
Abstract
Background
Headache attributed to head injury is claimed to be among the most common secondary headache disorders, yet available epidemiological evidence is scarce. We evaluated the prevalence of headache among individuals previously exposed to head injury by a comparison to an uninjured control group.
Methods
This population-based historical cohort study used data from hospital records on previous exposure to head injury linked to a large epidemiological survey with data on headache occurrence. Participants without head injury, according to hospital records, were used as controls. The head injuries were classified according to the Head Injury Severity Scale (HISS) and the International Classification of Headache Disorders (ICHD-3 beta). Binary logistic regression was performed to investigate the association between headache and head injury, controlling for potential confounders.
Results
The exposed group consisted of 940 individuals and the control group of 38,751 individuals. In the multivariate analyses, adjusting for age, sex, anxiety, depression and socioeconomic status, there were significant associations between mild head injury and any headache, migraine, chronic daily headache and medication overuse headache.
Conclusion
Headache was more likely among individuals previously referred to a hospital for a mild head injury compared to uninjured controls.
Introduction
Headache is very common in the general population and constitutes a large social and economic burden for the global society as well as the individual (1,2). Headache can either be primary, for example migraine or tension-type headache (TTH), or it can be secondary to another disorder. Headache attributed to head injury (the latter referred to as traumatic brain injury (TBI) if the brain is affected), is among the most common secondary headache disorders (3).
Traumatic brain injury (TBI) is a common and important global health issue and a major cause of morbidity (4,5). Headache is the most common symptom following TBI (6–8) and is often persistent (6,9). It is reported that 18–22% of the headaches attributed to traumatic injury to the head (HAIH) last for more than one year (10,11).
HAIH is defined in the current version of the International Classification of Headache Disorders (ICHD-3 beta) as a headache disorder with no defining clinical characteristics that starts within seven days of trauma or injury or after regaining consciousness (3). HAIH is defined as persistent if it continues beyond three months.
Only a small number of studies using non-injured comparison groups have investigated the causal relationship between head injury and headache (12,13), and few of them have shown a dose-response relationship (14). It has also been shown that HAIH does not differ from migraine and tension-type headache (TTH) based on clinical characteristics (10). Consequently, some experts are disputing the existence of HAIH, arguing that it may be nothing other than a primary headache being misattributed to a head injury (15).
Available epidemiological evidence on HAIH is mainly based on studies with methodological limitations such as small samples with a high risk of selection bias, and varying case definitions for both head injury and HAIH.
In this article we present the findings of the so far largest controlled, population-based study on HAIH. We specifically investigated whether the prevalence of headache and its subtypes was higher among persons previously exposed to head injury and whether this was influenced by injury characteristics.
Materials and Methods
Study design
This is a historical cohort study. Data from hospital records on exposure to head injury during the period 1988–2008 were assembled and linked to a large epidemiological survey, performed between 2006 and 2008, with validated data on the occurrence of headache. Participants without head injury, according to hospital records, were used as a control group.
The HUNT3 survey
The third Nord-Trøndelag Health Study (HUNT3) was a cross-sectional study performed between October 2006 and June 2008. All inhabitants of Nord-Trøndelag County above the age of 19 were invited to participate. There were more than 200 health-related questions, and among them there were 14 headache questions designed to establish whether the participants suffered from headache or not, and to classify the headache according to the International Classification of Headache Disorders (ICHD-II) (16). Details of this comprehensive health study, including non-respondents, are described elsewhere (17,18).
Head injury data collection
Inhabitants in Nord-Trøndelag who had answered the 14 headache questions in HUNT3 and also been exposed to a head injury during the period 1988–2008 were identified in 2012 by a computer-based search. This was performed as follows: The national 11-digit identification numbers of all patients who had received one or more diagnoses related to head injury at the outpatient or inpatient wards at the hospitals in Nord-Trøndelag (i.e. Levanger and Namsos) or the nearest university hospital (St. Olavs Hospital in Trondheim, Sør-Trøndelag) during the time period 1988–2008 were registered. From the list of identification numbers, a data manager at the HUNT Research Centre identified all individuals who had answered the headache questions in HUNT3. Initially, all participants with head injuries that had received diagnostic codes from the International Classification of Diseases 9 (ICD-9) and 10 (ICD-10) referring to trauma to the body above the neck were included. Participants with diagnostic codes without assumed influence of brain function were later removed and the final selection was done by search for ICD-9 codes 800–804, 850–854, 920 and 925, and ICD-10 codes S02, S06, S07, T02.0–T04.0, and T06.0. Exclusion criteria were chronic subdural hematoma, no contact with the hospital in the first 48 hours after injury, and no matching information about trauma in the text of the chart or lack of signs or symptoms of head injury noted in the medical record.
Data regarding the head injuries were collected from medical records. This was performed by two medical students (LHN and TP) and an experienced research nurse (GBG) in close dialogue with a neurologist with expertise in epidemiology and headache (ML) and a neurosurgeon with expertise in head injury (AV). All available information in the medical records was scrutinized. A total of 38 variables were recorded for each head injury (Supplementary Table 1). If the same individual had more than one head injury, up to three of the most recent head injuries were recorded in chronological order. We recorded any CT, MRI or X-ray-imaging associated with the head injury within three months after the injury. Clear clinical signs of cranial fractures (hemotympanum, clear bleeding from the auditory canal and leakage of cerebrospinal fluid) were regarded as cranial fractures even without imaging evidence. The head injuries were classified according to the Head Injury Severity Scale (HISS, 19), and to the ICHD-3 beta, which contains a relatively detailed classification of the head injury associated with the headache (3). Because medical records often contain insufficient information to correctly classify injury severity (20), we used the term “most likely” in some categories in order to be able to describe the acute symptoms and signs and classify the injury.
Headache diagnosis in HUNT3
Individuals who answered “yes” to the first screening question “Have you suffered from headaches during the last year?” answered the subsequent thirteen headache questions in HUNT3 that enabled the report of definite migraine, probable migraine and tension-type headache (TTH), according to the ICHD-II criteria (16). The participants were also asked to state the consumption of analgesics and over-the-counter (OTC) drugs during the last month. This enabled the report of medication overuse headache (MOH). Participants fulfilling both TTH and probable migraine criteria were classified as TTH. Participants were not specifically asked about the duration of untreated headache attacks, due to the fact that some individuals always use attack medication for their headaches. Because of this, the ICHD-II criteria for migraine were modified so that duration of less than four hours was also accepted. Chronic daily headache (CDH) was defined as headache occurring >14 days per month. The ICHD-II criteria for MOH were slightly modified so that they were based on OTC-medications only. This was due to lack of information about prescribed analgesics and triptans. Medication overuse was defined as OTC-medication use for headache or pains in muscles and joints ≥4 days per week during the last month. MOH was defined as CDH with medication overuse. The validity of these questionnaire-based diagnoses has been reported previously (21). For any headache, the sensitivity was 88% and specificity 86% (kappa value 0.70, 95% confidence interval (CI) 0.61–0.79); for migraine, the sensitivity was 51% and specificity 95% (kappa values 0.50, 95% CI 0.32–0.68); for TTH ≥ 1 day/month the sensitivity was 96% and specificity was 69% (kappa value 0.44, 95% CI 0.30–0.58), and for MOH the sensitivity was 75% and specificity was 99% (kappa value 0.75, 95% CI 0.30–1.00).
Statistical analysis
Descriptive statistics (mean with standard deviation) and chi-square test were used to characterize the sample. In the multivariate analyses, using binary logistic regression, we estimated the odds ratios (OR) with 95% CI for the association between head injury and its subcategories and each category of headache. Head injuries were also stratified on the basis of when it happened (the 50% most recent, i.e. ≤10 years before interview, and the 50% earliest head injuries, i.e. >10 years before interview). Persons not suffering from headache were used as reference category. We initially adjusted for age (continuous variable) and sex, and subsequently for other potential confounding factors identified previously (e.g. smoking (yes/no), body mass index (BMI, continuous variable), and total Hospital Anxiety and Depression Scale (HADS) score (categorized from continuous variable into three categories with score boundaries ≤16, 17–21 and ≥22). Further, to adjust for socioeconomic status, we included information on occupation (ten categories) and reclassified the subjects into an approximation of the international social class schema by Erikson, Goldthorpe and Portocarero (EGP) (22,23). The participants were classified into three categories: high social class (EGP I-II), medium social class (EGP III-IV) and lower social class (EGP V-VII).
Covariates that did not substantially change the estimated ORs separately or together (i.e. less than 0.05) were excluded from the final model. This was the case for smoking and BMI. Subjects with incomplete data for the HADS score variable were nevertheless included, as a separate missing category, in all analyses to reduce the impact of response bias. In all analyses, two-tailed p-values were calculated and a p-value of 0.05 or less was defined as statistically significant. Statistical analyses were performed with IBM® SPSS® Statistics 21.
Ethical approval
The study was approved by the Regional Committee for Medical and Health Research Ethics and by the HUNT Research Centre.
Results
Participants
The flow of participants through the different stages of the study is presented in Figure 1. There were 25,760 registered hospital-referred head injuries at Levanger and Namsos hospitals and 119,402 at St. Olavs hospital in Trondheim during the 20-year period. Linkage of the patients’ national identification numbers to the HUNT database revealed that 2,889 of the persons with hospital-referred head injuries had answered the headache questions in HUNT3. Of them, 1,183 had a head injury with a diagnostic code reflecting assumed influence of brain function. Among these, 66 experienced their head injury after the HUNT3 survey and were thus not eligible, and 177 were excluded with regard to the exclusion criteria. The final exposed group (n = 940) and the unexposed group (n = 38,751) are presented in Table 1.
Flow of participants through the different steps of the HUNT3 headache survey and the different steps of identification of participants with head injuries. Demographics. BMI: Body Mass Index; HADS: Hospital Anxiety and Depression Scale. The HUNT occupational classification reclassified into Erikson, Goldthorpe and Portocarero (EGP) social class schema (23,24). Full-time household workers, students, militaries, persons receiving social security and persons with missing data.

Head injuries
Injury characteristics.

HISS: Head Injury Severity Scale; ICHD 3-beta: International Classification of Headache Disorders, version 3-beta.
Refers to number of head injuries and not number of patients.
If several head injuries, only first head injury is counted.
E.g. confusion, disorientation, slowed thinking, or somnolence.
After the head injury, a CT scan was performed on 40% (n = 380), an MRI on 1% (n = 6) and a plain X-ray of the head on 11% (n = 102) of the patients. The scans revealed traumatic pathology in 11% (n = 99) of all patients in the cohort. In total, 6.5% (n = 61) had intracranial pathology: 30 patients had only intraparenchymal lesions (22 patients had brain contusions, four had intracerebral hematomas, four had both brain contusion and intracerebral hematoma), 14 had only extraparenchymal hemorrhages and 17 patients had both. 7.7% of all patients (n = 72) had cranial fractures (revealed either by imaging or clinical findings), and 3.3% (n = 31) had both cranial fracture and intracranial pathology.
In the year 2000, new guidelines for initial management of minimal, mild and moderate head injuries were implemented in Norway advocating more liberal use of CT imaging of the head (24). During the period 1988 through 2000, 30% had a CT examination (n = 196 out of 643), while from 2001 the proportion was 62% (n = 184 out of 297). During the first time period, 6% (n = 37) of all patients had imaging evidence of intracranial pathology compared to 8% from 2001(n = 23), χ2 (1) = 1.346, p = 0.246.
Headache diagnoses
Prevalence OR with 95% CI of headache disorders related to earlier head injury.

Adjusted for age, sex, social class by occupation and HADS score.
Other headaches: headaches that are not possible to classify as either migraine or TTH. HISS: Head injury severity scale.
Number of patients, not of head injuries.
Prevalence OR with 95% CI of different frequencies of headache (disregarding diagnosis) related to earlier head injury.
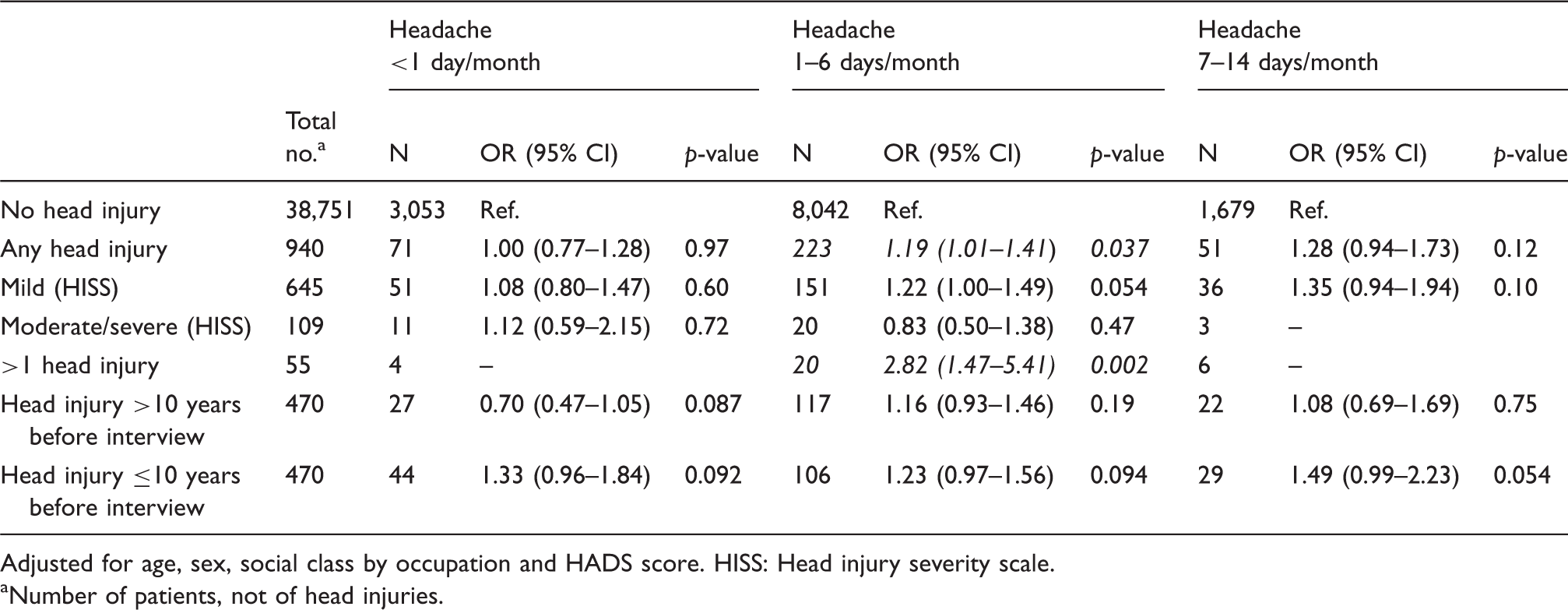
Adjusted for age, sex, social class by occupation and HADS score. HISS: Head injury severity scale.
Number of patients, not of head injuries.
Prevalence OR with 95% CI of chronic daily headache (CDH) (disregarding diagnosis) and medication overuse b headache (MOH) related to earlier head injury.

Adjusted for age, sex, social class by occupation and HADS score. HISS: Head injury severity scale. aHeadache on ≥15 days/month.
Medication overuse is estimated based on medications used for headache or pain in muscles and joints. cNumber of patients, not of head injuries.
Participants exposed to a mild head injury according to ICHD-3 beta had a significantly higher prevalence of migraine (n = 126 (17%), OR 1.58, 95% CI 1.27–1.97, p < 0.001), CDH (n = 32 (4%), OR 1.89, 95% CI 1.30–2.76, p = 0.001) and MOH (n = 16 (2%), OR 1.98, 95% CI 1.17–3.32, p = 0.010). However, they did not have a significantly higher prevalence of TTH (n = 127 (18%) OR 1.12, 95% CI 0.91–1.38, p = 0.30) or CDH without MOH (n = 14 (2 %), OR 1.72, 95% CI 1.00–2.98, p = 0.052).
Participants previously exposed to a moderate or severe head injury according to both classifications did not have a significantly higher prevalence of headache. The figures for the HISS classification are given in Table 3, and for ICHD3 beta classification the OR was 1.05 (n = 38, 95% CI 0.54–2.04, p = 0.89).
Relationship between acute symptoms, imaging findings and current headache
Prevalence OR with 95% CI of headache following head injury with or without proposed risk factors for headache.

Adjusted for age, sex, social class by occupation and HADS score. aOr most likely. bRefers to number of patients and not number of head injuries. cSubdural hematoma, epidural hematoma, subarachnoid haemorrhage and cortical contusions or intracerebral hematoma. Missing data are interpreted as not having the symptom or finding.
Discussion
In this large population-based study, the main finding was that headache suffering was more likely among individuals exposed to a mild head injury than those not exposed.
Our results contrast with a previous Norwegian population-based study with an uninjured control group, which did not find an association between previous head injury and headache (12). However, that study had low statistical power since only 192 patients and controls were included and the control group differed significantly from the exposed group with regard to several important confounders.
We found that the association between headache and head injury was evident only for those sustaining mild head injury. This is in accordance with several earlier studies (10,25), although the comparability is limited by different methods for classification of head injury severity. We used both HISS and ICDH-3 beta as classification systems, as HISS is widely used among neurosurgeons whereas ICHD-3 is used by headache specialists (5,24). Using ICHD-3 beta for classification of head injury severity in our analysis resulted in the same conclusions as for HISS, with the one exception that a significant association between previous mild head injury and CDH without medication overuse was no longer observed.
When classifying the headaches according to criteria for primary headache disorders, the higher occurrence of headache among individuals exposed to head injury was only evident for migraine, with the exception of TTH in the most recent injuries. This is in accordance with several studies published in recent years that report migraine as the most common headache phenotype after head injury (6,9,26,27). This is in contrast with earlier studies where TTH was reported as the most common (8,28,29).
Headache, nausea or dizziness at admission was associated with headache at the time of HUNT3, while alteration in mental state, cranial fracture, or intracranial pathology (traumatic lesions) was not. A study from 2002 found that the presence of nausea in the emergency room after mild TBI was strongly associated with the severity of most post-traumatic complaints, including headache, after six months, while headache and dizziness in the emergency room were not significantly associated. However, the study was small and did not have uninjured controls (7). Although headache, nausea and dizziness at admission may be consequences of the head injury, they can also represent an already existing primary headache disorder. Among some individuals with episodic migraine or TTH, the stressful circumstances of the accident and physical injury rather than the direct injury to the head may have triggered an episode of headache on the day of admission. Likewise, those with pre-existing CDH of any kind may have had an increased likelihood of reporting headache both at the day of admission and at follow-up even if there is no causal relationship with the injury to the head. In a study from 2005, Nestvold et al. (30) studied predictors of headache 22 years after hospitalization for head injury. They found no association between headache the first day after head injury and headache 22 years after the head injury. Cranial fracture seemed to be protective of long-term headache. We did not find cranial fracture to be either protective or a risk factor for headache.
Our study, and others like it, may be subject to a selection bias because individuals with headache and nausea after a head trauma may be more likely to seek medical advice and also to be referred to hospital. Since pre-traumatic headache seems to be a strong risk factor for headache after head injury (31), this may have contributed to our finding of a somewhat higher prevalence of headache after head injury.
Having had multiple head injuries increased the association to headache. This may represent a “biological gradient” in support of a causal relationship according to the Bradford Hill criteria (32). A recent study showed that soldiers with two or more mild TBIs experienced significantly more post-traumatic symptoms than those with a single mild TBI only (33). However, this may also be due to a reinforcement of the selection bias mentioned above. Another similar study could not confirm this phenomenon statistically (34).
The major strengths of this study were the population-based design, the large sample size, and the use of validated headache diagnoses. Selective participation in HUNT3 due to headache status seems unlikely, because the headache questions were a minor part of a survey with more than 200 health related questions. It was also an advantage that head injury was not mentioned in HUNT3, as this might have introduced a recall bias (e.g. those remembering their head trauma being more likely to recall suffering from headache). We had extensive objective and previously documented information on each head injury, retrieved from medical records, thereby eliminating recall bias. This also enabled us to classify most of the cases both according to HISS and ICHD-3 beta. We had information on medication overuse and were able to distinguish medication overuse headache from other chronic daily headache.
The study also has some limitations. We were not able to determine time of onset of the headaches. This has two consequences, the first one being that the headache could have been present already before the head injury. Secondly, we cannot determine if the onset of headache was within seven days after head injury, which is the criterion for classifying a headache as attributed to traumatic injury to the head, according to ICHD-3 beta (3). However, several studies have indicated that this criterion may be too strict (9,35). Moreover, patients with chronic headaches had to be pooled into one CDH category, because only seven persons with chronic migraine and 16 with chronic TTH had had any trauma. This sample size was too small for drawing statistical conclusions about possible associations to previous trauma. Since it is difficult in epidemiological studies to establish precise diagnosis among persons with very frequent headache, headaches occurring >14 days/month are often pooled into one category. However, the low number of events in some subgroups, (e.g. moderate/severe head traumas and subjects with headache >14 days/month), made it difficult to draw firm conclusions with regard to their associations, despite pooling headaches into one CDH category in this study. A further limitation was that medications other than OTC-analgesics could not be considered in the definition of MOH because there was no information available about triptans or other prescription drugs in the present HUNT dataset. Furthermore, when retrieving information about the head injury from medical records, there is a risk of not capturing relevant information. Missing data may have led to overrepresentation of certain symptoms because the physicians were more likely to make a note in the medical record of a present symptom than an absent one. However, the proportion of data missing was low (Table 2). Generalization of results should be performed with caution, since only 42% of the adults invited to HUNT3 answered the headache questionnaire. Furthermore, patients without referral to hospital were not captured, and those had presumably mostly minimal or mild head injuries and not moderate or severe head injuries. The results might have been different if we had been able to include all persons in the population with minimal or mild traumas, provided that there is, as we have argued above, a selective inclusion of persons in whom such events elicit headache. However, it is unrealistic to capture in a population-based survey all persons who do not seek medical help after a trauma. Finally, during the data collection, it was not registered which of the four exclusion criteria that was applied when persons were excluded.
In conclusion, the present study indicates that mild but not moderate or severe injuries are associated with persistent headache. It can, however, not be excluded that cases with mild head injuries already suffering from primary headache came to the hospital more often. A large cohort-study is needed to follow a population which is known to be headache free and explore whether subjects who are exposed to a head injury more often develop persistent headache than the surrounding population.
Headache has high personal and societal costs because it leads to absence from work and social activities and patients with mild TBI present daily at emergency departments (1,2). Headache attributed to mild traumatic injury to the head may thus be a significant public health issue, and it has also important medico-legal implications. Further epidemiological research aiming to elucidate whether there is a causal association is urgently needed.
Key findings
Headache suffering was more likely among individuals exposed to a mild head injury than those not exposed. The association between headache and head injury was not evident for those sustaining moderate or severe head injury. Migraine was the most common headache phenotype after head injury. Headache, nausea or dizziness at admission was associated with headache after head injury, while alteration in mental state, cranial fracture, or intracranial pathology (traumatic lesions) was not.
Footnotes
Acknowledgements
The Nord-Trøndelag Health Study (The HUNT Study) is a collaboration between HUNT Research Centre (Faculty of Medicine, Norwegian University of Science and Technology NTNU), Nord-Trøndelag County Council, Central Norway Health Authority, and the Norwegian Institute of Public Health.
Declaration of conflicting interests
No sources of funding were used to conduct this study. All authors have completed the Unified Competing Interest form at www.icmje.org/coi_disclosure.pdf (available on request from the corresponding author) and declare that (1) they have no support from any private company for the submitted work; (2) they have no conflicts of interest that are directly relevant to the content of this study; and (![]() ) their spouses, partners, or children have no financial relationships that may be relevant to the submitted work.
) their spouses, partners, or children have no financial relationships that may be relevant to the submitted work.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.