
Abstract
Introduction
Migraine has a substantial disease burden in Kuwait and Arabic Gulf countries. We aimed to report the epidemiology and burden of migraine, health system organization, barriers to migraine care, treatment patterns, and unmet needs to improve migraine care in Arabic Gulf countries.
Results
Migraine is the top disabler of all neurological conditions among all ages in this region. The healthcare infrastructure is generally well-developed, with access to both public and private healthcare services. In public service, patients with migraine are managed by a network of healthcare professionals composed of three levels: primary care physicians, general neurology clinics, and headache clinics. Subjects with migraine have access to a broad spectrum of migraine medications, including over-the-counter pain relief and prescription drugs like triptans. Advanced treatments such as onabotulinumtoxinA injections and monoclonal antibodies that focus on calcitonin gene-related peptide are also offered. Many migraine subjects explore alternative therapies that are rooted in traditional practices. Public awareness of migraine is growing in the Arabic Gulf countries, aimed at reducing stigma and improving understanding. There is a need to improve the education of general practitioners and increase the number of headache specialists in addition to improving the role of nurses in caring for migraine patients.
Conclusion
Modern medical practices, traditional beliefs, and a rapidly evolving healthcare landscape shape migraine in the Arabic Gulf countries. Subjects with migraine are encouraged to seek medical advice, explore treatment options suited to their needs, and actively participate in educational initiatives to better manage their condition.
This is a visual representation of the abstract.
Introduction
Region-specific studies on migraine management or socioeconomic impact in Arabic Gulf countries are scarce. Arabic Gulf countries are located in the Middle East. The Middle East is defined as a transcontinental region centred on Western Asia and parts of North Africa. It included countries such as Egypt, Iraq, Jordan, Lebanon, Yemen, and the Gulf Cooperation Council (GCC). 1 The GCC region involves navigating the unique cultural, environmental, and healthcare landscape of countries like Saudi Arabia, the United Arab Emirates, Kuwait, Qatar, Oman, and Bahrain. In GCC, common migraine triggers can include environmental factors such as extreme heat, humidity, and fluctuating air pressure. Lifestyle factors such as fasting during Ramadan, irregular sleep patterns, and dietary habits may also play a role. Limited awareness and fear of stigma may delay diagnosis and treatment.
This manuscript describes important and underreported aspects of migraine care in Kuwait and other GCC countries. It also offers insightful observations about current service structures and regional challenges.
Epidemiology and burden of migraine
The prevalence of migraine in the GCC countries is comparable to global averages, affecting 12–15% of adults; however, it is underreported due to stigma. Migraine has been prevalent in the Middle East for centuries. Various forms of headaches, including one-sided headaches, are mentioned in ancient Egyptian papyri. 2 The oldest known medical manuscript, the Ebers Papyrus (dating back to about 1200 BC and discovered in the necropolis of Thebes), contains an ancient Egyptian prescription for migraine based on earlier medical documents, including an Egyptian papyrus of 2500 BC. 3 In the book Canon of Medicine by Ibn Sina (Avicenna) (980–1037 AD), Avicenna discussed the pathogenesis and treatment of migraine. 4 Migraine prevalence among the general population in GCC countries was estimated in different studies and showed a range between 2.6% and 78.5%,5–8 although they share the same culture, economics, ethnicity, and hot climate.5,9,10 The high prevalence of migraine in some GCC countries may be related to the high consanguinity rate since migraine is believed to have high genetic factors. 11 Earlier epidemiological studies in GCC countries estimated that the prevalence of migraine ranged from 2.5% to 10%8,12; however, some more recent studies have found higher migraine prevalence estimates of around 25%.13–16 Hence, migraine may be more prevalent in the GCC countries than previously believed. This change is likely due to increasing knowledge, earlier diagnosis of migraine, and conducting better epidemiological studies. In GCC countries, migraine was found to be more widespread in women than men as well as more predominant in the urban population. Furthermore, it potentially influences the daily life activities of the patients, including social occasions, employment, and schooling. 7 Prevalence of migraine studies from GCC countries confirms a high prevalence of migraine during the most economically productive years of life, and episodic migraine is more commonly diagnosed than chronic migraine.13–17 In a cross-sectional community-based study conducted in Kuwait, it was noted that the prevalence of migraine peaked in young adults between 18 and 30 years (70.8%) and then slightly declined among age groups 31–50 years. And dropped to its lowest level in a group of patients aged 50 years or more (20%). The female-to-male ratio was 2:1 in migraine. 13 In a community-based study, migraine prevalence was 10.9% among the pediatric and adolescent population of Kuwaiti children aged 6–17. The students with headaches lost a mean of 1.29 + 1.23 days of school and reported a mean of 1.16 + 1.50 days; they could not do activities they had wanted to. Parents lost an average of 1.01 + 1.02 days of work due to their children's headaches during the four weeks prior to the study. 18 Migraine prevalence among school children aged six to eighteen in GCC countries ranged from 7.1% to 20.1%.19–23 In a Kuwaiti study, migraine was significantly higher in girls compared to boys among middle schoolers; however, no significant difference between genders was noted among primary school students. 23 Postpubertal females are at higher risk of developing primary headaches compared to prepubertal females. 24 Migraine prevalence among medical university students in GCC countries ranged from 12.2% to 27.9%.25,26 Migraine in Kuwait and other GCC countries has a significant negative impact on daily activities, schooling/employment, social occasions, and the quality of life (QoL) of patients. 16 In GCC countries, Muslims traditionally observe dry fasting throughout the entire month of Ramadan each year. Fasting is one of the five pillars of Islam and a vital part of the Islamic religion. Muslims fast from dawn until sunset, during which they must refrain from all foods and drinks. Fasters will have two main meals during the day, one after sunset and one just before dawn. They partake in several prayers during the night, which will result in a change in their sleeping patterns. A Kuwaiti study reported that migraine frequency and severity worsen during Ramadan fasting. Changes in sleep and food habits, along with dehydration, make migraine worse. 27 A favorable and effective prophylactic treatment should be started a few months before Ramadan for better outcomes.
Consultation and health system organization
According to the World Health Organization's 2011 Atlas of Headache Disorders, it is estimated that around half of people with headaches are primarily self-treated, with only around 10% being treated by neurologists. 28 Primary care settings typically manage migraine.29,30
Governmental and private sectors divide the healthcare system in GCC countries. Governmental hospitals serve the majority, while the private sector typically covers expats with insurance. In the governmental sector of GCC countries, patients with migraine are managed by a network of healthcare professionals composed of three levels: primary care physicians, general neurology clinics, and headache clinics (Figure 1). In the private sector, patients can directly consult any physician without the need for a referral.

Journey of migraine patients in GCC.
Thirty percent of primary care doctors and thirty-four percent of neurologists worldwide consult about migraine. 28 In GCC countries, many of the headache patients are seen by physicians other than neurologists, who could be a family doctor, ophthalmologist, otolaryngologist, cardiologist, internal medicine physician, vascular surgeon, neurosurgeon, gastroenterologist, physiotherapist, alternative medicine practitioner, or others; this could lead to a proper treatment gap. 31 This underscores the limited understanding of migraine characteristics among the GCC population. 31
In Kuwait, patients experiencing headaches first consult a general practitioner in primary care. Some of them are referred to neurologists in general hospitals. Their neurologist rarely refers patients to Kuwait's extremely limited specialist headache clinics. The scarcity of specialized headache physicians explains the limited number of specialized headache clinics in Kuwait. Neurologists refer some headache-afflicted subjects to other specialties. Some general practitioners in primary care fail to recognize migraine, which explains this trend.
In a community-based study in Kuwait, general practitioners (GPs) were the ones who managed 67% of our headache patients. This high percentage points to the importance of adequate education of general practitioners about headache diagnosis and management to avoid headache under-recognition and chronification of headache. 13
Another community-based study to assess migraine burden in Kuwait reported that most of the migraine cohort (64.4%) sought medical advice with respect to their migraine, and the majority (62.4%) were seen by GPs, while only 17.2% were assessed by neurologists and 3.7% were examined by other specialties. Misdiagnosis of tension-type headaches and sinus-related headaches occurred in 8.9% and 2.1% of migraine subjects, respectively. 16 Another study 18 reported that 67% of the pediatric population utilized medical care.
Patients with migraine in governmental hospitals in the GCC region often have to wait six to twelve months to see a neurologist. 32 This is longer when compared to the global average wait time, which was estimated at 3.7 months for the first visit and 2.5 months for the follow-up visit. 33
The GCC region lacks certified headache medicine specialists and adequate headache clinics to which referrals can be made for the diagnosis and management of various types of headaches, including chronic migraine and medication overuse headache. 32
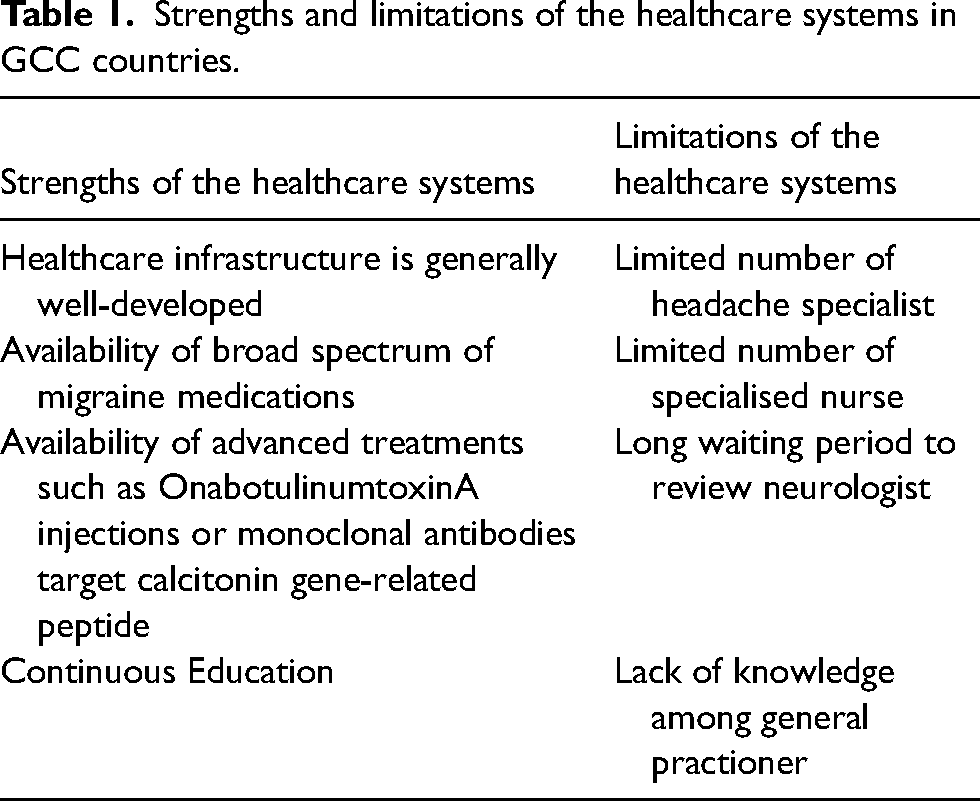
The specialized headache clinic accepts a limited number of patients. The longer duration of patient visits, compared to those at other clinics, explains this. The delay could be a consequence of a different patient pool, more patients with chronic migraine, and the higher level of specialized visits performed in these clinics. Table 1 displays the strengths and limitations of healthcare systems in GCC countries.
Strengths and limitations of the healthcare systems in GCC countries.
Evidence-based migraine treatments available in Kuwait.

Access to diagnostics, care, and barriers
Migraine is still an underdiagnosed and undertreated health problem. Its impact on patients is underestimated.5,32,34 The prevalence of hidden migraine among the previously studied sample was 31.7%. 34 Diagnosis delay was reported to be 6–15 years across the migraine patients in Gulf countries. 35 It was reported as 7.75 (1–38) years in Kuwaiti patients with migraine. Some of them were misdiagnosed as sinusitis and underwent sinus surgery. 36 In another Kuwaiti study, although the majority were seen by their general practitioners, only 4.6% received an accurate diagnosis of migraine. 16 A study done in Jeddah showed that primary care physicians had low knowledge levels and inappropriate attitudes toward chronic migraine. 37 The primary care physicians referred only 54.49% of (migraine) patients to a neurologist, indicating poor referral. 37 Another factor contributing to the misdiagnosis of migraine is that they can sometimes be associated with white matter hyperintensities (WMHs), leading to their being misdiagnosed as multiple sclerosis. Previous studies in Kuwait reported that 40% of migraine patients had WMHs. 38 A previous study from the Middle East misdiagnosed 14.7% of migraine patients as having multiple sclerosis. 39
Patients with migraine in a previous study in GCC countries believed that there are too few physicians who specialize in treating migraine and that emergency departments should have a migraine specialist so that severe migraine attacks are better treated. 32 Patients in public systems in GCC countries take too long to obtain an appointment. 32 However, because of the self-referral system used in most private hospitals, patients decide which specialty they need to visit, and, presumably because of poor awareness of migraine features, 31 many patients access other specialties before finally seeing a neurologist or headache specialist. 32 In the private sector, patients have direct access to specialized physicians. They do not need a referral from GPs. Self-referral is not reimbursed by insurance. It is the patient's choice.
In Kuwait, patients waited one to three months for a first visit and three to four months for the follow-up visit. The long waiting lists might be due to patients with less common migraine being referred incorrectly, not having a system to prioritize patients, not having enough resources for migraine care, not having enough delegation of tasks, and poor management of follow-up visits. The demand for neurologists’ services exceeds their availability. In Kuwait, a ratio of one neurologist per general population is very low. The number of neurologists is 70, and the general population is 4.850 million. There are only two headache specialists in Kuwait. Additionally, the excessive referral of patients to specialized tertiary centers is a common cause of inflated wait lists. Unavailability of migraine-specific treatment in primary care services is another cause of excessive referral.
Patient prioritization triage and patient prioritization are performed for urgent cases, such as patients with acute attacks or with suspected tumors or strokes, thus avoiding the waiting list. There is a need to perform more advanced triage to differentiate access priorities among non-urgent cases, which represent most patients. Consequently, such procedures help guarantee access for severe cases and limit waiting lists for patients with chronic migraine or more complex cases.
Delays in diagnosis in our region are explained by lack of physician knowledge, patient unawareness, and lack of a proper health infrastructure that affects the patient journey. To improve the attitude towards referral and treatment, primary care physicians and other medical specialities must increase their awareness. 39 The knowledge gap among non-neurologists impacts the management of migraine patients and interferes with reaching a proper diagnosis. 31
Another barrier to delayed diagnosis is the traditional beliefs related to headache. Some subjects believe that such sickness in the head is from Jin/devils; they prefer to treat it with the Holy Quran. Also, some subjects think that their headache is due to what is called Farry. They define Farry as an opening or a gap in the skull that would allow air to circulate inside, causing chronic headaches. Therefore, they treat headaches with head banding or tying the head with a cloth to reduce the pain. Relief of pain is explained with the reduction of blood flow during migraine attacks.
Few patients feel a stigma with migraine. Especially women prefer not to disclose their disease to their husbands and feel a stigma with migraine. Fear of stigma delays diagnosis and treatment.
Another barrier to patient care is some patients having to pay for treatment because of insurance limits. Some insurance companies do not consider migraine a disease. Patients also experience difficulties accessing novel class-specific medication due to public hospitals in the GCC region generally not including these medications in their formulary. A plausible reason is that decision-makers lack awareness of the severely disabling effects of migraine and hence the need for effective therapies. 32 Reimbursement is a major issue for novel migraine treatments. These drugs are currently unavailable in most regions of the world, including the Middle East, and they are unlikely to be reimbursed in the near future in most healthcare systems that are not prepared to sustain their high costs. These novel migraine treatments are available at governmental hospitals for citizens in the GCC. Private insurance should cover these medications for expatriates. Not all insurance companies accept migraine treatment reimbursement.
The evaluation of migraine subjects does not involve the nuances of the patient-doctor relationship or the elicitation of a history. The conversation is straightforward without difficult terminology.
The headache clinic and most neurology clinics in this region strictly adhere to international guidelines for diagnosis and treatment. The delayed diagnosis and improper management of migraine are common among patients and physicians. The gaps in critical knowledge among physicians have been found to be an issue in the GCC, which could be a contributing factor to migraine being misdiagnosed. Addressing these regional challenges may help policymakers improve early migraine diagnosis and enhance the quality of patient care.
GCC countries face some barriers to patient care during their journey. These barriers include long waiting periods for patient care, limited access to specialised centres, lower levels of patient awareness, insufficient evidence of headache symptoms, a lack of awareness of headache guidelines among health practitioners, and shortages of dedicated nursing staff.32,35,40 Addressing these barriers is crucial for improving the diagnosis rate, enhancing the quality of patient care, improving health outcomes, and improving the migraine patient journey. 40
Treatments of migraine (acute and preventive)
Currently, most countries in the Middle East lack specific guidelines for managing migraine. 40 Subjects with primary headache manage their headache by self-medicating, mainly with conventional over-the-counter (OTC) analgesics. 17 The World Health Organization's (WHO) Model List of Essential Medicines includes acetylsalicylic acid, ibuprofen, paracetamol (acetaminophen), sumatriptan, and propranolol. 41 All these medications are available in our region. Table 2 displays available medications for migraine in Kuwait that range from simple analgesics to novel therapies and migraine-specific drugs. 42
Treatment strategies for migraine in our region include both acute and preventive medications for mitigating migraine attacks, alleviating pain, managing comorbid conditions, minimizing disabilities, and restoring function.43,44 Preventive treatment helps to lower how often and how badly migraine attacks happen and includes antiepileptic drugs, beta-blockers, antidepressants, serotonergic antagonists, calcium channel antagonists, angiotensin modulators, and nutrients and herbal products.
The latest guidelines from the American Headache Society (AHS) suggest using triptans, gepants, NSAIDs, antiemetics, combination pain relievers, CGRP antagonists, and selective serotonin agonists to treat migraine attacks quickly. The 2024 consensus from the United Arab Emirates (UAE) on the acute management of migraine recommends using analgesics, primarily NSAIDs, along with migraine-specific treatments such as triptans, gepants, or ditans. This approach follows a stratified patient-centric model that considers migraine severity, the patient's comorbidities, and any contraindications to other medications. 45 For the management of acute migraine attacks in Kuwait, we follow the International Headache Society's global practice recommendations for the acute pharmacological treatment of migraine. 46 Multiple drug classes and individual drugs are available for the acute treatment of migraine attacks in Kuwait. These include simple analgesics (e.g. paracetamol or acetaminophen); NSAIDs such as ibuprofen, acetylsalicylic acid, diclofenac, or naproxen; and migraine-specific drugs such as triptans. Triptans that are available in Kuwait are sumatriptan, zolmitriptan, frovatriptan, eletriptan, and rizatriptan. NSAIDs and paracetamol are less expensive and generally more widely available than triptans. Ergots are no longer prescribed for outpatients due to side effects, risk of overuse, and availability of safer options. It can be prescribed for inpatient use as 1 mg intravenously in certain situations, such as status migrainous. They can only be used when all acute treatments are ineffective or contraindicated and ergots are not. Migraine patients who don't respond to NSAIDs should be evaluated for triptans. They should be referred to secondary care because triptans are only available in the hospitals, not in the primary care facilities. Triptans are free for citizen patients. Expats got it from private hospitals after evaluation by a neurologist or physician. The expat should pay if it is not covered with insurance. Acute treatment strategies include stepped or stratified care. Step care escalates treatment across or within attacks according to the treatment response, safety, and costs. In stratified care, treatment selection is based on the assessment of disorder severity. Stratified care may lead to more effective acute treatment and is more cost-effective due to a decrease in physician office visits, emergency department visits, and medical procedures.46–48 Nausea with headache attacks is treated with antiemetics such as metoclopramide and prochlorperazine (Table 2).
There are various types of medications for preventing migraine in our area, including blood pressure medications, anti-seizure drugs, antidepressants, monoclonal antibodies that target the CGRP pathway or receptor, and onabotulinumtoxinA. UAE consensus in 2024 for preventive management: CGRP monoclonal antibodies are considered the first-line therapy. However, if the patient has been on continuous CGRP monoclonal antibodies for 12 months, a pause in treatment is ideal. 49 Reimbursement issues significantly affect certain populations seeking novel headache treatments, including ditans and drugs that target the CGRP pathway. In Kuwait, we follow guidelines from the International Headache Society's Global Practice Recommendations for Preventive Pharmacological Treatment of Migraine. 50
Migraine preventive medications are offered for migraine patients with two to four days with migraine per month whose migraine attacks cause disability and are not quickly responsive to acute migraine medications, migraine with attacks associated with prolonged and severe auras, acute migraine treatment that is not effective, or the subject has contraindications to their use. Other indicators for initiating preventive treatment are people with migraine overusing acute medications, as well as those who are at risk of medication overuse, absences from work or school due to migraine, and substantial negative impact on daily routines. The decision to initiate preventive treatment is a shared decision-making process between physician and patient. Shared decision-making is common practice in Kuwait and other GCC countries. We should discuss and carefully consider the potential benefits, side effects, and risks associated with the use of preventive medications. The discussion and decision-making process should encompass the potential benefits, side effects, and risks of preventive medications, as well as patient-specific factors including age, child-bearing potential, existing health conditions, possible medication interactions, and the ability to follow the medication dosing schedule. 46
The choice to begin a preventive migraine medication should take into account various factors, such as how often and how severe the migraine attacks are, how long they last, if there are other types of headaches (like tension-type headaches), how much the migraine affect daily life, how well the current medication works, how often it needs to be taken, and what the patient prefers. When prescribing migraine treatment, comorbidity is considered, including conditions such as hypertension, depression, or epilepsy. We may choose one treatment for both conditions at that time. Table 2 displays available preventive treatment in our region.
Comorbidities like anxiety, depression, and insomnia sometimes require the help of a psychiatrist for behavioral services, which are available in most hospitals. Many patients and their families decline referrals to these services.
In women with menstrual migraine, we prescribe non-steroidal anti-inflammatory drugs or triptans as first-line drugs. The combination of triptans with non-steroidal anti-inflammatory drugs, or triptans with antiemetics, as well as non-steroidal anti-inflammatory drugs with antiemetics, can be used in case of failure of individual drugs. If the previously mentioned treatments are ineffective, we recommend short-term prevention with naproxen or frovatriptan for women with regular cycles. Mefenamic acid is also considered for menstrual migraine. 51
If the earlier treatments don't work, hormonal treatment using a steady dose of combined hormonal contraceptives or just progesterone contraceptives can be an option for migraine without aura, along with starting regular preventive treatment sooner. Short-term prevention should be started 2–3 days prior to the first day of menses and continued during menstruation.46,47
In Kuwait, a study that looked at patients with episodic or chronic migraine who were treated with erenumab found that they had fewer headaches, less pain, used less pain relief medication, and felt better overall. A study of migraine burden in Kuwait reported that the majority (94.6%) of migraine subjects used symptomatic drugs for headache attacks, whereas 39.9% were taking preventive medication. 23
The majority (95%) of the paediatric migraine patients received symptomatic drugs for headache attacks, and only 7.5% used preventive medication. 3
OnabotulinumtoxinA is approved in Kuwait and other Middle Eastern countries for the treatment of chronic migraine. The evidence is based primarily on one positive study (PREEMPT 2) and on the pooled analysis of two studies (PREEMPT 1 and PREEMPT 2).52,53 In an earlier study in Kuwait, 75% of patients with chronic migraine treated with onabotulinumtoxinA (BoNT-A) improved. Patients assessed at the 4th, 8th, and 12th weeks following BoNT-A injection showed significant improvement in all outcome measures compared to baseline. There was an improvement in the total number of moderate-to-severe headache days, the number of migraine days, and analgesic consumption. The total scores of the Headache Impact Test-6 significantly improved compared to the baseline. 54 In one recent study in Kuwait, BoNT-A was an effective and well-tolerated therapy in the prophylaxis of episodic migraine. It dramatically decreased the burden of migraine, the frequency of migraine days, and the use of acute medicines. With BoNT-A treatment, disability and quality of life significantly improved. 55
Traditional and alternative medicine
Traditional medicine (TM) is widely used for primary headache disorders in GCC countries. The prevalence rate of TM use in the Gulf is high. It is 70% in Kuwait, 56 67% in the United Arab Emirates, 57 and 42% in Saudi Arabia. 58 TM is sometimes used instead of conventional medicine and may lead to a delay in the diagnosis and proper management. 56 Cultural and religious beliefs were the reasons for seeking traditional medicine (TM) in 51.3% of cases, while 10% sought it due to ineffective medical treatment and 8.6% did so because they were intolerant of medical treatment. 56 Popular treatment based on the Qur’an and the Sunna of the Prophet Muhammad continues to be practiced in Muslim countries due to religious inspiration. 59 Hijama was the most commonly used TM for primary headache, in 65.6% of the Kuwait cohort. 56 The religious roots of hijama stem from the fact that the Prophet Muhammad (peace be upon him) recommended it for curing illnesses. 60 The Arabic word ‘hijama’ is often translated into English as ‘cupping.’ Hijama is a type of blood cupping, which is also known as wet cupping. 60
Other TMs that are used in Kuwait for headaches include Sabkha, herbal remedies, head massage, and diet modification. Sabkha (aka Labkha) is an herbal mixture that includes henna, prepared by a specialised person and applied to the head and left for a few days. 61 Headbanding, or tying the head with a cloth to create pressure around the head to reduce the flow of blood to the scalp, can help to relieve the pain caused by swollen blood vessels. Application of an ice pack and local scalp pressure are the most used non-pharmacological methods for temporary relief of (migraine) pain. 62
The Canon of Medicine, written by Ibn Sina, described local treatment of migraine. 4 Ibn Sina's local treatments for migraine included cupping, cutting veins in the forehead and temples, using a local aloe solution, and applying peppermint, Haltit (Ferula asafetida), Sakbing (Galbanum ferula galaniflua), or pepper extract like capsaicin.
Neuromodulation, including transcranial magnetic stimulation and noninvasive Vagus nerve stimulation is unavailable in Kuwait. However, some patients bought the device Cephaly, and they are happy using it.
Education and professional training in migraine
Numerous scientific activities aim to educate physicians on various types of headaches, their diagnosis, management strategies, and the international guidelines for migraine diagnosis and treatment. Every two years since 2012, Kuwait has hosted the crucial headache session at the Kuwait-North America conference. Since 2023, the Kuwait Neurological Society has held Headache Day annually for educational purposes. Several countries in the region engage in similar activities. The Kuwait Neurological Society is conducting continuous education activities for neurology residents as well as for the primary healthcare system. The curriculum for medical students includes undergraduate lectures on headache diagnosis, differential diagnosis, and treatment. Updated knowledge from the undergraduate programs emphasizes the value of migraine prevalence for improving management and reducing migraine burden. Neurology and internal medicine residents have an educational program on headaches. Medical students and residents attend neurology and headache outpatient clinics during their neurology block to gain experience in assessing headache cases and their management. Unfortunately, the GCC region lacks certified headache medicine specialists.
Policy and advocacy
Advocacy strategies are applied to create awareness about the impact of migraine on individuals, their families, and the economy. These strategies also help secure funding for research and improve access to medication.
There are booklets that are created and distributed to migraine patients during their visits to the headache clinic. Additionally, social media in the region spreads knowledge to the population about migraine symptoms, diagnosis, and available treatments.
Patient advocacy groups and societies are being established to empower individuals with migraine by amplifying their voices, supporting their journeys, and advocating for the Ministry of Health to reimburse their migraine medications.
Patient support and advocacy groups have an important role in patient education and awareness about symptoms, triggers of migraine, and effective self-care strategies and help them improve their daily activities and quality of their lives.
The government needs to create policies that make it easier for people to acquire treatment by developing specific plans and guidelines for headache care at all levels of health services.
Health authorities consider the insurance coverage and socioeconomic status of patients and take adequate measures to improve access to health care infrastructure, specialised centres, and the availability of novel treatments.
Future directions
Research is needed on biomarkers that predict treatment response and potential adverse events. Future genetic migraine studies in our region are required because of the higher consanguinity there. Also, future studies should focus on detecting the reasons for migraine underdiagnosis and why positive cases don’t seek medical advice despite their symptoms and disability.
A digital solution could improve patient management and transform the hospital patient experience, for instance, by engaging patients during the wait time and reducing visit time by completing patient history and questionnaires. Well-designed epidemiological studies involving Arab nations will further aid learning more about this condition. Future longitudinal studies are necessary to explore the prognosis and predictors of chronicity in Arab countries, aiming to yield more precise results. Future studies should focus on detecting the reasons for migraine underdiagnosis and why positive cases don’t seek medical advice despite their symptoms and disability. Innovative technologies are transforming headache medicine, with digital resources, telehealth, mobile apps, wearables, and artificial intelligence enhancing patient care and improving health outcomes. The introduction of digital technology in headache management represents a vital advancement, especially given the global burden of migraine and the limited availability of specialists. These supplementary tools facilitate the customization of treatment plans, paving the way for an era when healthcare provision is increasingly accessible, efficient, and patient-centered. Increasing numbers of headache specialists and specialized clinics will reduce the burden on healthcare settings and allow better management of migraine headaches. Our region limits the role of nurses in migraine management. There is a need to identify opportunities to improve and reevaluate the role of nurses in caring for patients with migraine. They should have an important role in patient education, such as explaining the migraine diary to the patients, patient compliance with the migraine diary, and triggers of migraine. In specialized clinics, nurses should have a higher level of delegation and involvement in patient care. They should be more involved in specialists delegating more tasks, such as preliminary visits, remote follow-ups, and treatment administration support. These recommendations cannot be applied to all countries in the Middle East. This depends on each country and the available sources. Not all the countries are at the same level; everyone should work on the most vital point to improve migraine diagnosis and treatment. There are no studies on the cost of migraine, either direct or indirect, in GCC countries. Studies on the cost of migraine are planned.
Additional suggestions
We need reliable measurement of migraine disability, referring to interictal periods during which patients also suffer negative effects of the migraine. There is a need to operationalize scales and coefficients that will enable the objective measurement of headache-related disabilities in both populations and individuals.
Strengths and limitations
The strength of this paper is that it provides a comprehensive review of migraine care in the Middle East. It addressed a significant gap in the literature by summarizing epidemiology, barriers to care, service delivery, access to treatment, and traditional medicine practices unique to this region. The manuscript provides advantageous suggestions for clinicians, policymakers, and researchers interested in regional disparities and healthcare challenges in headache medicine. A limitation of this paper is its primary focus on Kuwait.
Conclusion
Migraine has a substantial disease burden in the Middle East. Migraine is still underdiagnosed and undertreated in Middle Eastern countries. Region-specific migraine guidelines are not available for most countries within the Middle East region. Evaluating various aspects of the migraine patient journey may help bridge gaps in care and enable clinicians to make informed decisions in routine clinical settings. There is a network of healthcare professionals composed of three levels: primary care physicians, general neurology clinics, and headache clinics; the structure is limited by the lack of nursing support. Raising awareness, improving treatment access, including migraine in the epidemiological surveillance agenda, and exploring new treatment strategies are all part of improving migraine care. Public awareness of migraine as a neurological condition is growing in the GCC countries, with increased advocacy and educational efforts aimed at reducing stigma and improving understanding. Cooperation among GCC countries can bridge the gaps in migraine care.
Article highlights
Migraine burden in the Middle East is an emerging public health focus.
In GCC countries, patients with migraine are managed by a network of healthcare professionals composed of three levels: primary care physicians, general neurology clinics, and headache clinics.
To improve the care of migraine patients, we should improve patient education and awareness of migraine, improve the education of general practitioners, increase the number of headache specialists and specialized headache clinics, and improve the role of nurses in caring for migraine patients.
Most GCC countries have access to a broad spectrum of migraine medications, including simple pain relief in addition to prescription drugs like triptans, BoNT-A injections, and monoclonal antibodies.
Footnotes
Disclosures
The authors have no conflict of interest for this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.