptides involved in pain signaling and inflammation, such as substance P, calcitonin gene-related peptide (CGRP), and glutamate. These neuromodulatory effects contribute to reduced peripheral and central sensitization, key processes underlying chronic pain conditions like migraine and potentially PTH. Moreover, OnaBTX-A acts on nerves such as the trigeminal and cervical nerves, indicating that its analgesic effect is not solely due to muscle relaxation. When treating chronic migraine, a phenotype is frequently observed in chronic PTH. OnaBTX-A is typically administered in prescribed injections targeting specific muscles of the face, head, and neck. The administration of OnaBTX-A is relatively straightforward, requiring no specialized equipment or hospitalization, which enhances its practicality and accessibility for both clinicians and patients.
Recent studies have suggested that OnaBTX-A may provide relief for PTH, though the available literature remains limited and largely anecdotal.2,3 Furthermore, critical gaps persist in understanding optimal injection sites, dosing protocols, and long-term safety, as most data are extrapolated from migraine studies rather than PTH-specific trials.2,3 Additionally, the precise mechanism by which OnaBTX-A alleviates PTH, whether through inhibition of peripheral sensitization, suppression of inflammatory mediators, or indirect modulation of central pain pathways, remains unclear.9,10
This systematic review aims to synthesize the existing evidence on the efficacy and safety of OnaBTX-A for PTH. Specifically, we evaluate key treatment outcomes, including headache frequency reduction and pain intensity improvement. By consolidating data from available case reports, clinical studies, and trials, this review seeks to clarify the therapeutic potential of OnaBTX-A for PTH and identify key knowledge gaps requiring further research.
Method
Literature search
A comprehensive literature search was conducted using the PubMed, Scopus, and Web of Science databases, covering studies published from inception to February 2025. The search terms included “Onabotulinum Toxin A,” “post-traumatic headache,” “headache disorders,” “case reports,” and “case series.” Studies were considered eligible if they specifically examined the use of OnaBTX-A for PTH and provided sufficient clinical data for analysis. We conducted this systematic review and meta-analysis in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 9
Inclusion and exclusion criteria
The review's inclusion criteria consisted of individual case reports and case series, regardless of the number of patients included. Studies were required to report on PTH treated with OnaBTX-A and be published in English. Studies that did not meet these criteria were excluded. Specifically, nonhuman studies, reviews, and guidelines were not considered. Additionally, studies lacking follow-up data on treatment outcomes were excluded from the final analysis.
Quality assessment
The quality of the included studies was assessed using the Joanna Briggs Institute (JBI) critical appraisal tools for case reports and case series. 10 The JBI checklist for case reports evaluated study reliability based on criteria such as patient demographics, clinical history, diagnostic criteria, intervention details, and outcome measures. For the case series, the JBI checklist examined the inclusion criteria, consistency of measurement methods, completeness of follow up, and statistical analysis. Each study was scored, and only those meeting a sufficient quality threshold were included in the final analysis.
Data extraction
Data from the selected studies were independently extracted by two reviewers. Any discrepancies in the data collection process were resolved through discussion and consensus. The extracted data included details such as the author and publication year, patient demographics (age and sex), clinical presentation and headache characteristics, treatment protocols (including OnaBTX-A dosage and injection sites), and measured outcomes such as headache frequency, severity, and reported side effects.
Results
Study selection
A total of four studies were included in this review, comprising two case series and two case reports published between 2012 and 2020. These studies were identified after screening the relevant literature and evaluating eligibility based on the inclusion criteria. The PRISMA 2020 flow diagram illustrating the study selection process is shown in Figure 1.

PRISMA 2020 flow diagram.
Study characteristics
A total of four studies11–14 collectively reported on 69 patients with PTH who received treatment with botulinum toxin type A (OnaBTX-A). Sample sizes ranged from a single case report to a case series of 64 patients. The studies were conducted in the United States and Germany. The mean patient age ranged from 15 to 62 years, with gender distribution favoring males (65 males, 94%). Detailed study characteristics, including trauma type, headache location, and follow-up durations, are provided in Table 1.
Summary of included case series on OnaBTX-A for post-traumatic headache.

traumatic brain injury.
PTH etiologies included gunshot wounds, 11 sports-related concussion, 13 and blunt or blast injuries. 12 Headache onset varied from 48 hours to 28 years postinjury, with clinical features ranging from constant throbbing pain to chronic tension-type headache. Follow-up periods ranged from 10 to 90 days, though longer-term therapeutic cycles were also reported.
Clinical presentation and intervention
All included patients were diagnosed with PTH, commonly following traumatic brain injury (TBI), sports-related concussion, or military blast exposures. Headache onset ranged widely, from as early as 48 hours to as late as 28 years postinjury. While most studies described headache in general terms, one case report specifically identified temporal headaches following pterional craniotomy associated with temporal muscle hypertrophy. Headache locations varied, but most often involved the frontal, occipital, cervical, and temporal regions.
Treatment in all studies involved botulinum toxin type A (OnaBTX-A) injections targeting affected muscle groups, including the temporalis, frontalis, occipitalis, trapezius, and cervical paraspinal muscles. Dosing regimens varied: some studies used high-dose protocols (e.g. 155–220 units every 8–12 weeks), while others reported lower doses (e.g. 25–50 units) targeting specific muscles such as the temporalis. Treatment frequency ranged from single injections to repeated cycles administered over several months. Across all studies, patients experienced substantial to complete headache relief, often within 10 to 15 days of treatment initiation, and no serious adverse effects were reported. Treatment parameters and clinical responses are detailed in Tables 2 and 3.
Clinical presentation, intervention, and outcomes.

PTH: post-traumatic headache; TBI: traumatic brain injury.
Diagnosis, headache characteristics, treatment parameters, and clinical response.

Injection protocols
Follow-up periods varied across studies, ranging from 10 to 90 days. One study reported sustained headache relief and resolution of temporalis muscle hypertrophy, while other studies lacked detailed efficacy and safety assessments. 11
Intervention and efficacy
Across all studies, OnaBTX-A demonstrated consistent pain relief in patients with chronic PTH. In Ferguson et al., 11 patients reported 70% to 100% improvement in headache and neck pain. Yerry et al., 12 noted that 64% of patients improved with regular injections, experiencing both fewer headache days and lower pain intensity. Complete headache resolution was achieved in both case reports,13,14 including improved quality of life and symptom reversal. Pain relief typically began within 10 to 15 days postinjection, with some cases reporting sustained benefit lasting months.
Despite variations in protocols, most patients experienced moderate to significant clinical improvement, indicating that OnaBTX-A may be an effective option for treatment-resistant PTH.
Safety outcomes
None of the included studies reported serious adverse events. Minor side effects such as neck pain or headache exacerbation were reported in 13% to 18% of patients, 12 but these were transient and did not lead to treatment discontinuation. The overall safety profile was favorable across all studies, with no systemic complications or long-term harms reported.
Quality assessment
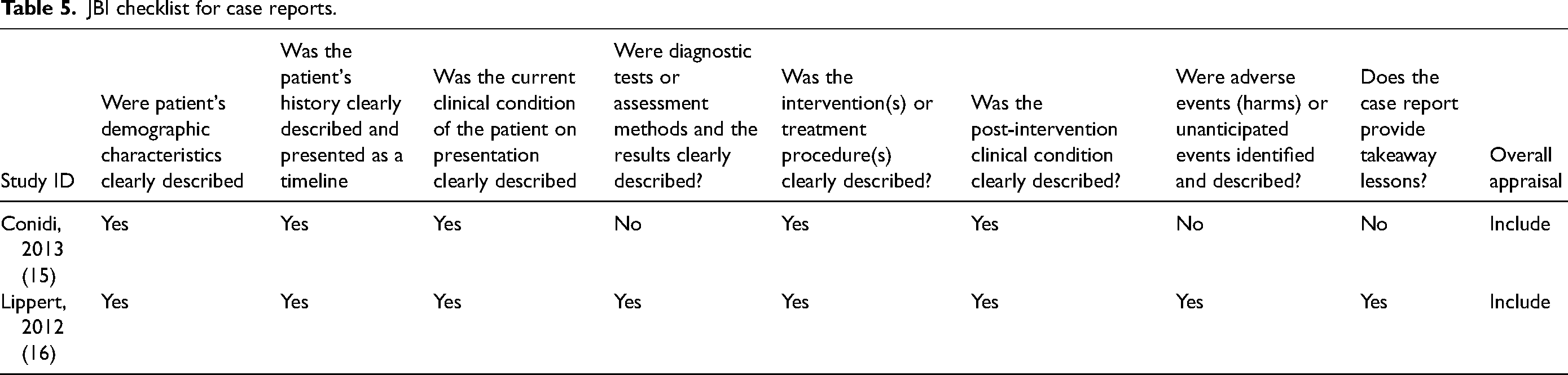
The JBI Checklist indicated that the included case series11,12 met key quality criteria, such as clearly defined inclusion criteria, consistent diagnostic approaches, and thorough clinical reporting, as shown in Table 4. In contrast, the case reports13,14 provided more limited information, with gaps in demographic and clinical data, as outlined in Table 5. None of the studies conducted statistical analyses, consistent with their descriptive design. Despite these methodological constraints, all studies were retained for analysis due to the overall consistent evidence supporting BoNT-A's potential efficacy and the need for future controlled studies.
JBI checklist for case series.

JBI checklist for case reports.
Discussion
Onabotulinumtoxin A (OnaBTX-A) has emerged as a promising therapeutic option for various headache disorders, including PTH. Initially introduced into clinical neurology following incidental cosmetic use in the early 1990s, OnaBTX-A has demonstrated efficacy in chronic migraine and related headache syndromes.15,16 Its mechanism of action extends beyond muscular relaxation: OnaBTX-A cleaves SNAP-25, a protein essential for synaptic vesicle fusion, thereby inhibiting acetylcholine release at the neuromuscular junction.16,17 Additionally, it modulates the release of pain-associated neuropeptides, such as substance P, glutamate, and CGRP, which contribute to peripheral sensitization, neurogenic inflammation, and nociceptive transmission.16,18 These neuromodulatory effects may underlie its potential benefits in headache types not solely attributed to muscular hyperactivity.
The administration of OnaBTX-A is relatively straightforward, requiring no specialized equipment or hospitalization, enhancing its feasibility in outpatient settings. Given the disabling nature of chronic PTH and the limited efficacy of conventional treatments, OnaBTX-A offers a practical and potentially effective alternative for patients with refractory symptoms.
Among the included studies, the most compelling data were presented by Ferguson et al., 11 who reported a 90% reduction in headache severity within 2 weeks of OnaBTX-A treatment, and complete symptom resolution following up to eight treatment cycles. Their findings support the use of OnaBTX-A for a subset of PTH cases related to craniofacial muscle dysfunction, particularly postcraniotomy headache due to temporalis muscle hypertrophy after pterional craniotomy.
OnaBTX-A is internalized by peripheral sensory neurons and undergoes retrograde axonal transport, potentially affecting second-order neurons in the central nervous system. This mechanism contributes to its long-lasting effects on neuronal excitability and central sensitization, both of which are hallmarks of chronic headache disorders.17–19 In parallel, OnaBTX-A has been shown to downregulate the expression of nociceptive ion channels such as transient receptor potential vanilloid 1 (TRPV1) and purinergic P2X3 receptors, thereby attenuating peripheral sensitization and reducing pain perception over time. 20
Despite its mechanistic plausibility, current clinical evidence for OnaBTX-A in the treatment of PTH is limited by methodological constraints. Most available data derive from case reports and small series lacking control groups, thereby introducing selection bias and limiting generalizability. Considerable heterogeneity in injection protocols, dosing regimens, and target muscle groups further complicates interpretation. Notably, while standardized injection paradigms such as the PREEMPT protocol, consisting of 155 units of OnaBTX-A injected into 31 sites across the head and neck every 12 weeks, are widely adopted in chronic migraine treatment, their applicability to PTH remains uncertain.15,16
In clinical practice, some physicians employ a “follow-the-pain” technique, whereby OnaBTX-A is injected into areas of maximal tenderness or hypertrophy. While this individualized approach may enhance symptom relief in selected patients, it may also yield variable cosmetic outcomes and contribute to the shifting of pain to previously unaffected regions.16,17 Moreover, the lack of validated outcome measures specific to PTH presents a challenge in objectively evaluating treatment efficacy. Although assessment tools such as the Migraine Disability Assessment (MIDAS), Short Pain Inventory (SPI), and SF-36 have been validated in chronic migraine populations, their utility in the postcraniotomy context has yet to be rigorously examined.17–19
OnaBTX-A is generally well-tolerated, with most adverse effects being mild and transient. These include localized injection site pain, muscle weakness, and transient neck discomfort. Serious complications such as anaphylaxis or systemic botulism-like symptoms are rare but necessitate appropriate clinical vigilance.16,17,20,21 Combination therapy with prophylactic agents, such as topiramate, sumatriptan, or rizatriptan, may further enhance therapeutic outcomes in patients with chronic headaches undergoing OnaBTX-A therapy.15,16 Observational studies have reported symptom improvement in 80% to 100% of patients resuming OnaBTX-A injections, underscoring its clinical utility in refractory headache cases.
Conclusion
This review underscores the potential role of OnaBTX-A in managing post-traumatic headaches. While the preliminary data suggest promising therapeutic benefits, further large-scale, randomized controlled trials are necessary to validate its effectiveness and establish standardized treatment protocols. OnaBTX-A's ability to target both peripheral and central pain pathways, coupled with its favorable safety profile, positions it as a valuable adjunct in postsurgical headache management. Continued research and refinement in clinical application may lead to more precise and effective utilization in neurosurgical recovery.
Clinical implications
OnaBTX-A offers a promising option for managing post-traumatic headaches, particularly in cases involving temporalis muscle hypertrophy.
Its minimally invasive nature and favorable safety profile support its use when conventional treatments are ineffective.
The dual action on peripheral and central pain mechanisms enhances its therapeutic value.
Individualized injection strategies may optimize outcomes, especially using the “follow-the-pain” technique.
OnaBTX-A can be integrated into a multidisciplinary approach to improve patient recovery and reduce headache-related disability.
Footnotes
Acknowledgments
The authors extend their sincere gratitude to all individuals who contributed to the development of this work.
Author contributions
HA conceptualized the study, designed the search strategy, supervised the project, and drafted the initial manuscript. MW contributed to the data extraction, quality assessment, and manuscript revision. AM contributed to data analysis, interpretation of findings, and manuscript editing. All authors read and approved the final manuscript.
Consent for publishing
All authors have reviewed and approved the final version of the manuscript and consent to its publication.
Data availability statement
Data extracted from the included studies and the PRISMA checklist are available upon reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Open practices
No software code or advanced data analytics tools were utilized in this narrative synthesis.